
Abstract
Community-based models of cannabis cultivation, distribution, and consumption have been documented across Europe, North America, South America, and New Zealand since the 1990s (Decorte et al., 2017; Jansseune et al., 2019; Pardal, 2016, 2020, 2023; Queriolo et al., 2016; Reiman, 2014). These models include cannabis clubs (including cannabis social clubs, cannabis buyers clubs, and cannabis compassion clubs), cannabis dispensaries, and cannabis distribution projects. All three models of cannabis clubs share similar characteristics in that they are nonprofit, driven by cannabis users, rely on a membership or intake system, and supply members with low-cost and high-quality cannabis for their personal use (Belackova et al., 2016; Belackova & Wilkins, 2018). Historically, cannabis clubs were developed to meet the needs of people who use cannabis for therapeutic and/or recreational purposes (Feldman & Mandel, 1998; Parés-Franquero et al., 2019). Cannabis dispensaries, on the other hand, are more akin to community pharmacies or storefront retailers. Many were introduced to help people access medical cannabis, whether authorized by a government-run medical cannabis program or not (Capler et al., 2017; Valleriani et al., 2020). It is important to note, however, that dispensaries and compassion clubs are sometimes used interchangeably in the Canadian literature. Cannabis distribution projects are more recent and unique to the Canadian context (St. Pierre et al., 2022; Valleriani et al., 2020). They provide cannabis products as safer alternatives to the unregulated poisoned opioid supply, without barriers and restrictions, and rely exclusively on grassroots-level donations and distribution efforts (St. Pierre et al., 2022; Valleriani et al., 2020).
Community-based models were born out of three types of policy problems. First, to address supply gaps and challenges created by prohibition, de facto decriminalization in the absence of legalization, and legalization (Decorte & Pardal, 2020). For people who use cannabis for therapeutic purposes (CTP), for instance, these models offer a middle-ground option between an underground market that does not meet their unique needs and government-run medical cannabis pathways that are overly cumbersome and restrictive (Valleriani, 2022). Second, to offer a range of cannabis products to people who use CTP and who have historically been excluded from and underserved by the government-run medical cannabis programs. For example, cannabis dispensaries and compassion clubs played a pivotal role in filling persistent gaps in the Canadian medical program, which relied heavily on physician gatekeeping and limited rather than expanded access to CTP (Belle-Isle et al., 2014; Capler et al., 2017; Capler & Bear, 2023; Fischer et al., 2015, 2020; Lucas, 2008, 2009, 2012; Ng et al., 2022; Valleriani, 2022; Walsh et al., 2013). Third, to implement a harm reduction and substitution tool in the context of an overdose crisis fueled by a highly toxic illicit opioid supply (Valleriani et al., 2022). Overall, community-based models share similar goals in that they seek to provide direct and low-threshold access to low-price and high-quality cannabis products while also offering education, support, and a sense of community (Decorte, 2015; Feldman & Mandel, 1998; Hathaway & Rossiter, 2007; Lucas, 2009).
Studies conducted on community-based models of cannabis cultivation, distribution, and consumption have documented several benefits. These models generate public health benefits by way of quality control, product information, membership or intake process (e.g., age), decreased public use, and promotion of responsible use (Belackova et al., 2016; Capler et al., 2017; Pardal, 2016; Parés-Franquero et al., 2019; Valleriani, 2022). They also increase access to education and guidance, which in turn, promotes informed decision-making and can reduce potential harms (Belackova et al., 2016; Capler & Bear, 2023; DeAngelo, 2015; Hathaway & Rossiter, 2007; Parés-Franquero et al., 2019; Subritzky, 2018). Moreover, these models have social benefits by creating opportunities for mutual aid, contributing to a sense of belonging, and increasing access to community resources and activities, as well as fostering a broader sense of healing, connectedness, and spirituality (Capler & Bear, 2023; DeAngelo, 2015; Feldman & Mandel, 1998; Hathaway & Rossiter, 2007; Lucas, 2009; Subritzky, 2018; Valleriani, 2022). Finally, recent studies suggest that community-based models of cannabis cultivation, distribution, and consumption have a role to play in scaling up cannabis substitution approaches amid the opioid overdose crisis by improving pain management, increasing rates of injection cessation, and contributing to improved treatment outcomes and adherence (Chayama et al., 2021; Lake et al., 2019; Lucas et al., 2021; Mok et al., 2021; Reddon et al., 2020; Socias et al., 2021; St. Pierre et al., 2022; Valleriani et al., 2020; Voon et al., 2018).
Community-based models of cannabis cultivation, distribution, and consumption tend to operate outside existing legislation and regulations (Decorte, 2015). These models have been historically “tolerated” by authorities and, as such, have always existed in legal limbo and have episodically faced raids, seizures, shutdowns, and legal proceedings (Decorte, 2015; Hathaway & Rossiter, 2007). Jurisdictions that have legalized cannabis have approached community-based models in two ways. In Uruguay, for example, nonprofit self-managed cannabis clubs have been included in the cannabis legislation and are regulated by the government (Decorte et al., 2017). Membership is based on age and a monthly fee. People who use CTP are allowed to join. On-site consumption is permitted. In contrast, Canada's cannabis legislation (the Legalization in Canada has had a stronger ability to dismantle and suppress the Compassion Club model than prohibition ever did. By removing the legal grey area, legalization either pushed Compassion Clubs fully inside a regulatory framework that excluded their core values, or it pushed them completely outside the zone of tolerance they had previously inhabited (p. 200).
In the province of British Columbia (BC), where we conducted our research, long-standing community-based models that had been operating since the 1990s (e.g., British Columbia Compassion Club Society
1
and Vancouver Island Compassion Society
2
) were forced to close their doors following cannabis legalization because they faced government sanctions. Others, like the Blue Door dispensary, recently closed after being raided
3
by BC's Community Safety Unit (CSU)—the unit responsible for compliance and enforcement of the
Unlike other jurisdictions (Decorte et al., 2017), designated cannabis consumption spaces that allow indoor smoking are not permitted in Canada. Prior to legalization, concerns were raised by members of the Task Force on Cannabis Legalization and Regulation (Health Canada, 2016) about the disproportionate impact of smoke-free regulations that prohibit indoor smoking
The purpose of this paper is to present the findings of an instrumental case study of VCBC. Our main objective was two-fold.
The Case: VCBC
Founded in 1996, VCBC was modeled after the original San Francisco Cannabis Buyers Club. The San Francisco Cannabis Buyers Club was opened by Dennis Peron in 1991 to make medical cannabis available to people diagnosed with AIDS and people living with other chronic health conditions such as glaucoma, arthritis, and neurological disorders (Malott, 2009). By 1996, when VCBC opened, Peron and his small team were serving 12,000 members (Malott, 2009). VCBC started as a small grassroots project to provide compassionate access to cannabis to people living with chronic illnesses and symptoms (Smith & Kittel, 2019). In 2001, it secured the first location to provide members with a storefront experience and a consumption space. It has continued to do so despite having to move to another location in 2002 and more recently, in February 2023. In 2012, it became a registered nonprofit society governed by a board of directors (Smith & Kittel, 2019). Working with unregulated small-scale growers and collecting donations, VCBC was recording an average of $4,500 in daily sales in the year leading to cannabis legalization.
At the time of writing, VCBC staff served an average of 8,000 members in-person and online (J. Kittel, personal communication, March 30, 2023). Applying for a membership is free. However, each applicant is required to complete an application form, provide proof of condition and/or recommendation from a healthcare provider, and submit a copy of a photo ID. This means that all members have been screened for age requirements (19 years and older in BC) and health requirements. They have also agreed to a basic code of conduct (e.g., infection prevention measures, no scent policy, and tolerance zero for disruptive and disrespectful behaviors toward staff and other members). VCBC members have access to a comprehensive menu of affordable and high-quality cannabis and cannabis products. Cumulating more than two decades of experience in making cannabis products, the club offers products such as capsules, suppositories, topicals, and high-THC edibles. VCBC prices are more affordable than legal market prices. For example, a prerolled joint at VCBC is $3 below current BC market prices.
4
VCBC dried flower ranges from $6 to $8 per gram, whereas market prices can go up to $13 per gram.4 High-THC (75 mg) cookies, which have proven particularly helpful for members with severe pain,
5
sell for $2.50 each. In comparison, a cookie containing 10 mg of THC (the maximum dosage currently allowed under the
The Box, VCBC's consumption space, was been accessible to members for more than two decades. In 2016, VCBC was granted an exemption
6
from the municipal government under section 6(c) of its Cannabis-Related Business Regulation Bylaw to allow on-site consumption. As VCBC founder Ted Smith writes7: The exemption granted to the VCBC is the first of its kind in the country but it is very clear every city in Canada should have spaces for patients to quietly consume their medicine protected from the weather, thugs and police harassment. As we march forward into a legal scheme, let us hope all levels of government work together to help manage these safe inhalation facilities.

The Box (Smith & Kittel, 2019).
As we were conducting our case study, BC launched a round of public consultations to determine whether consumption spaces should be permitted (Ministry of Public Safety and Solicitor General, 2022a). The consultations were limited to recreational consumption and they excluded indoor smoking (and vaping). Nonetheless, survey respondents did indicate an interest in and support for indoor consumption spaces for people who smoke cannabis (Ministry of Public Safety and Solicitor General, 2022b). Among survey respondents who reported consuming cannabis, concerns about consumption spaces were notably lower than among those who did not consume cannabis (Ministry of Public Safety and Solicitor General, 2022b). Likewise, perceived benefits were higher among respondents who reported consuming cannabis than those who did not. Interestingly, a little over a third of the 16,092 respondents reported difficulties in accessing a space to smoke (or vape) because of provincial regulations, municipal bylaws, and strata and tenancy agreements (Ministry of Public Safety and Solicitor General, 2022b).
VCBC has a long history of legal victories for the rights of people who use CTP. Prior to legalization, it faced several raids by law enforcement and was successful in arguing that CTP is protected under the
After the
Study Design
Case study methodology as defined by Stake (1995, 2005) offers a flexible approach to exploring and describing a particular case in its real-life context. The case can be defined as an individual, a group, a program, a city, a country, or a particular phenomenon of interest (Stake, 1995, 2005). Stakes (1995, 2005) identifies three types of case studies: intrinsic, instrumental, and collective (or multiple). An intrinsic case study is undertaken to analyze the particularities of a unique case and develop a better understanding of this case alone (Stake, 1995, 2005). In contrast, an instrumental case study is primarily undertaken to examine a case that can provide insights into a broader phenomenon (Stake, 1995, 2005). When this approach is extended to multiple cases, it becomes a collective case study (or multiple case studies; Stake, 1995, 2005). Case study research starts from a simple yet complex question: “what can be learned from the single case?” (Stake, 2005, p. 443). For this study, we identified that VCBC and its consumption space could help us learn more about the experience of people who smoke CTP in a designated community space against a backdrop of cannabis legalization and the “slow eradication of compassionate access to cannabis.” 8
Our case study was developed collaboratively with VCBC over the summer of 2021, during a period of great uncertainty for VCBC related to the pandemic and its legal standing. The study design was constrained by several contextual factors and informed by preparatory fieldwork at VCBC and consultation with the VCBC leadership team. First, it was understood that VCBC members were particularly vulnerable to COVID-19 and the safest way to collect data would have to be prioritized (Sevelius et al., 2020). Second, because The Box was temporarily closed, we had to find ways of reaching VCBC members when they came to VCBC in-person and when they received VCBC electronic communications. Third, the uncertain context and urgency of documenting the experience of members in the face of a possible permanent closure required flexibility and creativity. For all these reasons, we decided to conduct a descriptive survey that a convenience sample of VCBC members could complete online or using a hard copy. Case studies typically draw on multiple sources of data such as interviews, questionnaires, observations, documents, and so forth (Stakes, 1995, 2005). Like many other researchers conducting research during the COVID-19 pandemic (Krause et al., 2021; Sevelius et al., 2020; Shinew et al., 2022), we had to turn to other sources of data (e.g., news stories, VCBC documents, court documents, virtual discussion with VCBC leadership, and grey and scientific literature) to inform the survey development, contextualize the study and its findings, and open the analysis to conceptual inquiry.
Survey research provided opportunities to gather data in real-time during the COVID-19 pandemic, but it is not without limitations (Hlatshwako et al., 2021). In designing the study and survey, we used the following strategies to increase rigor and participation (Hlatshwako et al., 2021). We developed the survey with questions drawn from prior surveys of medical cannabis use (Walsh et al., 2013) and added questions related to The Box and its closure due to the COVID-19 pandemic. An interdisciplinary panel of experts from public health, psychology, nursing, social work, and policy reviewed the final draft of the survey. The leadership team at VBCB also provided input and ensured that the questions were written in a way that was clear and accessible to members. The final version of the survey had 34 questions covering four domains: demographics, cannabis consumption, access to and use of The Box, and the impact of a temporary closure of The Box due to COVID-19. We used an open-access survey platform and organized the questions to optimize flow. Providing a hard copy option was important to address the technology divide that became apparent during COVID-19 and thus, increase participation among VCBC members who are structurally vulnerable (e.g., precariously housed; Sevelius et al., 2020). Hard copies also provided a way for members with underlying health conditions and increased vulnerability to COVID-19 to pick up a survey at the same time as their cannabis products and then return it at their next visit—as opposed to being forced to fill out the survey on-site and spend more time in the shared space. Finally, we used existing electronic communication channels to recruit members for the survey who were using The Box before its temporary closure. This form of communication was important, especially for members who switched to online ordering during the pandemic.
Data Collection and Analysis
After securing ethics approval, an invitation with an online link to the survey was sent to all VCBC members and also shared via VCBC's communications channels (e.g., social media and website until February 14, at which point the website was taken down by the CSU). Recruitment posters were displayed at VCBC, and paper copies of the survey were available to pick up or to fill out on-site. Completed hard copies of the survey were dropped into a locked box and picked up weekly by the lead researcher. Respondents were eligible to participate if they self-identified as VCBC members, used CTP, accessed The Box, and were able to complete the survey in English. Given the VCBC membership application process, which we describe above, we did not have to screen potential respondents for age requirements (19 years and older in BC) and health requirements. We recorded consent at the beginning survey and then asked respondents to answer mandatory questions to confirm eligibility. The rest of the survey questions were not mandatory. Respondents could opt to skip a question and continue with the survey. They also had the option of entering a draw for a $25 cash prize or a $25 VCBC gift card at the end of the survey.
The survey was open for responses between January and March 2022 and was completed by 104 respondents (
Descriptive statistics were generated from the survey data (Thrane, 2022). For Likert scale scores, we opted to use the weighted averages available via the survey platform, meaning that the highest the score on the Likert scale the more weight it was given in the calculation of the average (i.e., each score on the scale did not carry the same weight; Lavallée & Beaumont, 2015). Using the Likert scale findings and the sources of data collected as part of the case study, which we detailed above, we also identified three conceptual avenues that can inform future research and policy-making. This is consistent with our overall objective for this case study which was to think more broadly about the experience of people who smoke CTP and the role of cannabis consumption spaces.
Results
The results section is divided into two parts. The first part describes the sociodemographic and socioeconomic characteristics of respondents, followed by their cannabis consumption and overall experience accessing The Box. The second part identifies three conceptual avenues that are then carried over into the discussion.
Descriptive Results
Sociodemographic and Socioeconomic Characteristics
58% (
Sociodemographic and Socioeconomic Characteristics.

Gender categories were aggregated to protect the confidentiality of respondents.
Select all that apply questions.
When asked about their annual income, 44% (
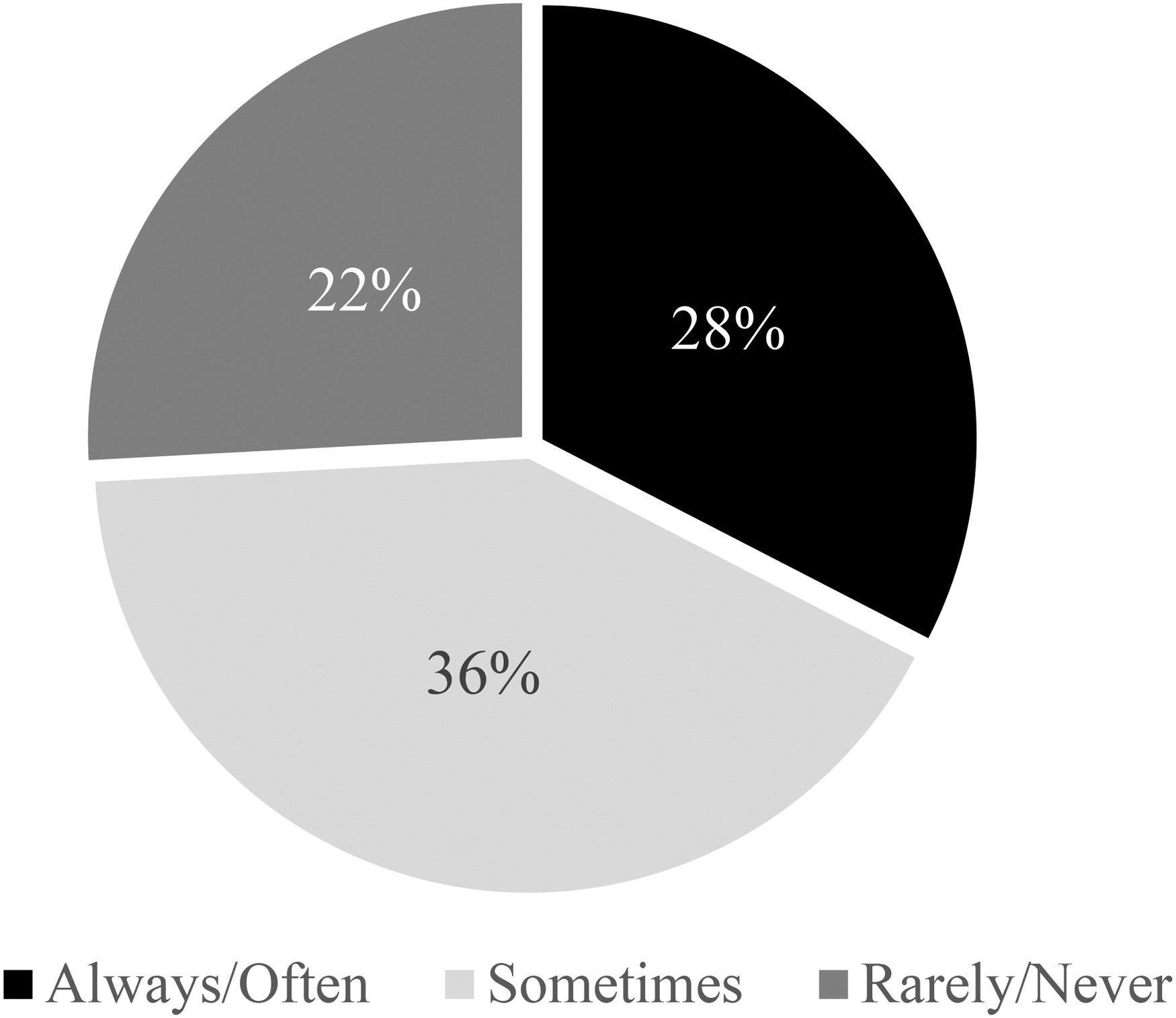
Affordability of cannabis.
Cannabis Consumption
Table 2 summarizes the information collected about respondents’ cannabis consumption including frequency, reason(s), preferred modes of consumption, and amount used. Frequency was reported according to monthly, weekly, and daily consumption. 73% (
Cannabis Consumption.
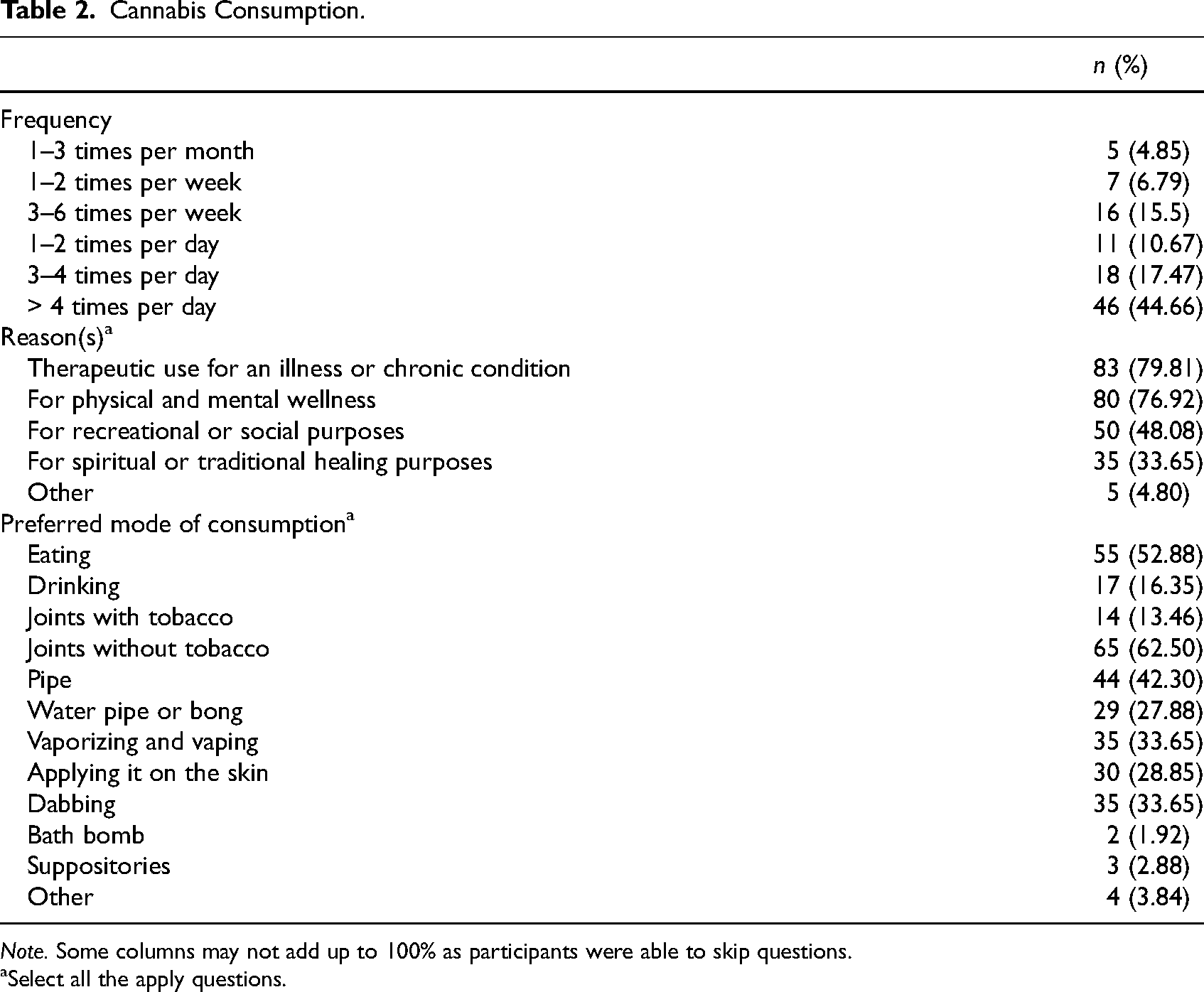
Select all the apply questions.
The most to the least preferred mode of consumption included: smoking, ingesting (eating or drinking), and topical application (lotions or bath bombs). Of the modes of smoking, the three most commonly reported were smoking joints without tobacco (63%,
Experience Accessing the Box
We asked respondents how often they accessed The Box before its temporary closure, what equipment they used (if any), how much they smoked during a regular visit, why they smoked in The Box, and how beneficial the space had been to them (see Table 3). In terms of frequency of visits, the sample was split into three groups: (a) monthly visitors (31%,
Experience Accessing The Box.
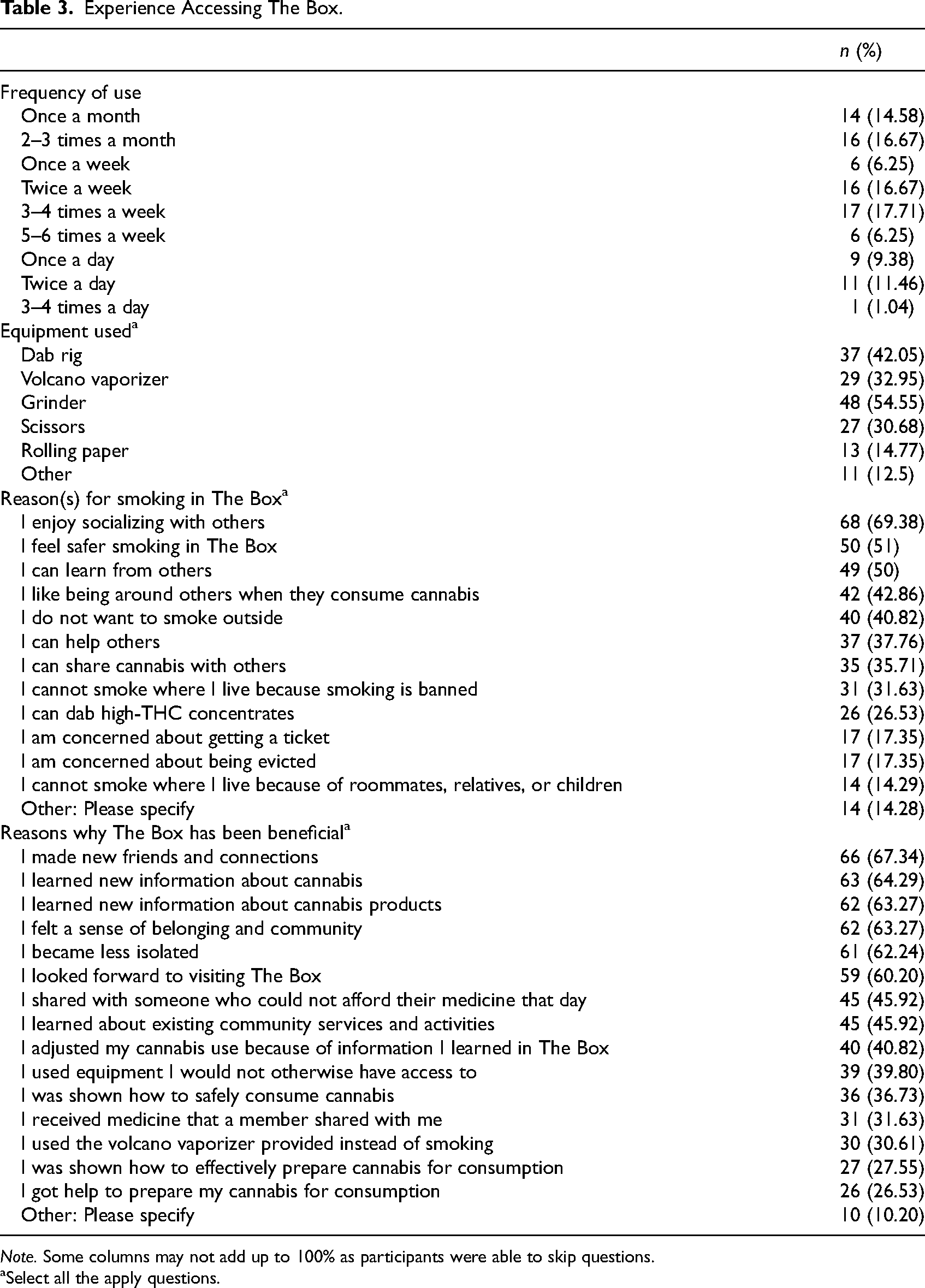
Select all the apply questions.
Socializing was a common reason (69%,
The main benefits of The Box were: (a) breaking isolation and building community, (b) learning something new and adjusting cannabis use, and (c) reducing potential harms associated with cannabis. Respondents reported making new friends and connections (67%,
Conceptual Avenues
Cannabis is Therapeutic, and so is The Box
As pointed out above, the reasons why respondents consumed cannabis varied and were not exclusively therapeutic in a medical sense (i.e., symptom relief). Managing an illness or chronic condition was common but so was physical and mental wellness. Recreational or social use, which privileges enjoyment and pleasure, was also deemed important. Finally, for a third of our sample, cannabis was used for spiritual or traditional healing purposes as well. The Box offered a place where cannabis could be consumed with all these reasons in mind. For example, when we asked respondents to use a Likert scale of 1 to 10 (10 being the most important and 1 being the least important) to rank the importance of The Box on their mental health, physical health, social life, and spirituality (Figure 3), they reported the following: Mental health was the single most important contribution of The Box with a weighted average of 6.85. Social life was ranked second at 6.54. Importance to physical health was ranked third with a weighted average of 6.24, followed by spirituality with a weighted average of 5.83.

Importance of The Box.
Considering that smoking was the preferred mode of consumption among our respondents, it makes sense that accessing a place to smoke would be deemed important, especially when options to smoke indoors and outdoors might be limited. However, our findings suggest that The Box was more than “just a place to smoke” for respondents. For example, mental health and social life ranking higher than physical health are indicative of space-specific effects that merit further inquiry. In other words, if the sole purpose of a cannabis consumption space is to smoke cannabis (as a medicine), other dimensions of the consumption experience
If not in The Box, then Where
When we asked about the impact of the temporary closure of The Box due to COVID-19 using the same Likert scale design (Figure 4), one respondent used the text box and described it as follows: “It was a loss. A social, medicinal loss.” Consistent with the above findings, the

Impact of closure.
Given that smoking in The Box generated benefits that exceeded those associated with smoking cannabis (as a medicine), that smoking was the primary mode of consumption for respondents, and that smoking posed real challenges (e.g., smoking bans) and risks (e.g., eviction), we see two potential conceptual avenues to explore. First, it is important to untangle the broad concept of “people who use CTP.” Studying those who primarily or exclusively
Feeling (Un)Safe in The Box
We asked respondents to rank how safe they felt in The Box on a Likert scale of 1 to 10 (10 being the safest and 1 being the least safe). The responses yielded a weighted average of 8.75, with 82% (
First, we see a need to dive more deeply into the concept of safety. For example, The Box may feel like a “refuge haven” (an expression used by a respondent) because it offers protection from the risks of smoking outdoors (e.g., ticketing) or in indoor spaces where smoking is prohibited (e.g., eviction). However, the same feeling of safety may not apply
Discussion
Our findings offer important insights into a unique community-based model of cannabis cultivation, distribution, and consumption and a unique group of people who use CTP, both of which are currently located outside the scope of the
First, it addresses a major gap by providing a middle-ground option for people who face numerous structural vulnerabilities and live with chronic illnesses/disabilities whose needs are not met by the government-sanctioned market—a market intended for
Surveying VCBC members allowed us to identify who uses The Box and why they do so. The majority of our respondents identified as cisgendered White men and reported a yearly income of <$40,000. This is consistent with other Canadian studies conducted with people who use CTP (Belle-Isle et al., 2014; Capler et al., 2017; Costiniuk et al., 2019; Lucas 2012; Walsh et al., 2013). Across these studies, 67%–87% of participants identified as cisgendered men, 81%–93% identified as White, and 48%–89% reported a yearly income of <$40,000. In contrast to previous studies, however, our survey generated higher engagement from people who identified as transgendered, nonbinary, genderqueer, and/or Two-Spirit as well as people who identified as Indigenous. While our study design did not include an in-depth exploration of Lesbian, Gay, Bisexual, Transgender, Queer/Questioning, Intersex, Asexual, Two-Spirit (LGTBQIA2S) + and Black, Indigenous, and People of Color (BIPOC) voices and experiences, we see a need for more research to address this gap.
Respondents used The Box because smoking was their preferred (and most effective) mode of delivery and having a place to smoke was important not only to optimize symptom management but also to build meaningful social connections and feel better mentally while seeking refuge from the potential risks of smoking outside (e.g., ticketing) or in places where smoking bans are in effect (e.g., eviction). This is a significant finding for two reasons. One, it is consistent with research dating as far back as the 1990s which found that cannabis clubs worked at the medical–social–mental–spiritual nexus (Feldman & Mandel, 1998; Hathaway & Rossiter, 2007). In other words, the impact of cannabis clubs extends beyond cannabis itself. Second, it makes an original contribution to the existing literature by revealing particular aspects of cannabis legalization that have not been studied to date, namely by conducting a case study of a cannabis club that continues to operate outside the legal framework and exploring the role/importance/contribution of consumption spaces in a context where smoking indoor
When asked about the importance and helpfulness of The Box, more specifically, our respondents reported reasons and benefits that are best interpreted by combining public health, harm reduction, and wellness perspectives. Taken together, these perspectives help us understand why consumption spaces matter to people who
From a
Finally, from a
Our survey had some limitations, some of which are discussed in the study design section. The scope of the study was narrow, the context was in flux amid a pandemic and ongoing enforcement measures (e.g., website closure, risk of raids, etc.), we relied on a survey as a primary data collection method, the survey questions focused primarily on the experience of using The Box, and the sample was a small proportion (8.56%) of a subgroup of VCBC members. In opting for a convenience sample of members with a common experience of (and need for) using The Box, this may have generated a positive bias. However, critiques offered by respondents reflected an ability to recognize the benefits of The Box while also acknowledging its limits. Furthermore, it is important to recognize that members for whom The Box was the only consumption space available may have responded favorably in the hopes of preserving that space in a time of heightened uncertainty. Finally, we cannot claim that our sample was representative of members nor that our findings are generalizable to all VCBC members—or people who use CTP more broadly. As noted above, our sample was consistent with other Canadian studies conducted with people who use CTP; thus suggesting potential transferability.
Conclusion
Our study adds to the literature on cannabis clubs and raises important issues related to cannabis legalization, the role of community-based models of cultivation, distribution, and consumption, and the impact of accessing (and potentially losing access to) a consumption space such as The Box. Overall, we consider that VCBC and its on-site consumption space offered a useful case study to make “real-time observations” (Watson et al., 2019) about cannabis legalization as it unfolds over time and across jurisdictions. Given that the BC government, which is tasked with enforcing the