
Abstract
Keywords
Introduction
In the context of prohibition, the unregulated drug supply in Canada (and beyond) is constantly evolving to evade law enforcement crackdowns, leading to an increasingly toxic supply with catastrophic and avoidable increases in morbidity and mortality among people who use drugs. One of the main repercussions of prohibition has been a rise in adulterants, including a wide array of pharmacological and psychoactive compounds and chemicals, which has resulted in an unpredictable drug supply (Payer et al., 2020; Russell et al., 2023).
Since the beginning of the COVID-19 pandemic in particular, benzodiazepines, a central nervous system depressant, have become a prominent feature in the unregulated drug supply across North America (McNeil et al., 2022; Russell et al., 2023). The rise of benzodiazepines within the supply can be attributed, in part, to the increased border crackdowns imposed during COVID-19 that forced many to turn to less familiar sources due to fewer drugs entering the country, as well as the pervasive criminalization and prohibition that characterizes the North American approach to drug policy more broadly (Ali et al., 2021; Canadian Centre on Substance Use and Addiction, 2020; McNeil et al., 2022; Nguyen & Buxton, 2021; Schneider et al., 2023). In British Columbia (BC), Canada, for example, the detection of benzodiazepine-like substances spiked from 15% in July 2020 to 52% in January 2022 (BC Coroners Service, 2023; Foreman-Mackey et al., 2023). Unregulated benzodiazepines typically contain much stronger derivatives or analogs (e.g., etizolam) of regularly prescribed benzodiazepines used for anxiety or sleep aids (e.g., alprazolam, lorazepam, and diazepam); these are commonly mixed with opioids (e.g., fentanyl) and sold either as “benzodope” or “down”, with some people who use drugs purchasing benzodiazepines unknowingly or unreliably (Bonn, 2023; Crackdown, 2022; Russell et al., 2023). For those who regularly use opioids, the volatile supply means that in some situations “benzodope” is what is available.
Regardless of the evolving supply, many people have sought and continue to intentionally seek out benzodiazepines due to the euphoric, pleasurable, and anxiety-reducing effects, combined with the fact that benzodiazepines extend the half-life of fentanyl to produce an effect more akin to heroin (Bonn, 2023). For others however, especially those who are using benzodiazepines unknowingly or in unpredictable quantities, benzodiazepines may have profound sedative effects that can include confusion, dizziness, drowsiness, passing out, and memory loss or anterograde amnesia (e.g., “benzo blackouts”), while increasing susceptibility to more complex overdose (Liebrenz et al., 2016; Russell et al., 2023). Despite the influx of benzodiazepines within the unregulated drug supply, there remains a critical lack of understanding regarding the gendered impacts of this shift, including vulnerability to gender-based violence (GBV) among women and gender minorities who use drugs (WWUD).
Structural, Symbolic, and Everyday Violence and Experiences of WWUD
GBV refers to the harmful acts directed at a person or persons based on their gender identity, gender expression, or perceived gender, and can manifest as physical, sexual, emotional, and/or psychological violence (Walsh et al., 2015). Intersecting modes of economic and social marginalization, criminalization, racist, settler colonial logics, and drug war violence shape WWUDs’ experiences of GBV, with factors such as heightened surveillance and interactions with police—who are often also perpetrators of GBV—further increasing WWUDs′ exposure to GBV (Birgin et al., 2022; Boyd et al., 2018; Collins et al., 2020a; Collins et al., 2020b; Gilbert et al., 2015; Goldenberg, 2020; Harris et al., 2024; Knight et al., 2014; Ohtsuka et al., 2023; Shannon et al., 2008). Trans and two-spirit people face GBV at heightened rates due to the added layers of gendered discrimination and exclusion embedded within many facets of our societal fabric (Martin & Walia, 2019).
Concepts of structural, symbolic, and everyday violence are useful in examining WWUDs’ experiences of GBV. Structural violence refers to how social structures and institutions sustain, perpetuate, and routinize inequalities and resulting harms. Analyses applying this lens have highlighted how macrocontexts (e.g., drug prohibition, gender subordination, racism, systemic social exclusion, economic marginalization, etc.) have an impact on microcontexts (e.g., WWUDs’ individual drug use experiences), shaping the health and safety of WWUD, including their exposure to GBV (Boyd et al., 2022; Farmer, 2009; Galtung, 1969; McNeil et al., 2014; Scheper-Hughes & Bourgois, 2004; Shirley-Beavan et al., 2020).
Internalization of social–structural subordination because of its ubiquity and resulting self-blame is understood as symbolic violence (Bourdieu, 1979). Structural and symbolic violence commonly presents itself as a form of everyday violence, a term that refers to the normalization of violence that is often embedded within gendered relations and rendered invisible due to its pervasiveness (Bourdieu, 1979; Scheper-Hughes & Bourgois, 2004). Such experiences of everyday violence in the lives of WWUD have been highlighted in past works, underscoring how gendered power dynamics are regularly expressed through violence and often inflicted by police, intimate partners, or unknown people in community, and compounded by criminalization (Boyd et al., 2018; Collins et al., 2020a; McNeil et al., 2014).
GBV among WWUD is an urgent public health concern given its prevalence and normalization, and direct association with drug war violence. Experiences of GBV in the context of the unregulated drug toxicity crisis have been shown to increase the likelihood of overdose for WWUD (Ataiants et al., 2022; Collins et al., 2020a; Gilbert et al., 2022; Goldenberg, 2020; Knight, 2017). As already alluded to, ongoing systems of settler colonialism, as well as the racist and imperialist logic in which prohibition was founded, has meant that this link is especially pronounced for Indigenous or otherwise racialized WWUD (Gordon, 2006; Lavalley et al., 2018). Indigenous women in Canada experience physical violence at 8 times the rate as non-Indigenous women, while also making up 36% of BC's fatal overdoses in 2022—a rate 8.8 times higher than non-Indigenous women (First Nations Health Authority, 2022; Martin & Walia, 2019; Thumath et al., 2021). Notably, Indigenous women and two-spirit people have repeatedly attempted to raise the alarm on the disproportionate levels of GBV they face within Canada, combatting the normalization of this reality (Martin & Walia, 2019).
WWUD have also reported gendered barriers to accessing harm reduction services, including overdose prevention sites. These are spaces that are both regularly surveilled by police and dominated by men, with some WWUD experiencing exclusion, intimidation, and harassment while accessing these sites, including being confronted by police and/or violent actors in community who they have been previously victimized by (Boyd et al., 2018, Collins et al., 2020b). This has resulted in many WWUD voicing concerns regarding safety and the threat of GBV in and beyond such service delivery settings, reducing the likelihood of WWUD utlizing these sites (Austin et al., 2023; Boyd et al., 2018; Collins et al., 2020b; Harris et al., 2024; Martin & Walia, 2019; Shirley-Beavan et al., 2020; Värmå Falk et al., 2020).
While past research has drawn important connections between drug prohibition, gender, and experiences of violence, what remains underexplored is the various impacts that the influx of benzodiazepines in the increasingly volatile unregulated drug supply have on WWUD. Focusing on WWUD who experience intersecting modes of criminalization, our analysis incorporates concepts of structural, symbolic, and everyday violence to evaluate the ways in which which the surge of benzodiazepines in the supply has shaped the health, safety, and experiences of GBV among WWUD in Vancouver, BC.
Methods
For this analysis, we drew on 30 in-depth qualitative interviews with sex workers who use drugs across Coastal BC (Metro Vancouver and Victoria) conducted between 2022 and 2023. This work is part of the AESHA project, a community-based longitudinal cohort and qualitative study that investigates the impacts of social and structural factors on sex worker safety, health, and human rights. The AESHA project has built on collaborations with sex work organizations and has included experiential staff (current/former sex workers) on the project team since its inception in 2010.
Study recruitment was facilitated through longstanding relationships between the research team and sex workers who use drugs. Additional recruitment was supported by individual members of the research team who utilized their personal networks to identify and recruit participants from across Coastal BC. Participants were purposively invited to include a diverse array of experiences and perspectives (e.g., based on sexuality, gender, socioeconomic status, frequency of drug use, types of drugs used, sex work environments, etc.), with snowball sampling also used in some instances where study participants invited others in their community to participate. In order to be included in the study, participants had to be 18 years or older, live in Coastal BC, and identify as someone who used unregulated drugs and engaged in sex work in the last 6 months. All participants were remunerated with a CAD$50 honorarium for their time and expertise. The study holds ethical approval through the University of British Columbia/ Providence Health Care Research Ethics Board.
Interviews were conducted over the phone or at the AESHA project office depending on participant preference and location by two members of the research team (JM, AK). Participants were provided with information about the study and a copy of the consent form prior to the interview. Before beginning the interview, interviewers allowed time to answer any study-related questions and confirm that participants had a complete understanding of the study processes and aims. All participants who agreed to participate provided informed consent prior to the interview. Once the interview was complete, interviewers went through a demographic questionnaire with participants to collect data about characteristics such as housing, gender identity, drug use patterns, and age.
Interviews were supported by a semi-structured interview guide, encouraging broad discussions of (a) drug use experiences and access to harm reduction services; (b) policing and dual criminalization (e.g., drug use and sex work criminalization); (c) experiences with and opinions of prescribed safer supply; and (d) opinions on drug regulation and potential regulatory models. The interview guide was developed based on the existing knowledge of the research team and further refined in consultation with community experts (e.g., women with experience of drug use and criminalization). Notably, all interviews were conducted prior to the implementation of BC's decriminalization approach (Michaud et al., 2024). The interview guide was piloted in the first three interviews, after which it was reviewed and revised based on participants’ feedback to enhance relevancy. The research team met weekly to discuss the interview guide, patterns and variations in the data, and to ensure the data continued to elicit a rich understanding of the topics explored. Interviews lasted for approximately one hour and were audio recorded, transcribed verbatim, and checked for accuracy. All data were organized, stored, and coded in NVivo 12.
The data were analyzed using a thematic approach (Braun & Clarke, 2006). To begin, the research team worked to develop the initial coding framework, which was conceptualized based on key themes reflected in the interview guide, as well as observations made upon reviewing the transcripts and known topics or concepts from the literature. The framework was discussed and refined, and then applied to three transcripts, after which the coding team adjusted and further developed the framework. Once finalized, the coding framework was applied to all interviews. The research team met every two weeks to discuss the coding framework, with the ultimate aim of promoting intercoder reliability. This iterative and rigorous process of coding, discussing, and refining continued until all the data were organized under the final coding framework.
After the initial round of coding, the first author (JM) inductively analyzed participant accounts with a focus on the distinctive ways participants articulated experiences of GBV amid the rise of benzodiazepines in the unregulated drug supply, an issue that was repeatedly emphasized during interviews. These findings were further organized into themes and subthemes and shared with senior members of the analysis team for input and final approval. Emergent themes were analyzed with attention to structural, symbolic, and everyday violence, giving particular focus to, and drawing connections between, the way in which structural violence (e.g., drug prohibition, sexism, racism, criminalization, etc.) and symbolic violence contributed to everyday experiences of GBV in the context of the unregulated drug toxicity crisis. Themes included the influx of benzodiazepines in the unregulated drug supply and everyday experiences of violence among WWUD; the normalization of everyday experiences of violence among WWUD; the rise of benzodiazepines in the unregulated drug supply and the overdose experiences of WWUD; and community care and involvement in the face of structural and everyday violence. These themes are unpacked further within our results.
Results
Drawn from a diverse group of 30 participants from across Coastal BC (see Table 1 for demographic info), participants spoke to the ways in which prohibition, a form of structural violence, impacts the content and composition of the unregulated drug supply, shaping WWUDs’ experiences of GBV amidst systemic gender subordination and misogyny. The rise of benzodiazepines in the unregulated supply in particular was discussed as creating especially dangerous conditions for WWUD due to the increased likelihood of experiencing unwanted sedative effects, including confusion, drowsiness, and memory loss. Our results highlight that, despite discussions of community support and the use of safety strategies, many participants felt especially vulnerable to GBV while either unknowingly using benzodiazepines, or not knowing its potency. Participants also expressed having little recourse due to partial memory loss of the events and experiences of criminalization and police violence. In discussions of these topics, participants spoke to several interconnected themes related to the impacts associated with the rise of benzodiazepines in the unregulated supply, which we outline below.
Participant Demographics (
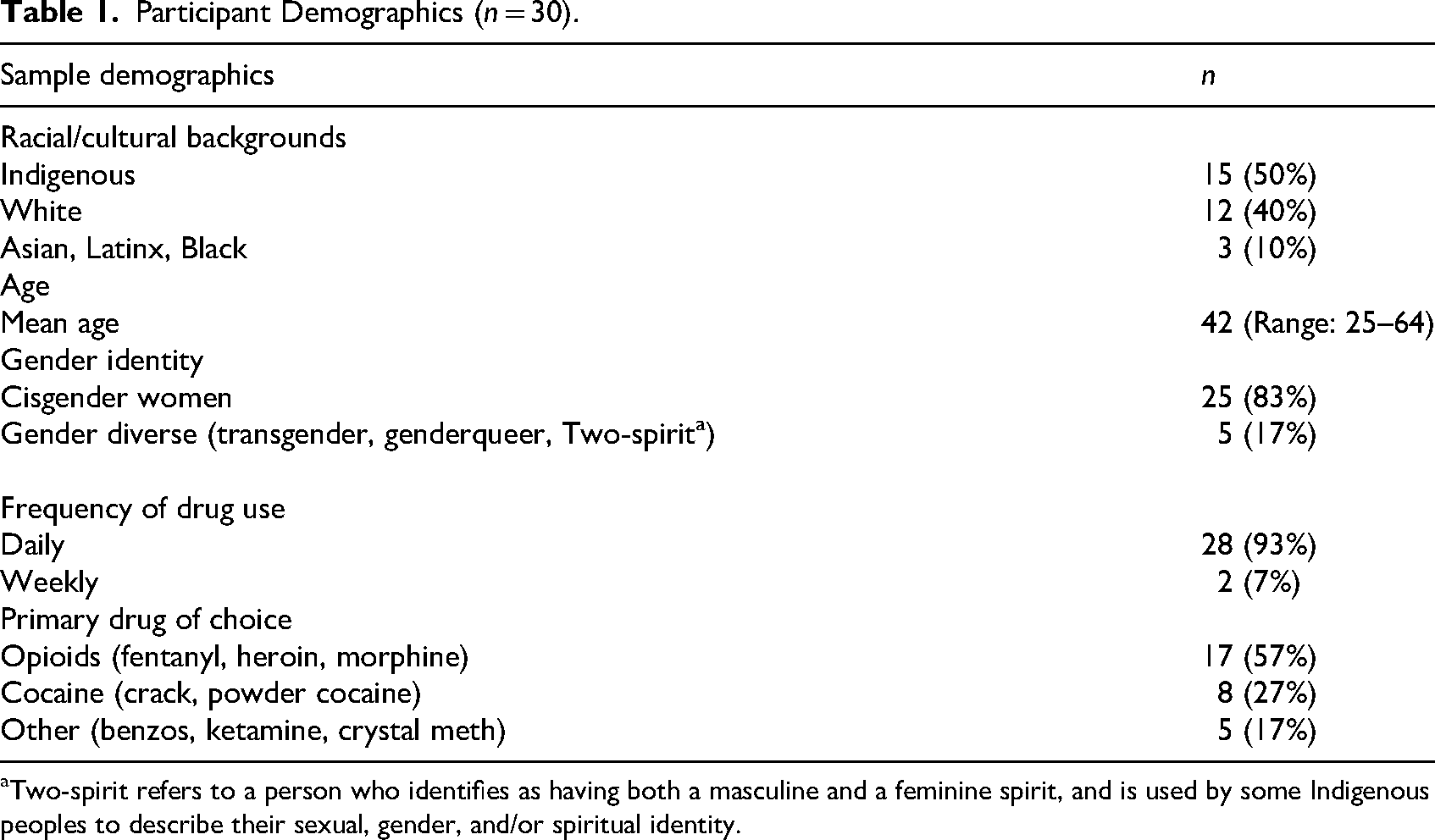
Two-spirit refers to a person who identifies as having both a masculine and a feminine spirit, and is used by some Indigenous peoples to describe their sexual, gender, and/or spiritual identity.
Prohibition as a Form of Structural Violence: The Influx of Benzodiazepines in the Unregulated Drug Supply and Everyday Experiences of Violence Among WWUD
Participants repeatedly underscored the ways in which prohibitionist policies and the subsequent unpredictability of the unregulated drug supply made it exceedingly difficult to discern drug content, negatively affecting WWUDs’ everyday lives. In particular, participants discussed situations in which they were uncertain about what type of substance they were buying, leading some to purchase benzodiazepines or “benzodope” (e.g., benzodiazepines mixed with opioids) when intending to buy, for example, opioids such as fentanyl. The evolution of the supply was described by one participant who stated: “Well, it's going from fentanyl to carfentanyl to benzos, and shit has just been so bad” (Participant 11).
The sudden influx of benzodiazepines in the unregulated drug supply following the COVID-19 pandemic, combined with low benzodiazepine tolerance or familiarity, meant that WWUD were often unprepared to deal with the effects of benzodiazepines, exacerbating the potential for being targeted by violent actors, including strangers, supposed friends, or intimate partners. The word benzo isn’t something that we used very often. It was like, okay what is that? Oh okay, they’re like valium? I didn’t realize they were a big thing […] And now it's like it's this dark word, ‘do you have benzodope or do you have non-benzo [dope]? Are you [dealer] gonna lie about it or not? Because if you do, then my days gonna be sabotaged and I don’t know if I’m gonna have a home, if I’m gonna get robbed. You can lose everything in a day and I see it happen to people. Like, they’re getting beaten, robbed, by their friends, or their supposed friends. It's really scary. (Participant 03)
In the absence of regulatory controls to minimize the far-reaching effects of prohibition and the resulting uncertainty about drug content, WWUD remained susceptible to unwanted benzodiazepine exposure. As outlined by this participant, using benzodiazepines unknowingly can heighten WWUDs’ experiences of physical or sexual assault, or place WWUD in a position where they could “lose everything” due to the exploitative practices of some who weaponize the broader violence of the drug war to their own benefit. The significant social and structural violence endured by many WWUD—shaped by forces such as criminalization, settler colonialism, racism, social exclusion, and gendered surbodination—was described as further exposing WWUD to GBV, theft, and exploitation, perpetuating and normalizing the everyday violence WWUD are confronted with. Notably, as highlighted by the above quote, such experiences had the potential to be profoundly destabilizing for WWUD, particularly those who were living in poverty.
While some participants described unintentionally using benzodiazepines as a result of the volatile supply, many purposefully sought out benzodiazepines due to their myriad positive effects, including reducing anxiety and instilling a sense of calm: “When I take benzos, it makes me feel like everything is OK. They’re kind of like a coping mechanism that I use, honestly […] it's something that's always been helpful” (Participant 25). Despite this, the impacts of prohibition meant that potency was often difficult to determine. Similarly to the discussions around unknown benzodiazepine use, participants spoke to the ways in which the unintended use of high strength benzodiazepines contributed to negative drug use experiences, placing some WWUD in precarious or potentially unsafe positions. The other day I had a fire right across my hall, and […] my place was clouded with smoke. I ended up doing a shot of benzodope, it was supposed to be very light benzos, and I was down and out and, passed out, for the entire day into the evening. I didn’t realize that there was a fire. [My boyfriend] called my boss and said ‘she can’t go to work, she's benzo’d.’ [I was] talking like totally coherent, but my brain wasn’t there. Like I’m functioning, but my brain isn’t there. (Participant 03) Well, I know last year, is when I had those robberies happen [to me after using benzodiazepines] and I think that's because [benzodope] is super unpredictable. Sometimes [my friend] is really worried about me, like she’d text me asking where I am. Sometimes I don’t even know where I am, but I’d go on Google Maps and send a screenshot of the location and just text it, because I’m not in the frame of mind to even look around and know where I am. (Participant 13)
These narratives illustrate that the fluctuating potency of benzodiazepines in the unregulated drug supply may result in experiences of long lasting memory loss, drowsiness, confusion, or other symptoms that can work to heighten WWUDs’ vulnerability to exploitation in different contexts; this includes altered levels of awareness and heightened exposure to various forms of disappearances (e.g., the disappearance of memory, disappearance from public space in order to avoid violence, etc.). Notably, such experiences of reduced awareness, in tandem with the sedative effects of benzodiazepines, were described as potentially increasing WWUDs’ likelihood of being targeted and violently harmed.
For some participants, episodes of intense benzodiazepine-related memory loss lasted from a few hours to several days, leading to the disappearance of long stretches of time. These experiences compounded the stress and fear many endured after the unknown use of benzodiazepines, or exposure to high potency benzodiazepines, making it increasingly difficult for WWUD to piece together what had happened to them. Given the structural context of pervasive gender inequities and subsequent high rates of GBV among WWUD, this type of long-lasting memory loss was identified as being especially concerning (Boyd et al., 2018). This was described by one participant who stated: You have no memory [of] what you did for days, two, three or four days, right. And you think, where could I have been for four days? Where was I? What was happening to me? (Participant 21)
Similarly, others discussed waking up with bruises, missing belongings or articles of clothing, or in an unknown location after being tarteged during a prolonged “benzo blackout”. Such experiences further exemplified how unpredictable benzodiazepine use, enabled by prohibition, had the potential to alter perceptions of time and memory, increasing WWUDs’ vulnerability to violence, especially in situations where participants were isolated and/or unable to lean on support networks for safety.
Sub-Theme: The Effects of Prohibition on Sex Workers Who Use Drugs’ Occupational Health and Safety
For sex workers, the volatile drug supply was described as adding an additional layer of complexity, with the potential to negatively shape occupational conditions. Participants especially underscored that using benzodiazepines in unknown or unpredictable quantities often made it difficult to enact critical safety strategies that strengthen sex workers’ occupational health and safety (e.g., screening clients, working in collaboration with others, etc.) amid ongoing criminalization. One time [after using benzos] I don’t even remember going with this guy. […] I just sorta remember coming back on the train. And I didn’t know what I was doing on the train. And I got off at a station and I had to catch a bus back here [to my home] and I was wondering why I was on the train and I was trying to piece it together. And then my friend said we were doing benzo dope at [X's] place and I decided to go out with this guy that stopped by to pick me up. And I was like holy fuck that's why I was on the train. I did a date. (Participant 01) Hell yeah, [benzos] are a big issue […] you know that they [sex workers] can’t give consent and [they don’t know] what they’re doing or what's going on around them? Like, when you’re on that, you’re in blackout, right, you don’t know what you’re doing. (Participant 24)
As illustrated through the above narratives, the impairment that can be caused after using benzodiazepines unknowingly or at a higher strength than intended can limit the ability for sex workers to adequately control their working conditions or environment, with some reporting having no memory of working at all. This meant that, in a few instances, workers were ripped off or unable to dictate the terms of their transaction (e.g., unsure about where the date took place, if a condom was used, etc.) after using benzodiazepines, increasing vulnerability to occupational violence, including GBV, carried out by predatory people posing as clients. The dangers associated with the memory loss endured by participants in this context were described as being made more complicated by the structural violence sex workers who use drugs face due to their dual criminalization, further limiting access to recourse and undermining safe working conditions, ultimately increasing the likelihood of experiencing more intensified forms of everyday violence and subsequent disappearances (e.g., disappearance from a public space to avoid perpetrators of violence and/or police, more permanent forms of disappearances resulting from physical violence or overdose).
The Normalization of Everyday Experiences of Violence Among WWUDs
Consistent with the previous section, the normalization of WWUDs’ exposure to physical or sexual violence as a result of benzodiazepine-related memory loss was explicitly highlighted by several participants: Because you’re blacking out and you don’t remember what you’re doing, you seem like you’re fine but you’re not fine. You’re not there. You can be walking around, functioning but no one's home at that time. How could [they] not take advantage of you, right? (Participant 03)
While this participant spoke directly to benzodiazepine use and resulting experiences of memory loss, her narrative points to an even broader concern wherein GBV has become a regular part of some WWUDs’ drug use experiences in the context of systemic gender subordination and misogyny. Given the increasingly unpredictable drug supply, the implication that WWUD
Notably, the normalization of violence among WWUD led some participants to blame themselves for the violence they had experienced. “The effects of doing benzos – I tell you benzos destroy [people] […] Because some of the stuff [that happens]….the worse shit [that happens] the worse shame and remorse you go through, right” (Participant 23). This kind of self-blame, which can also be understood as a form of symbolic violence, in tandem with the intense emotional and physical trauma some experienced in the context of extended benzodiazepine-related memory loss, had a profound impact on WWUDs’ mental health and well-being, perpetuating the cycle of violence endured by WWUD.
Prohibition as a Form of Structural Violence: The Rise of Benzodiazepines in the Unregulated Drug Supply and the Overdose Experiences of WWUD
The fear of being taken advantage of or harmed in the context of benzodiazepine-fueled memory loss, drowsiness, or confusion, meant that many of the participants we spoke to preferred to use alone at home. This experience was described by one participant who stated: “I'm actually safer using alone in my suite, than being somewhere and then passing out and getting all my stuff stolen kind of thing” (Participant 13).
Critically however, this is contradictory to the directives given to never use drugs alone due to the crisis-level risk of overdose fueled by prohibition (Government of British Columbia, 2025). It is important to note that, while such directives do not attend to the structural violence of the unregulated drug toxicity crisis and how it engenders everyday violence—as well as skirt government responsibility in meaningfully addressing the central drivers of the crisis—they remain in place given the nature of the current drug supply. Despite this, many WWUD continued to use alone in order to avoid the potential for GBV, disappearing them from public view and increasing their likelihood of experiencing a fatal overdose.
In a few instances, the preference to use alone was furthered by WWUDs’ limited options for recourse following experiences of violence, including assault or theft. As already noted, participants discussed situations in which predatory people would take advantage of the memory loss experienced by WWUD after benzodiazepine use to target them with relative impunity. Contacting police was not an option for participants, with many noting that the police often perpetuated the GBV that WWUD experienced in these situations. For example, participants described instances where the police caused additional harm by questioning or not believing WWUD, profiling WWUD due to their criminalized identity, arresting WWUD for violating the terms of their probation (including using drugs when directed not to, and/or entering a red zone that the person had been forbidden to enter), or directly inflicting physical, emotional, or psychological violence upon WWUD. Such police interactions represented another form of disappearance experienced by WWUD; not only did many participants feel unable to be in public areas due to the potential risk of violence from people in community, they also wanted to avoid the systemic and targeted violence perpetrated by police towards WWUD.
The inconsistency of drug composition and potency also contributed to participants’exposures to drug toxicity. While many discussed using benzodiazepines with no issue, without the quality control provided by legal regulation benzodiazepines can heighten the risk of complex overdose, especially when combined with opioids (e.g., “benzodope”). This is made more concerning by the fact that naloxone, a medication that can temporarily reverse an opioid overdose, does not work on benzodiazepines. Several participants noted that they had experienced a near fatal overdose within the year prior to our interview. And I’ll be narcaned like eight times or so so, it scares the hell outta me and it happens to a lot of people out there. They just don’t react well to benzos. Like even the smallest traces. And that's what's killing a lot of people. Your brain forgets to breathe is literally what it is. (Participant 03)
As pointed out by this participant, benzodiazepines, like opioids, can affect the ability of people to breathe properly due to its depressant effects on the central nervous system, increasing the likelihood that an overdose involving benzodiazepines might be fatal. Without the ability to use naloxone as a means of benzodiazepine overdose reversal, overdose responses are generally more involved, with those experiencing a “benzodope” overdose often taking longer to return to baseline. In tandem, participants also described that people sometimes remain unconscious for hours following a “benzodope” overdose, shaping the risk of overdose-related complications.
Notably, participants expressed that WWUD will continue to experience preventable deaths and other forms of violence, including GBV, if the largely prohibition-based status quo remains unchallenged. Government inaction regarding prohibition was seen as a central part of the violence endured by WWUD, normalizing GBV and mass death and making many WWUD feel as though their lives were expendable. In order to curb the negative experiences associated with unknown or unpredictable benzodiazepine use, including overdose, participants repeatedly spoke to the importance of ending prohibition and regulating the unregulated drug market, which would allow WWUD to easily obtain safe, accessible drugs that are similar in composition to street-level drugs. They need to make [safe supply] more realistic. I would say look at like legalizing drugs and stuff. I know it's not gonna work out ideally quite the way you want it to but like, try putting it out there. Like and at a real fucking level. Not like, not like this little Mickey Mouse thing like, you’re like giving children's Tylenol to [adults]. Let people be adults and, make their own decisions because, when it comes down to it they’re gonna anyways and, they’re gonna find a way, so we need to make it safer. (Participant 03)
Narratives especially highlighted the need for different approaches in terms of regulatory models (including medical and nonmedical models) to ensure accessibility and a meaningful reduction in reliance on the unregulated drug supply. Moreover, as pointed to by the above participant, many underscored that any regulatory model implemented should be inclusive, allowing for WWUD “to make their own decisions” about their drug use (e.g., in terms of drug type, consumption methods, etc.) and use drugs for whatever reason they choose without being policed or pathologized, including the pleasurable, relaxing, and social aspects of drug use.
Community Care and Involvement in the Face of Structural and Everyday Violence
WWUD highlighted that community care and involvement were critical in establishing some protection from the violence associated with prohibition-based policies and the subsequent unpredictable drug supply. Participants pointed to the ways in which community networks and information sharing were integral in responding to potentially disruptive or harmful situations, including the prevalence of benzodiazepines, and helped prevent the various disappearances experienced by WWUD in this context. For example, WWUD recounted informing each other about the detection of misidentified (e.g., opioids containing benzodiazepines) or especially potent drugs, which allowed others to adequately prepare for potential risks or be more discerning in what they were purchasing. This was described by one participant who noted: Um, well I always try to test my drugs, or buy from the same person that I trust […] My friends will also tell me about the dope that's going around so I can be more careful […] Also doing it at home, that's pretty safe for me because there's always someone here. If I'm worried about using certain dope, if I haven't used it before, I will go tell my neighbour to come use with me or check on me. (Participant 26)
Consistent with the above narrative, participants spoke extensively about the ways in which they would look out for each other in order to mitigate the everyday violence and subsequent disappearances perpetuated by the unregulated drug supply. Particularly, WWUD repeatedly described using together in order to avoid the potential for a fatal overdose or being taken advantage of following the unpredictable or unknown use of benzodiazepines.
In line with this, several participants also discussed selling or providing unregulated drugs themselves, disrupting the artificial user/seller binary. Challenging common stereotypes of people who sell drugs, these participants often described engaging in practices of care to ensure drug quality and reduce the potential for prohibition related harms (e.g., unpredictable drug content/quality) for those in their community, particularly other WWUD. This included testing their drugs before selling, acting as a witness or using with others to reduce the potential for fatal overdose, distributing naloxone, and/or supplying people within their networks.
Community-run spaces were also discussed as being hugely important in building connections and contributing to a sense of safety among WWUD in the face of the unsafe conditions largely reproduced by the state, including mechanisms of state surveillance and criminalization. Many participants spoke to such spaces as providing an important refuge from the structural and everyday violence WWUD face. Well [a local community-run harm reduction site] has a lot of respect from the people on the streets, right? Because they could relate to us and we’re mostly all friends, right? […] So it's a place where I feel safe. (Participant 09)
Participants pointed to the ways that community-run harm reduction organizations are imperative in creating safer spaces for WWUD to manage the intersecting impacts of the ongoing unregulated drug toxicity crisis. Beyond mitigating the risk of a potentially fatal overdose, such spaces also ensure protection from the GBV associated with unpredictable or high potency benzodiazepine use in community. For WWUD, these spaces were also discussed as ensuring reliable community support and relative protection from police or related modes of state violence.
Discussion
In the context of the volatility fostered by a prohibitionist approach to drug policy and exacerbated by COVID-19 related border closures, participants highlighted that the contaminated drug supply, including the advent of benzodiazepines at unknown content or potency, was associated with long lasting memory loss or, in some instances, temporary loss of consciousness. This was described as shaping WWUDs’ vulnerability to GBV amidst systemic gender inequity and misoginy. Drawing on concepts of structural, symbolic, and everyday violence, our results highlight that the structural violence of prohibition and systemic criminalization, in tandem with related forms of social and structural violence endured by many WWUD (e.g., gendered subordination, settler colonialism, racism, poverty, social exclusion, etc.), have led to experiences of everyday violence stemming from the unpredictable drug supply. Without the quality control provided by legal regulation, the increasingly toxic supply makes it difficult to assess drug quality, placing WWUD in potentially dangerous or precarious situations.
Among WWUD, we found that gender, compounded by intersecting social locations (e.g., income level, race, housing status, etc.), played a considerable role in shaping experiences following the unintentional or unpredictable use of high-potency benzodiazepines. This is in line with past research that has highlighted that the unregulated drug toxicity crisis and related impacts are gendered (Ataiants et al., 2022; Boyd et al., 2018; Collins et al., 2019; Harris et al., 2021; Macleod et al., 2021; Martin & Walia, 2019; McNeil et al., 2014). In particular, WWUDs’ experiences are heavily shaped by social conditions and interconnected systems of structural, symbolic, and everyday violence that normalize gendered differences in drug- and prohibition-related outcomes. This is reflected in our results, which demonstrate how the volatile unregulated drug supply and experiences of targeted GBV are intimately connected.
The sedative and memory-loss effects of benzodiazepines, along with a lack of opportunities to discern drug composition, were shown to increase participants’ risk of GBV. This, combined with the social-structural vulnerability many WWUD endure due to their gender subordination and visibility, as well as the widespread normalization of GBV among WWUD, exacerbated the potential for violence in participants (Boyd et al., 2018; Collins et al., 2020a, 2020b; El-Bassel et al., 2020; Goldenberg, 2020; Harris et al., 2021; Harris et al., 2024; Knight, 2017; Knight et al., 2014; Krüsi et al., 2016; McNeil et al., 2014; Shirley-Beavan et al., 2020; Värmå Falk et al., 2020). The imperialist and racist roots of prohibition also created the conditions in which Indigenous or otherwise racialized participants remained disproportionately impacted by prohibition and systemic criminalization, heightening their vulnerability to benzodiazepine-related exploitation, including targeted GBV (Gordon, 2006; Lavalley et al., 2018; Martin & Walia, 2019). Our findings are consistent with recent community reports highlighting accounts from WWUD who described prolonged periods of memory loss or passing out completely upon using benzodiazepines—often without their prior knowledge—resulting in experiences of physical or financial harm (Crackdown, 2022; St Denis, 2021).
Alongside the violence reproduced by prohibitionist drug policies, our results also suggest that multiple modes of criminalization increased WWUDs’ risk of GBV and overdose. In line with previous research, this was especially apparent among participants supporting themselves through sex work, who spoke about the dual criminalization they endure as a result of their sex work involvement as well as drug use, and how this has made it exceedingly difficult for them to enact critical safety strategies in the context of the everyday violence perpetuated by the unpredictable drug supply (e.g., relying on others for safety/support, reporting incidents of violence, etc.) (Goldenberg, 2020; Goldenberg et al., 2022; Harris et al., 2024). Moreover, sex workers who use drugs noted that the influx of benzodiazepines, and the subsequent sedative and memory loss effects, increased difficulty in responding to occupational violence, negatively shaping sex workers’ health and safety.
In line with this, WWUD spoke to having little recourse following incidents of robbery, physical, or sexual violence, due both to their criminalized identities and, at times, limited recall. Contacting police following incidents of benzodiazepine-related GBV was described as not being an option because of concerns of discrimination, further criminalization, potential for arrest (e.g., due to probation or red zones), widespread mistrust of the police, and prior experiences of GBV at the hands of police. According to those interviewed, this dynamic not only allowed WWUD to be targeted with impunity, it notably contributed to the normalization of the everyday violence endured by WWUD, leading some to self-blame for the violence they had experienced. Critically, this finding builds upon past research which has demonstrated that heightened surveillance and policing do not improve WWUDs’ situation in the face of the ongoing unregulated drug toxicity crisis. Rather, such forms of scrutiny have been shown to make WWUD disappear from public spaces as an attempt to exist outside of the police's purview, distancing WWUD from community visibility or support and subsequently heightening the potential for, or exposure to, GBV and other outcomes stemming from prohibition, including overdose (El-Bassel et al., 2020; Birgin et al., 2022; Boyd et al., 2018; Goldenberg, 2020; Harris et al., 2024).
Our findings highlight that the GBV and above-mentioned police violence encountered by WWUD is part of a continuum in which structural and everyday violence are mutually generative (Scheper-Hughes & Bourgois, 2004). As already noted, we found that the structural violence of prohibition, in tandem with the structural violence reproduced by gendered subordination, settler colonialism, racism, poverty, social exclusion, and related forces, has created the conditions in which the everyday GBV faced by WWUD (particularly low-income, Indigenous or otherwise racialized, or criminalized WWUD) has been socially and culturally engrained into the status quo. The normalization of this kind of structural and everyday violence was found to create the conditions that allowed for the increasingly abhorrent forms of GBV experienced by WWUD to persist and be internalized as routinized or justified, even among some participants, with the influx of benzodiazepines in the unregulated drug supply.
Several participants we spoke to discussed using benzodiazepines with no issue, often purposefully seeking out benzodiazepines due to their myriad positive effects (e.g., relaxation, sleep support, managing anxiety, extending the half-life of fentanyl, etc.). Despite this, many also spoke to the fact that combining benzodiazepines and opioids can increase the likelihood of experiencing a complex overdose, often taking WWUD longer to return to baseline (Bonn, 2023; McNeil et al., 2022; Payer et al., 2020; Russell et al., 2023; Ti & Tobias, 2021; Walton et al., 2016). In line with the above discussion, the fear of being taken advantage of or harmed during experiences of prolonged memory loss or sedation meant that many participants opted to use benzodiazepines away from others, generally in their homes, despite the potential for complex overdose. Notably, roughly 75% of 2024's overdose deaths in BC occurred in private or other residences, with WWUDs’ rate of fatal overdose rising (BC Coroners Services, 2024). Many participants expressed a willingness to take on this risk in order to avoid violent or invasive incidents in community. Consistent with past work (Boyd et al., 2018; Fast, 2023; Macleod et al., 2021; Norton et al., 2022), such experiences illustrate the way in which GBV, or the possible threat of GBV, removes WWUD from public view and increases their exposure to more dangerous drug use environments, including using alone, which heightens vulnerability to fatal overdose.
Again, WWUD would not be placed in a position of being potentially exposed to GBV in community, or experience heightened overdose risk, if prohibition-based policies were not widely enforced. As already pointed to, prohibition, punitive drug laws, and systemic criminalization create the conditions that cause death and harm by incentivizing an ever more toxic supply (Cano et al., 2024; McNeil et al., 2022; Xavier et al., 2024). Participants highlighted that unknowingly using benzodiazepines, or unknowingly using high-potency benzodiazepines, profoundly shaped their vulnerability to GBV. While community support and strategies to reduce the widespread impacts of prohibition were identified as being beneficial to participants’ safety and well-being, this ultimately does not address the structural drivers of the unregulated drug toxicity crisis, leaving WWUD at continued risk of gender-based and drug war violence. The influx of benzodiazepines within the supply and the associated gendered harms outlined in this paper further underline the need for a regulated, predictable, and accessible drug supply.
Ultimately, our results offer another perspective to the urgent call to end prohibitionist approaches to drug policy, and to address the intersecting forms of structural violence that reproduce and normalize the everyday GBV experienced by WWUD. Across narratives, it became clear that while the drug toxicity crisis is often framed through the tragic loss of life, experiences of drug war violence, especially among WWUD, extend beyond fatalities. In particular, while overdose fatalities tend to be higher among men (BC Coroners Services, 2024), our results highlight how the unregulated and increasingly toxic drug supply is linked to increased experiences of GBV, disproportionately impacting WWUD. Given these findings, it is important to highlight the nuanced ways that social locations converge to shape experiences in the context of the ongoing unregulated drug toxicity crisis, accounting especially for the gendered impacts of prohibition, which can often be overlooked but have significant consequences for WWUD.
Conclusion
This paper has demonstrated how the volatile unregulated drug supply has also amplified experiences of GBV among WWUD. Using concepts of structural, symbolic, and everyday violence, our findings highlight the way in which pervasive structural and symbolic violence, including increased exposure to an unpredictable drug supply that is propelled by prohibition and the subsequent normalization of supply related harms, is linked to heightened experiences of everyday GBV among WWUD. In order to mitigate the gendered harms of the unrgulated toxic drug supply, our findings underscore calls to legalize and regulate the current drug supply, not only to end overdose fatalities, but also to reduce vulnerability to GBV among WWUD. This needs to happen alongside sustained efforts towards gender equity more broadly.