
Abstract
Introduction
Impaired masticatory function, defined as the inability to chew harder foods effectively, may be a marker of overall health in older adults (Kimble et al. 2022). It results from tooth loss and may result in poorer nutritional intake, systemic inflammation, and health complications (Kimura et al. 2013). While tooth loss is independently associated with increased mortality risk (Koka and Gupta 2018; Nakazawa et al. 2023; Kiuchi et al. 2024), the specific contribution of impaired masticatory function to mortality risk has received less attention.
Several pathways have been proposed to explain this relationship. Chewing difficulty can lead to poor dietary intake due to a reduction in the consumption of fiber-rich and protein-dense foods that are essential for metabolic and cardiovascular health (Nowjack-Raymer and Sheiham 2003; D’Aiuto and Donos 2007; Ono et al. 2022). This leads to a decline in muscle strength, exacerbating physical frailty and increasing mortality risk (Xu et al. 2022). Maintaining teeth and replacing missing teeth may promote better nutritional intake and overall muscle strength, contributing to improved health outcomes (Moriya et al. 2012; Matsuo et al. 2021).
This study hypothesized that decreased perceived masticatory function is associated with higher mortality rates among older adults in Singapore. Singapore has one of the most rapidly aging populations, with almost 20% of residents aged ≥60 y in 2017, which is projected to rise to 40% by 2050 (Malhotra et al. 2019). This makes Singapore a valuable setting for investigating aging-related health outcomes with implications for population-level health policies.
While associations provide initial evidence, establishing causality requires an approach that evaluates the impact of modifying the exposure. Therefore, a causal inference approach was used to estimate the impact of modifying perceived masticatory function on mortality. The longitudinal modified treatment policy (LMTP) approach was applied to assess the impact of hypothetical interventions on perceived masticatory function. LMTP is a method that dynamically shifts an individual’s exposure values based on one’s observed exposure levels. This offers a realistic and flexible framework for causal estimation, addressing key limitations of traditional causal models, such as positivity violations and reliance on strict parametric assumptions (Díaz et al. 2023; Hoffman et al. 2024; Miki et al. 2024).
The aim of this study was to assess whether perceived masticatory function was associated with all-cause mortality. A second aim was to determine the impact of perceived masticatory function on all-cause mortality via a causal approach by emulating multiple counterfactual scenarios using the LMTP approach.
Methods
The article was written in accordance with the STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology; von Elm et al. 2008).
Data and Analytic Sample
This study utilized 3 waves of the PHASE data (Panel on Health and Ageing among Singaporean Elderly), a nationally representative cohort of community-dwelling older adults (≥60 y), collected at 3 time points (2009, 2011 to 2012, and 2015; Chan et al. 2019). Participants were selected from a stratified random sample of 8,400 older adults drawn from the national database of dwellings; 1,195 addresses were invalid and excluded. Among those remaining, 2,215 individuals declined participation or were uncontactable. Wave 1 (2009) included 4,990 participants, with 3,103 followed up in wave 2 (2011 to 2012). Mortality data were available in waves 2 and 3 (2015).
Outcome: All-Cause Mortality
The primary outcome was all-cause mortality and was assessed from waves 1 to 3. For participants reported as deceased by next of kin but not recorded in the National Registry of Births and Death, the date of death was determined by next of kin through a decedent questionnaire. If unavailable, it was approximated as the midpoint between the last interview and next-of-kin contact at the next wave. Survival time was calculated in days from baseline to death or censoring.
Exposure: Perceived Masticatory Function
Perceived masticatory function was used as a time-varying exposure between waves 1 and 2. Participants were asked during the interview, “The following foods are ordered from hardest to softest to chew. What is the hardest group you are able to bite and chew?” If participants were unable to respond due to health reasons such as hospitalization, institutionalization, dementia, or hearing and speaking difficulties, their proxies were asked. Response options were grouped by food toughness and chewing muscle activity (Nasu and Saito 2006; Nascimento et al. 2024). A texturometer measured the toughness of local foods commonly consumed by older adults in Singapore, making it easier for participants to understand and relate to the response options, and foods were arranged in descending order of toughness (Appendix Fig. 1).
Perceived masticatory function was assessed in 2 ways: 6-group categorization with increasing difficulty from group 1 to 6; binary classification, where group 1 indicated no chewing difficulty and groups 2 to 6 indicated any difficulty.
Confounders
Confounders included demographic, lifestyle, health, and social variables. Demographic variables included age, sex, ethnicity, education, housing type, and living arrangement. Self-reported smoking status (never and former/current) was also included. Chronic diseases diagnosed by a medical professional included cancer, cerebrovascular disease, and diabetes mellitus (yes/no). Depressive symptoms were measured by the Center for Epidemiologic Studies Depression Scale score, based on an 11-item checklist (Kohout et al. 1993).
Statistical Analysis
Kaplan-Meier survival analysis compared survival probabilities across the 6 levels of perceived masticatory function, and differences in survival distributions were assessed through log-rank tests. A multivariable Cox proportional hazards regression model estimated hazard ratios (HRs) for the association between perceived masticatory function and all-cause mortality. The proportional hazards assumption was evaluated by scaled Schoenfeld residuals, and variables violating the assumption were stratified to ensure validity within each stratum. Collinearity was assessed by variance inflation factor, with values >2.5 indicating multicollinearity.
Confounders included variables measured at wave 1. When the causal impact of perceived masticatory function on mortality was assessed via the LMTP approach, the same baseline demographic variables were included as time-invariant covariates, while time-varying confounders across waves 1 and 2 consisted of smoking status, self-reported diabetes mellitus, cancer, cerebrovascular disease, and depressive symptoms.
The LMTP framework was used to assess the impact of preserving or improving perceived masticatory function on mortality (Díaz et al. 2023) by emulating hypothetical counterfactual scenarios where individuals had higher levels of perceived masticatory function over time (Figure 1). Statistical parameters for each scenario were estimated by targeted maximum likelihood estimation (TMLE) to provide doubly robust estimates (Schuler and Rose 2017). TMLE combines g-computation, which models the outcome conditional on exposure and covariates, with inverse probability weighting, as derived from the propensity score model, to adjust for confounding and censoring. To enhance the flexible nonparametric estimation of these models, the Super Learner algorithm was used (Schomaker et al. 2019). This approach combines multiple predictive methods—generalized linear models, generalized additive models, extreme gradient boosting, and neural networks—into a weighted ensemble to minimize the cross-validated prediction error.

Proposed direct acyclic graph illustrating temporal associations among variables. W (baseline time-invariant covariates): age, sex, ethnicity, education, housing type, living arrangement. L0 and L1 (time-varying covariates): smoking status, self-reported cancer, cerebrovascular disease, diabetes mellitus, depressive symptoms. A0 and A1 (exposures): perceived masticatory function at wave 1 (2009) and wave 2 (2011 to 2012). Y1 and Y2 (outcome): all-cause mortality.
The following hypothetical scenarios of perceived masticatory function preservation were emulated:
Scenario 1: What if individuals who could not chew foods from group 6 retained the ability to chew foods in group 5 at each time point?
Scenario 2: What if individuals who could not chew foods from groups 5 and 6 retained the ability to chew foods in group 4 at each time point?
Scenario 3: What if individuals who could not chew foods from groups 4, 5, and 6 retained the ability to chew foods in group 3 at each time point?
Scenario 4: What if individuals who could not chew foods from groups 3, 4, 5, and 6 retained the ability to chew foods in group 2 at each time point?
Scenario 5: What if everyone had full perceived masticatory function at each time point?
The following scenarios were emulated for individuals who had <28 teeth without a denture and were experiencing some degree of impaired perceived masticatory function, to explore the potential impact of providing them with dentures:
Scenario 6: What if non–denture-wearing individuals were provided with dentures at each time point and improved perceived mastication by a maximum of 1 level?
Scenario 7: What if non–denture-wearing individuals were provided with dentures and improved perceived mastication to the second-highest chewing group?
Scenario 8: What if non–denture-wearing individuals were provided with dentures, which resulted in maximal perceived masticatory function?
Denture use was self- or proxy-reported and referred to removable prostheses. Illustrated scenarios are found in Appendix Figures 1 to 4. The causal estimand was the difference in mortality (by wave 3) between emulated hypothetical scenarios of better perceived masticatory function and the observed reality for the entire sample. Covariate-adjusted effects of perceived masticatory function on all-cause mortality were estimated via the LMTP approach. Counterfactual risk ratios and 95% CIs were estimated to calculate the relative reduction in mortality risk associated with each intervention. The absolute risk reduction and corresponding reduction in mortality per 100,000 people for each intervention were estimated to quantify the absolute impact of preserving perceived masticatory function. Additionally, the population attributable fraction, representing the reduction of mortality attribution to each scenario, was estimated with bootstrapped 95% CIs (1,000 iterations). E-values were calculated to estimate the impact of unmeasured confounding (VanderWeele and Ding 2017).
Missing data were imputed by chained equations (10 datasets; Van Buuren and Groothuis-Oudshoorn 2011) and pooled per Rubin’s rules. Denture data were unavailable for wave 2. If denture status was the same at waves 1 and 3, it was assumed unchanged at wave 2. If it differed, the change was assumed to have occurred by wave 2. All data were conducted in R (version 4.4.2; R Core Team). The
Results
In total, 4,990 individuals were included in the Cox model and LMTP analysis. While 3,103 individuals remained at wave 2, the LMTP approach accounted for deaths (

Flowchart of participants from baseline (2009) to end of follow-up (2015).
The mean ± SD age of the participants at baseline was 72.8 ± 8.1 y. Higher age, female sex, lower education level, living in smaller housing, smoking, poorer mental health scores, the presence of cerebrovascular disease, and diabetes mellitus were significantly associated with the binary perceived masticatory function variable (
An overall 1,094 participants (21.9%) were deceased by the end of follow-up. Perceived masticatory function distribution differed significantly between those alive and deceased (Table 1). There was a significant difference in the unadjusted survival curves among the perceived masticatory function groups. Survival probability was highest for group 1 and decreased progressively across groups throughout the follow-up period. When perceived masticatory function was dichotomized into a binary variable, those with chewing difficulty had a significantly lower probability of survival (Appendix Fig. 5).
Distribution of Baseline (Year 2009) Characteristics of Participants by All-Cause Mortality until December 31, 2015, after Multiple Imputation.
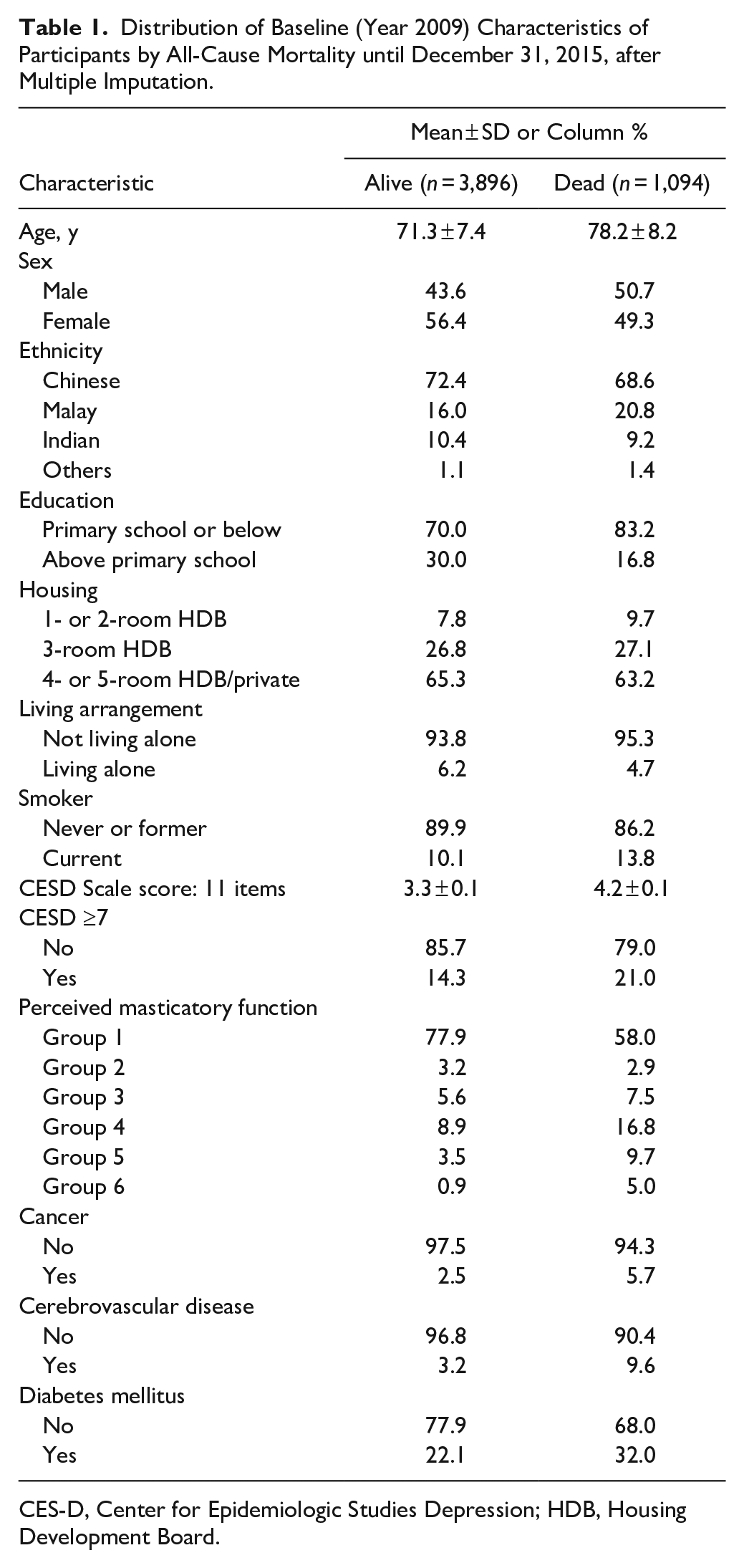
CES-D, Center for Epidemiologic Studies Depression; HDB, Housing Development Board.
For the Cox regression analysis, there was no evidence of multicollinearity (variance inflation factors <2.5). Cancer violated the proportional hazards assumption, with significant scaled Schoenfeld residuals (
Table 2 presents mean expected outcome estimates (TMLE estimates) for the observed data and each emulated hypothetical preventive scenario, based on the Super Learner and generalized linear models. The greatest improvement was observed in scenario 6, where participants retained the highest perceived masticatory function with an increased survival of 3% (relative risk, 1.03; 95% CI, 1.01 to 1.05). Scenario 4, where participants in groups 6, 5, 4, and 3 were shifted to groups 5, 4, 3, and 2, also resulted in significant improvement in survival probability (relative risk, 1.02; 95% CI, 1.01 to 1.04). However, shifting participants in the poorest perceived masticatory function groups (groups 6, 5, and 4) to slightly higher levels (groups 5, 4, and 3) did not produce a significant effect in reducing mortality (scenario 3). The absolute risk reduction was significant for scenarios 4 to 6, with the largest estimated mortality reduction of 2,059 deaths per 100,000 individuals (95% CI, 550 to 3,568) in scenario 6. Based on the population attributable fraction, 0.55% (95% CI, 0.16% to 0.91%) of mortality cases could be prevented for scenario 4, increasing up to 0.70% (95% CI, 0.18% to 1.19%) when individuals preserved the highest level of perceived masticatory function (Table 3).
Survival Probability across Perceived Masticatory Function Groups and Scenarios.

Models adjusted for age, sex, ethnicity, education, housing type, living arrangement, smoking status, self-reported cancer, cerebrovascular disease, diabetes mellitus, and depressive symptoms.
Estimated Proportional and Absolute Reduction in Mortality with Better Perceived Masticatory Function.

Among the 1,663 participants (33.3%) who did not have dentures at wave 1, emulated scenarios where dentures were provided to those with chewing disabilities with <28 teeth (
Discussion
Preserving perceived masticatory function was associated with a slight reduction in all-cause mortality after confounding adjustment. This association remained consistent whether perceived masticatory function was classified as an ordinal or simplified as a binary variable. Emulating scenarios with better-preserved perceived masticatory function demonstrated a modest positive impact of 1% to 3% on survival probabilities, supporting the importance of maintaining oral functionality in promoting longevity among older adults. The largest impact on survival probability was when all participants retained the highest perceived masticatory function, resulting in a 1.03-fold increase in survival probability. This corresponded to an absolute mortality reduction of 2,059 deaths per 100,000 individuals and a 0.70% reduction in mortality attributable to maximal perceived masticatory function preservation. This reduction is comparable to other modest but significant survival benefits observed in different population contexts. For example, in individuals with type 2 diabetes, a 5-kg/m² increase in body mass index corresponded to a 5% reduction in all-cause mortality—a phenomenon referred to as the obesity paradox—which may be explained by greater metabolic reserves and higher muscle mass (Liu et al. 2015).
This study reinforces the importance of masticatory function as a public health issue (Tonetti et al. 2017; Peres et al. 2019). It supports the hypothesis that better masticatory function enables the consumption of a more diverse and nutrient-rich diet, which in turn supports systemic health and reduces mortality risk (Nowjack-Raymer and Sheiham 2003; Xu et al. 2022). Prior studies showed an association between masticatory function and mortality (Onder et al. 2007; Jang et al. 2021; Abe et al. 2024; Du et al. 2025), with one estimating that higher masticatory performance reduces mortality by >15% in older adults (Abe et al. 2024). Another study showed that phenotypic age acceleration mediates this relationship (Du et al. 2025). However, these studies are associative and did not account for time-varying confounders; they also lacked direct causal comparisons and relied on parametric assumptions.
The reported HRs represent an averaged effect over time, which does not capture time-varying effects. To address this, causal inference methods were used to supplement the analyses, allowing for robust estimation of counterfactual survival probabilities. Additionally, the absolute risk differences and population attributable fractions were reported, which provide better interpretability in terms of public health policy impact. The causal estimate presented here is likely conservative, as it is grounded in real-world scenarios by comparing counterfactual estimates against the observed exposure rather than a hypothetical scenario where everyone is uniformly exposed or not exposed. While the estimates are small, they reflect the reality that mortality is determined by multiple factors beyond oral health. Various hypothetical emulations were also utilized to show the variation in outcomes that depends on the degree of scenarios in preserving perceived masticatory function. Estimates incorporated machine learning algorithms to enable flexible modeling of complex relationships for robust estimates.
This study utilized perceived masticatory function, rather than tooth number, as an exposure. Perceived masticatory function is a function of occlusal stability, intercuspation, periodontal health, prosthetic use, and neuromuscular coordination. Although this study did not assess the causal impact of tooth number on mortality, impaired chewing function is a more proximal indicator than tooth number in the hypothesized pathway, leading to inadequate nutritional intake, including reduced consumption of whole grains, nuts, and fiber-rich foods, while increasing consumption of softer, processed foods high in carbohydrates and sodium, thereby contributing to a higher risk of mortality (English et al. 2021; Ramezani et al. 2024). Reduced chewing function from periodontitis may also play a role due to mobility and loss of teeth (Liu et al. 2024; Du et al. 2025) rather than through systemic inflammation (Winning et al. 2021).
This study suggests that achieving maximum chewing function for all older adults may not be necessary, supporting the feasibility of retaining a shortened dental arch (Käyser 1981). The small incremental gains in survival from scenarios 4 to 6 suggest a threshold effect, where improvements beyond a certain point yield diminishing returns. Instead, targeting the more severe chewing disabilities by just 1 level may provide benefits at a population level. This study also found that prosthetic interventions with removable dental prostheses did not alter survival probability. While perceived masticatory function is causally linked to mortality, rehabilitation does not necessarily reduce it.
There are several limitations in this study. First, perceived masticatory function was subjectively assessed, making it susceptible to response, accuracy, reliability, and social desirability biases. Objective methods, such as comminution tests, would have provided more reliable assessments, although this may be infeasible in population-based studies. Nonetheless, the 6-level categorical scale provides more granularity than binary classifications (Tanaka et al. 2018; Watanabe et al. 2024). Second, chewing function is part of a broader set of symptoms of oral frailty, a multidimensional condition contributing to increased mortality (Dibello et al. 2021). However, this study lacked data on oral motor skills, pain, dysphagia, and dry mouth. Moreover, the role of masticatory function within the context of frailty syndrome remains underexplored. Frailty syndrome is characterized by reduced physiologic reserves and diminished overall muscle strength, which may explain its close association with masticatory function. The absence of frailty as a study variable may have limited the assessment of effect modification, where the impact of masticatory dysfunction on mortality could be stronger in frail individuals. Third, while adjustments were made for confounders, unmeasured confounders remain possible. E-values were reported to estimate the strength of the unmeasured confounder needed to explain away the association. Additionally, interventional studies are required to assess whether improving masticatory function in older persons not only reduces mortality but increases quality of life and nutritional adequacy.
The study findings may not be generalizable to other populations due to differences in dietary preferences. Variations in food texture and types of commonly consumed foods across countries, which differ in nutritional value, may influence the relationship between perceived masticatory function and overall health outcomes. Although this study was based on the hypothesis that better perceived masticatory function supports better nutritional status and thereby reduces mortality risk, the lack of significance with denture rehabilitation may be explained by the small number of non–denture wearers with chewing difficulties and the possibility that rehabilitation is not the sole causal pathway. Nutritional intake may also be shaped by individual dietary habits, societal food norms, and access to nutrient-rich soft foods. Furthermore, there was insufficient data to examine cause-specific mortality, which limits the ability to discern whether certain causes of death are more strongly associated with perceived masticatory function while others may be unrelated. Additionally, alternative pathways linking perceived masticatory function to cognitive health and reduced mortality warrant further investigation. The dataset also did not include information on the presence of fixed prostheses or the condition of existing natural teeth. As such, we were limited to modeling scenarios based on the available variables and could not emulate more specific treatment pathways. Fixed prostheses may improve perceived masticatory function more than removable prostheses, potentially leading to greater mortality risk reduction. However, the magnitude of this effect depends on the prevalence of such rehabilitations in the population, and any additional benefits must be weighed against their higher costs.
Conclusion
Worsened perceived masticatory function is associated with increased mortality in older adults. However, the causal effect is modest. Nonetheless, health policies that support chewing function may contribute to longer life expectancy in Singapore.
Author Contributions
J.R.H. Tay, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; U. Cooray, contributed to conception, design, data acquisition, analysis, and interpretation, critically revised the manuscript; A. Chan, M.S. Tonetti, G.G. Nascimento, M.A. Peres, contributed to design, data analysis and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345251363851 – Supplemental material for Perceived Masticatory Function and Mortality: A Causal Study
Supplemental material, sj-docx-1-jdr-10.1177_00220345251363851 for Perceived Masticatory Function and Mortality: A Causal Study by J.R.H. Tay, U. Cooray, A. Chan, M.S. Tonetti, G.G. Nascimento and M.A. Peres in Journal of Dental Research
Footnotes
Declaration of Conflicting Interests
Funding
Ethics Committee Approval
ORCID iDs
Availability of Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.