
Abstract
The fourth wave of the opioid toxicity crisis has resulted in a public health emergency in Canada (Public Health Agency of Canada, 2024) and is characterized by the combined use of psychostimulant drugs (e.g., methamphetamines) and/or benzodiazepines (e.g., alprazolam) with opioids, specifically potent opioids such as fentanyl and its analogues (Ciccarone, 2021; Toronto's Drug Checking Service, 2024; Volkow & Blanco, 2021). Due to the increased toxicity of the illicit drug market (Ciccarone, 2021), between 2020 and March 2024, there have been an estimated 32,461 opioid-related deaths in Canada (Public Health Agency of Canada, 2024), demonstrating the necessity of expanding services to reduce the serious harms associated with this crisis.
Safer Supply Programs
In the current context, traditional opioid agonist therapy (OAT) appears insufficient to address the substance use needs of many people who use drugs due to increased opioid tolerance and overdose risk (Karamouzian et al., 2023). In response to the opioid toxicity crisis and to address the unregulated drug market containing unknown contaminants (e.g., high-potency fentanyl-related substances, benzodiazepines, and nitazenes; Toronto's Drug Checking Service, 2024), safer supply programs (SSPs) have been implemented (Tyndall, 2020). Safer supply programs provide regulated prescription medications (e.g., diacetylmorphine, hydromorphone, dextroamphetamine) to people who use drugs (Government of Canada, 2024a; Ivsins et al., 2020). Operating as harm reduction services, SSPs tend to be low-threshold services that reduce accessibility barriers such as complex referral processes as well as high-tolerance in their approach (Klaire et al., 2022), which aims to retain individuals in treatment by removing strict policies (urine testing, etc.), to reach individuals who may not be able to adhere to or are not interested in other harm reduction services, such as OAT (Karamouzian et al., 2023). Opioid agonist treatment programs that do not operate using low-threshold and high-tolerance approaches may be too rigid in their rules, which can contribute to program dropouts or discharge (Power et al., 2024).
Among SSPs, there are differences in the services offered, the medications available, whether dispensing is supervised or not, and the types of consumption that are allowed on-site (i.e., inhalation, injection, intranasal use). Conceptualized as a form of safer supply, injectable OAT (iOAT) is a treatment program that aims to address the substance use health needs of those who have not responded to traditional OAT, by providing pharmaceutical grade opioids in a prepared liquid form (e.g., hydromorphone) to inject. Injections are generally supervised by staff trained in overdose response (Glegg et al., 2022).
Effectiveness of SSPs
Although the implementation of SSPs is recent, research examining their effectiveness is rapidly expanding, demonstrating overall reduced overdose events and mortalities among individuals receiving safer supply, in qualitative (e.g., Haines & O’Byrne, 2023; Ivsins et al., 2021), quantitative (e.g., Slaunwhite et al., 2024), and mixed methods studies (e.g., Klaire et al., 2022). Improvements in the mental and physical health of individuals receiving safer supply have also been reported (Haines & O’Byrne, 2023), along with increased financial stability as reported by program participants (Bardwell et al., 2023), and decreased engagement in criminal activities, also reported by program participants (Bonn et al., 2020; Giang et al., 2023). Individuals receiving safer supply have reported decreased engagement with the unregulated drug market and injection drug use (Bardwell et al., 2023; Gagnon et al., 2023). For example, some participants in a qualitative evaluation of four SSPs in Ontario discussed their decreased use of fentanyl and the transitions in their mode of administration from injection to taking oral safer supply medications (Gagnon et al., 2023). In addition, the cost-effectiveness of SSPs has been demonstrated (Gomes et al., 2022), where individuals receiving safer supply from a program in Ontario, Canada resulted in decreased healthcare costs, emergency department visits, and hospital admissions compared to individuals not receiving safer supply. Conversely, a recent study in British Columbia, Canada, where safer supply is available, found increased opioid-related poisoning hospitalizations, which the authors suggested might be due to diversion of safer supply prescriptions into the community (Nguyen et al., 2025). However, the observational and comparative design (i.e., outcomes from British Columbia were compared to “control” provinces, including Manitoba and Saskatchewan, where contextual factors such as the nature of the drug market may differ), prevents drawing conclusions regarding the cause of these observations (Nguyen et al., 2025). An additional study by Slaunwhite et al. (2024) identified reduced all-cause mortality and overdose-related mortality in participants who had received opioid safer supply one week prior and no statistically significant differences in acute care visits (i.e., ER visits and hospitalizations) when compared to those who did not access safer supply.
In New Brunswick, Canada, there is currently only one SSP that operates as an iOAT program (Government of Canada, 2024b). The iOAT program evaluated is located in Fredericton, a city with a population of approximately 60,000 individuals, surrounded by more rural communities (Statistics Canada, 2023). This iOAT program provides supervised injectable doses of liquid hydromorphone to clients three times daily, along with long-acting doses of oral OAT to prevent overnight withdrawal symptoms.
Gaps in the Literature
Safer supply programs in Ontario and British Columbia have been the primary focus of program evaluations that have occurred in Canada (Ledlie et al., 2024). Although this research is useful, findings from research conducted in one location may not translate to another geographical area (Morrison et al., 2017). The political context of a region influences program funding, availability, and operating practices (Morris et al., 2023). Variations in the nature of the drug supply must also be considered, as such differences can influence client needs. Although fentanyl has previously appeared predominantly in Western Canada as opposed to stimulants in Eastern Canada (Payer et al., 2020), the drug supply is constantly shifting. Recent reports examining the drug supply in New Brunswick have shown an increased presence of fentanyl (Government of Canada, 2024c), specifically fluorofentanyl, which is considered to be twice as potent as fentanyl (Toronto's Drug Checking Service, 2024) and highlight the necessity of regional evaluations. Furthermore, as SSPs are a newer service, barriers identified in program evaluations can be useful to adjust services to better reflect the needs of the population accessing them. Specifically, qualitative research is useful as it can contextualize quantitative research outcomes (Ivsins et al., 2023), provide the necessary perspectives of individuals using the services that are being evaluated (Michaud et al., 2024), and counter stigma and exclusion faced by people who use drugs (Selseng et al., 2021).
Purpose of the Current Study
The purpose of the current qualitative study was to assess a New Brunswick SSP offering iOAT, from the perspective of program users, to better understand program experiences, the program's impact, and potential treatment barriers. The Gelberg-Anderson Behavioral Model for Vulnerable Populations theoretical framework (Gelberg et al., 2000), a framework based off Anderson's Behavioral Model of Health Service Use (Andersen, 1995), guided the design of the study and interview guide. This framework emphasizes the multiple factors that impact the health of vulnerable populations as well as their access to health services, such as mental health symptoms, housing situation, victimization, and stigmatization (Gelberg et al., 2000). Specifically, the model considers predisposing factors such as substance use and demographic characteristics, enabling factors such as availability of care and barriers to accessing services, and need factors that encompass medical/psychological conditions necessitating treatment (Stein et al., 2007). The inclusion of stigma in the model is of particular interest given that stigma can result in structural barriers like institutional policies that reduce the accessibility of treatment or harm reduction options, and physical barriers such as a lack of transportation and limited treatment locations. In line with this theoretical framework, people who use drugs were engaged throughout the research, including involvement in the design of the interview guide to understand the experiences of program participants, program impacts, and barriers. The research questions for the current study were: (1) How does the iOAT program compare to previous programs used by participants?, (2) What are the impacts (positive and/or negative) of being in the program on participants’ lives (e.g., overall well-being, safety, and overdose frequency)?, and (3) What potential barriers (e.g., transportation challenges and program wait-times) impact participant's access to and continuation in the iOAT program?
Method
Participants
Semistructured interviews were completed with participants (
Materials
Participant demographics (e.g., age, gender identity, ethnicity) were collected in addition to current housing situation and substance use history. The semistructured interview guide was used to address the research questions. Participants were asked about their experience accessing the iOAT program, about the medications they receive, and about any interruptions to their safer supply and the subsequent impacts of such interruptions. Participants were queried about their experiences with the service providers (i.e., doctors, nurses, and social workers) and were then asked about the overall impacts of the program on their lives (e.g., substance use and overdoses). Lastly, participants discussed their met and unmet program needs.
Procedure
Ethical approval for the current study was granted by the authors’ institutional Research and Ethics Board. Semistructured interviews were completed by the first author in a private room with participants at the clinic. Participants were reminded that the evaluation was external, that their care at the SSP would not be impacted based on their participation, and that the summary of findings provided to the clinic would not include identifying information. Interviews lasted approximately 40 min (
Results
Characteristics of the Sample
Participant demographic information is presented in Table 1. Participants were on average 34 years old (
Descriptive Statistics.

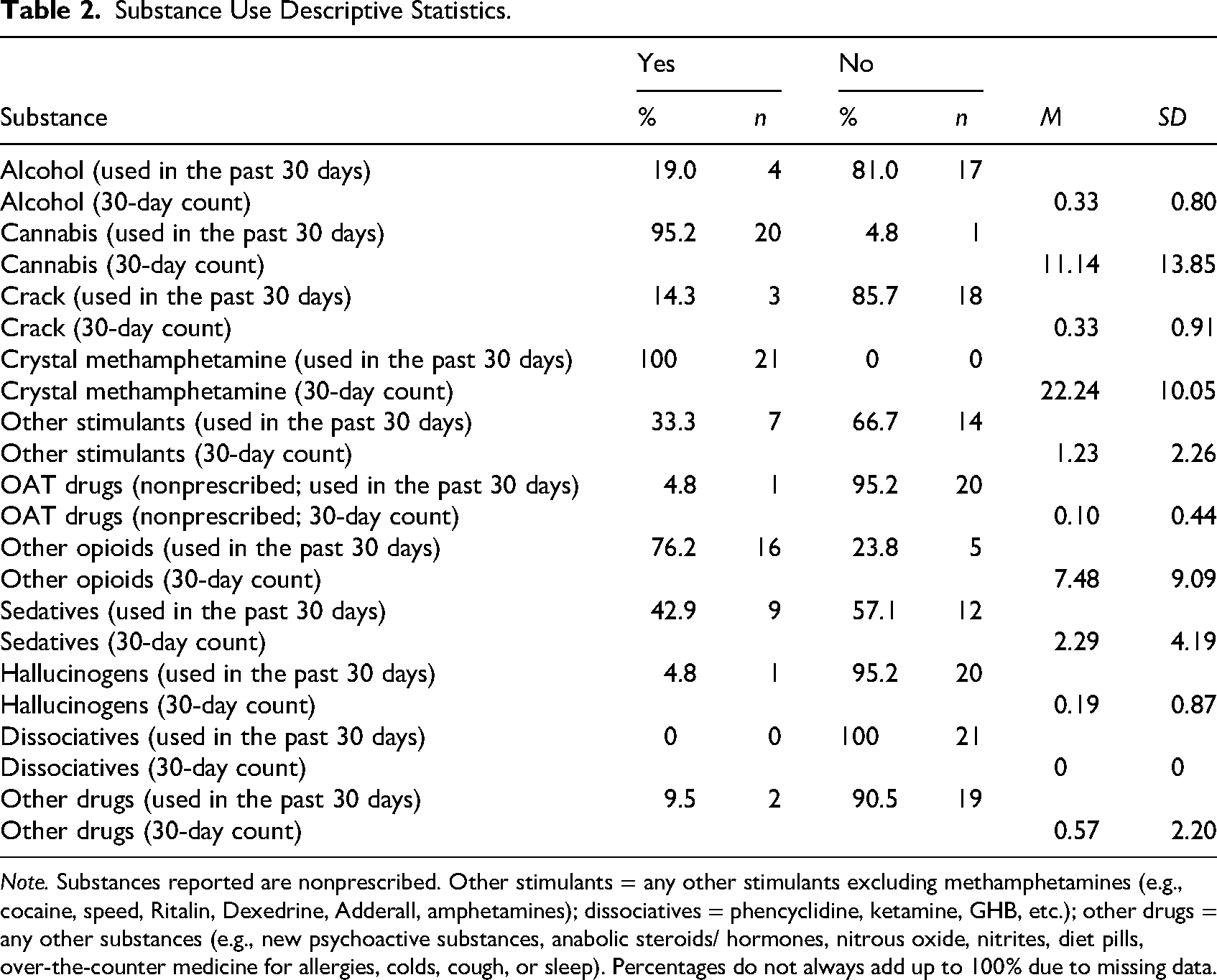
Substance Use Descriptive Statistics.
Qualitative Analysis
The following themes and subthemes emerged from the IPA (see Table 3). The interview centered around three research questions, pertaining to the participants’ experience in the iOAT program, the impact of the program on their lives and the potential barriers they experience.
Themes Identified Using IPA.

Experiences in the Program and Philosophy of Care
Low-Threshold Approach
The importance of the low-threshold characteristics of the program, which reduce barriers associated with accessing and remaining in treatment, was discussed by all participants. Direct interactions with the clinic staff because they were receiving other services at the clinic prior to enrolling in the program and/or being referred to the program by individuals already receiving services contributed to the low-threshold qualities (i.e., ease of program initiation) of the program. One participant explained “I was actually told by like a friend of mine about the program…like while we were using” (Participant 5). This individual heard of the program in a casual setting, walked into the clinic the same day, and had started on the program that week. Being able to walk-in to the clinic without the requirement of having booked an initial appointment was one of the low-threshold qualities of the program that participants appreciated. Another individual said, “I just came in, like I had come to River Stone before the program had started…so they knew me here from that, so I felt comfortable coming in” (Participant 1). This individual had participated in addiction education classes at the clinic, during which they developed relationships with the clinic staff. These relationships and prior knowledge of the clinic contributed to the ease of their program initiation.
Additionally, most participants compared their experiences in an OAT program to that of the iOAT program. Several participants had transitioned from OAT to iOAT, and although individual reasons differed, many participants reported that the OAT program was not meeting their needs (e.g., not sufficiently addressing withdrawal symptoms, and medication side effects). One participant explained their transition, saying “I got on to the Suboxone®, but I just, I couldn’t do it, it wasn’t enough, and then…I went right to the iOAT…I believe I actually used umm, outside, like that night, and then that next morning I was on the iOAT program” (Participant 3). This participant was experiencing withdrawal symptoms while receiving OAT and addressed their unmet needs by using opioids from the illicit market. Additionally, the iOAT program was described as being higher tolerance than OAT programs. For example, participants mentioned strict attendance and urine testing requirements in OAT that were absent from their iOAT experiences. Participants also discussed not being penalized for missing initial appointments. One individual said, “I had a few appointments like here and there to start the program, but we were doing fentanyl at the time and well I was supposed to be like here, [but] I was not at all” (Participant 17). This individual explained that they were welcomed by staff once they were ready to start the program, regardless of their missed appointments. The program was there for them once they were ready.
Safety
Participants described that the harm reduction approach of the program was central to instilling a renewed sense of safety in the context of an unregulated and dangerous opioid supply. Participants described that they are provided with a regulated supply of opioids, access to clean equipment, and testing and treatment for HIV and HCV. One individual who discussed the impact of the program's harm reduction approach said: I don’t have to worry about what I’m getting, I know I’m getting a Dilaudid® [hydromorphone]…and I know that if I, if I overdose, they’re great here, whereas before, I didn’t, if you’re getting beads, like hydromorphs…they could put anything in that, they could open the capsule and put anything, anything, and, you know they could put drift [deflazacort] in, and that's not safe to inject. (Participant 1)
This individual appreciated the program's harm reduction approach in that they were accessing a supply of opioid medications that were free from unknown contaminants, and that in the case of an overdose, they had confidence that the clinic staff would respond appropriately. The harm reduction approach instilled a sense of safety for this individual that was absent prior to their program initiation. Participants also described the importance of the program's harm reduction approach to their program initiation. A participant explained: My life was spiraling out of control…I overdosed really bad on what I thought was fentanyl but was isotonitazene like pure pure isotonitazene…so that was actually, that was probably like the main, main reason why I went and got on the program, because it was a safer place to get my fix, and I didn’t have to worry about dying like imminently. (Participant 21)
This individual discussed that the main driver to their initiation in the program was their life-threatening experience, and their awareness that an overdose from using unpredictable substances from the illicit drug market could be fatal. They were offered a renewed sense of safety in knowing that the substances they were using were what they were labeled to be.
Restoring Sense of Worth
Participants discussed their experiences of stigma within the healthcare and criminal justice systems and contrasted these experiences with those had in the iOAT program. Their restored sense of worth transpired from the content of their discussions. For example, when discussing their experiences at the clinic, one individual said, “they don't judge you and they treat you like a human” (Participant 8). This individual was discussing their experiences interacting with the clinic staff, and that being treated with respect increased their autonomy and sense of worth. They were able to access care and support in their treatment, which increased their own sense of worth and value as a human, regardless of their substance use.
Unmet Healthcare Needs
Participants discussed their past healthcare and substance use treatment experiences and compared both to the services and care they receive in the iOAT program. Many participants talked about their negative and stigmatizing hospital experiences, attributed to their substance use and participation in nonabstinence-based programs. For example, one participant explained “you go to hospital and then you’re just treated like a piece of shit cause you're an addict right” (Participant 8). Another individual said, “I don’t like going to the hospital for anything, especially if you have the flag on you that you’re in a program like this then they uh I find that they’re just super judgemental right” (Participant 21). These individuals indicated that the stigma they encountered at the hospital was due to either their substance use or nonabstinence-based program involvement, respectively. Another participant explained that their hospital experiences were “bad, horrible, not pleasant at all, very uncomfortable” and stated that they are “100% different from the experience that [they’ve] had here [at the iOAT clinic]” (Participant 3). This individual expressed that they perceived judgment due to their substance use in a different healthcare setting. Some healthcare providers maintain the view that abstinence-only approaches to substance use are more desirable than medications for the treatment of opioid use disorder, such as OAT medications and iOAT programs. Providers with this view may assert that programs that provide access to opioid medications are giving individuals access to “free drugs” and may not be open to seeing the harm reduction aspects of the program. Experienced stigma during hospitalizations led to unmet healthcare needs in participants (i.e., individuals leaving the hospital without receiving care and/or not seeking future medical care due to a fear of experiencing additional stigma).
Discontinuity in services
Participants who reported interruptions to their safer supply (from being arrested or hospitalized) explained that interruptions resulted in experiencing harmful withdrawal symptoms. Participants attributed inconsistent dosing practices/allowances in healthcare and correctional facilities to stigma. For example, participants explained that they received or were denied doses of safer supply while hospitalized and attributed these decisions to the healthcare providers’ views of the iOAT program. One participant discussed an interruption to their safer supply from being arrested, saying “I went four to five days without anything…that was brutal, brutal…it was inhumane…I was puking, had the poops, and I was pill sick…they didn’t know what I was talking about, the program, they didn’t even know about the program” (Participant 8). This individual expressed that their lack of access to safer supply medications while incarcerated contributed to their suffering and that a lack of knowledge about iOAT in these settings contributed to what they experienced as inhumane treatment.
Participants’ Outcomes in iOAT
Participants mentioned the impacts that the iOAT program has had on their lives through the themes of stability and social determinants of health.
Stability
Participants identified improvements in mental health and financial stability and decreased engagement in criminal activities. This was the result from a shift from centering their daily lives around opioid use to other priority areas of their lives. For example, one participant explained that they have been “able to focus more on…getting other parts of [their] life in order” (Participant 3). Specifically, this individual explained that since being on the iOAT program and “not having to worry each and every day how am I going to get my next fix,” their stress levels decreased, which allowed them to allocate their energy to securing housing, a previously identified priority for them. Another individual explained their satisfaction with the program, saying “it's actually doing a lot for me, a lot more than I thought it would. I thought I was just going to come in here and get high three times a day but…it's more…emotional and like uh mental” (Participant 11). This participant was surprised that in addition to access to opioid medications, the iOAT program contributed to improvements in their mental well-being, such as increased confidence and motivation to pursue their goals. An additional participant stated, “I don’t have to go sick, if I couldn’t find anything, or I don’t have to go rob or steal something…it keeps me out of jail, or I could be dead…it saved my life, because I was in a dark, dark place” (Participant 8). After accessing the iOAT program, and de-centering their life around substance use, they noticed that their mental well-being had improved, specifically referencing decreased symptoms of depression.
Similarly, related to a reduced reliance on the illicit drug market, participants reported improvements in their financial stability, and explained that they can allocate more of their income to other needs, such as food and housing. One individual explained that they “have a lot more time and…a lot more money…and [are] starting to have a little bit more normal of a life” (Participant 7). This participant indicated that because of their reduced reliance on purchasing substances from the illicit drug market, they have more money to spend on clothing, food, and housing.
Noncriminal Lifestyle of Incarceration
Similarly, participants reported decreased engagement in criminal activities. Participants explained that their prior engagement in criminal activities was to access substances from the illicit market, but that with a regulated supply of opioids from the iOAT program, these behaviors have decreased. Specifically, participants discussed decreases in their substance use outside of the program, due to not having to rely on the illicit drug market to counter withdrawal symptoms. One participant explained “other than smoking a little bit of meth, I don’t do anything outside the program. So, that changed quite a bit…and I was doing a lot of drugs outside the program right” (Participant 16). This participant explained that before the program, they participated in illegal activities with the goal of obtaining substances from the illicit drug market. Following iOAT program initiation, their engagement in illegal activities and with the illicit drug market reduced, and their focus shifted to finding employment, an aspect of their life that clinic staff was supporting them with.
Another participant explained: I’m not getting in trouble for shoplifting or anything like that anymore, like I just come down here and get my meds instead of freaking breaking the law, so that's good, that's a big bonus, cause if I wasn’t here, I’d be out shoplifting or I’d be out stealing something to get what I need to get. (Participant 18)
This individual described that wanting to separate themselves from the criminal justice system and that having more funds to spend on food were their main reasons for program initiation.
Social Determinants of Health
In line with the Gelberg-Anderson Behavioral Model for Vulnerable Populations theoretical framework, social determinants of health refer to the multiple environments and conditions that contribute to health inequities among populations. Within the iOAT program, participants discussed the many ways in which the clinic was helping to address social determinants of health, such as housing, food instability, employment, health coverage, and transportation, among other factors. When discussing how the clinic was helping to address social determinants of health, one individual explained “anybody who looks at this program and doesn’t see the positive side from it doesn’t fully understand” (Participant 3). This was in reference to the negative public perceptions of the program, and how if they were able to explain the impacts that the program is having for them and others, they would be able to see the importance of the program. They discussed the decreased criminal activity in the area and that more people in the iOAT program have access to stable housing. They indicated that the program does more than solely provide access to opioids, but removes people from the cycle of opioid use, and then provides support in the areas that directly contribute to health, like housing and access to food. For example, one participant explained the help the clinic was providing them in finding housing: We’re going to meet and talk about getting a place [housing]…because like when you’re homeless you’re just in survival mode…you don’t have time to go look for a place. You don’t have time, or the resources, and you don’t…you just get into a staying alive mode and especially the colder the weather gets. They said, okay we’ll do it, we will make a day where you come in once a week, and we will look through all the ads and I won’t let you leave until you’ve written a few down and called a few. (Participant 1)
This participant explained that when they requested help for finding housing, the clinic staff was attentive to their needs and provided accountability and support. Another participant discussed how the clinic was helping them with employment and said, “man they gave me a job here…like they offer me to do like cleaning” (Participant 4). This same individual explained “well, when I came to this program, I didn’t have welfare or assistance or anything because I didn’t have any ID or anything, so they helped me” (Participant 4). The clinic actively supporting participants in addressing their social determinants of health was impactful for this participant, and many others who discussed critical needs that the clinic was helping them to address.
Structural Barriers
Participants discussed the barriers they experienced in accessing and remaining in the iOAT program. Structural barriers refer to the conditions (e.g., policies and lack of transportation) that result in inequities within a system, such as the healthcare system, or programs such as the iOAT program.
Physical Barriers
Most participants discussed barriers to accessing their safer supply, mentioning challenges with transportation and daily attendance. Participants explained that these challenges impact their ability to find employment and to travel outside of the city. For example, one individual explained “it's just crazy to come down here three times a day, every day. It's like your whole life is just this program…I’d like to get back, go back to work and actually be able to do something with my life” (Participant 18). This participant was considering alternative programs to alleviate the time they spend at the clinic daily, and to allow them time to return to work. Another participant said, “the bad side to it is like I have to be here three times a day so I can’t go out to [location] for a day and spend the day with my kids cause I have to be here” (Participant 10). This individual expressed that the daily attendance requirements were keeping them from other important aspects of their life, such as family. When discussing challenges with transportation, one individual explained “I guess your only hard thing would be if you didn’t have transportation…Sundays, Sundays buses don’t run so…Sundays you have to, you got to get here the best way you know how. Depending [on] where you are in the city you know, it can be difficult sometimes” (Participant 3). This participant explained that on certain days, it is challenging to get to and from the clinic. They described biking and walking long distances to get to the clinic and receive care.
Institutional Barriers
Participants also discussed challenges associated with program policies such as the waiting period to start the program (i.e., period between the program intake appointment and the program initiation, approximately one week), the low starting dose in the program, and unmet mental health needs. Participants reported that program policies resulted in them experiencing withdrawal symptoms. For example, one individual explained their experience with the waiting period, saying “it took…about 5 days…it was a long five days…I was sick the whole time” (Participant 1). This participant explained that during the waiting period from their initial appointment to their program initiation, they experienced challenging withdrawal symptoms. When discussing the program's low starting dose, another individual explained that “it's a little frustrating because you’re used to doing so much and then…you’ve got this small amount that you’re doing, and you have to work up toward it…so it's kind of frustrating in the way that you’re going through withdrawals” (Participant 5). Although this individual indicated that they understood the medical precautions of starting at a low dose and gradually increasing, they described frustration because their tolerance was high from substances used outside of the program, and therefore experienced withdrawal symptoms. A related aspect was a minority of participants reporting that because they were using high-potency opioids (e.g., fentanyl), the liquid hydromorphone was not sufficient to counter their withdrawal symptoms. One individual explained “I just think it's not enough. Well, I do fentanyl on the street right? So uhm Dilaudid® [hydromorphone] isn’t really going to cut it, fentanyl is a lot stronger” (Participant 18). If medications do not counter withdrawal symptoms, this results in some participants either reporting supplementing with opioids from street supply or experiencing highly unpleasant withdrawal symptoms.
Unmet mental health needs were also reported by a few participants, as the program does not have adequate resources to address complex mental health needs. For example, one individual explained “they [program] want to help, but I think also I need to see a psychiatrist” (Participant 21). This participant explained that the lack of improvements in their mental health was not because the clinic did not see the need for support, but because their complex mental health needs could not be adequately addressed with the resources available at the clinic. This participant explained the stigma they encountered seeking mental health care at the hospital:
The psychiatrist on call, after listening to me cry to [them] and telling [them] that I didn’t see a reason to live anymore [they] told me to go to the homeless shelter a get a bed and go get a hot meal at the soup kitchen and then quit my programs at the [clinic]. So, if the first two things didn’t make to wanna kill yourself the last thing, the withdrawals from the last thing, sure as hell will. (Participant 21)
For this individual, their mental health needs were not being met within the clinic or within a hospital setting, resulting in a mental health crisis and a lack of options for receiving support.
Discussion
The current study was a qualitative evaluation of New Brunswick's first SSP, an iOAT program, from the perspective of program users. The purpose was to understand participant's experiences, the overall impacts of the program, and identify if any barriers to program access and treatment existed. Participants reported previous engagement with many substance use treatment programs, and prior to accessing this iOAT program, high rates of concurrent substance use (e.g., opioids and stimulants), unstable housing, and food insecurities, suggesting that the program is being accessed by individuals with complex needs.
Injectable Opioid Agonist Treatment Program Experiences
Participants described the importance of the iOAT program's low-threshold and harm reduction approach to providing regulated opioid medications, in an environment that supports engagement and retention in treatment. Many participants (71.4%) had received OAT but reported that the programs were inadequate to address their needs, highlighting the usefulness of iOAT programs to capture individuals who do benefit from OAT (Friedmann et al., 2024; Karamouzian et al., 2023). Safer supply program service providers have echoed the importance of operating low-threshold and nonmedicalized SSPs but noted that these aspects are difficult to achieve given the current medicalized approach to treating substance use disorders (Karamouzian et al., 2023). From the perspectives of people who use drugs, SSPs should operate to increase service accessibility and to provide safe environments (Pauly et al., 2022), aspects that have been reported as being important in previous SSP program evaluations (Henderson et al., 2024; Kolla et al., 2024).
In the current study, participants also reflected on the importance of the nonstigmatizing care that they receive in the iOAT program and often contrasted these experiences to previous negative and stigmatizing healthcare experiences. Participants explained that the nonjudgmental and respectful care from the iOAT staff was central to restoring their sense of worth and they contrasted this with their experiences in the community, such as within hospital settings, where they described negative experiences. These experiences often resulted in unmet healthcare needs among participants, which has been reported to be a consequence of healthcare stigma encountered by people who use drugs (Judd et al., 2023; Paquette et al., 2018). Brener et al. (2024) conducted a study in Australia to examine women who inject drugs’ experiences of stigma and its subsequent impacts on healthcare accessibility. Among the women, 75% reported having experienced stigma from healthcare workers, contributing to 77% of participants delaying access to healthcare services, and 81% avoiding disclosing drug use to healthcare providers. Nonstigmatizing care is a critical component of operating successful low-barrier SSPs (Bardwell et al., 2024). Safer supply programs should consider providing access to primary care, due to high levels of unmet healthcare needs in people who use drugs.
Participants also described interruptions to their safer supply (from being arrested or hospitalized) and explained that interruptions resulted in them experiencing harmful withdrawal symptoms, and in some cases, unmet healthcare needs (e.g., in hospital settings). Participants attributed interruptions to inconsistent dosing practices, a lack of appropriate guidelines on hospital/correctional practices for people who use drugs, and stigma encountered in both settings. Safer supply programs currently operate under medicalized approaches, where prescribers can be viewed as “gatekeepers,” an approach that may be supporting the criminalization of people who use substances, subsequently increasing stigma toward this population (Macevicius et al., 2024). Within criminal justice settings and healthcare settings, there are discontinuities within individual's access to services that are available in the community. Safer supply program service providers have previously reported concerns in the lack of continuity of care in these settings (Karamouzian et al., 2023). Interruptions to safer supply can reduce tolerance levels and increase unintentional overdoses (Karamouzian et al., 2023), which is especially concerning as one week following release from jail/prison settings, overdoses are the leading cause of death (Borschmann et al., 2024).
Injectable Opioid Agonist Treatment Program Impacts and Barriers
Participants were overall satisfied with the program, reporting increased stability in many areas of their lives and improvements in social determinants of health. Similarly, improvements in financial stability, decreased engagement in criminal activities, and a reduced reliance on the illicit drug market were also reported in previous SSP evaluations (Henderson et al., 2024; Kolla et al., 2024). However, some discussed the inadequacies of the medications available (i.e., hydromorphone) to meet their tolerance needs, specifically in cases of high-potency opioid use (e.g., fentanyl). Inadequacies in the medications available could be linked to the high rates of past 30-day opioid use reported in the current study, where individuals may have accessed opioids from the illicit market to avoid withdrawal symptoms. Challenges related to the strength of available medications have been reported by participants in other SSP evaluations in Ontario (Haines & O’Byrne, 2023; Henderson et al., 2024) and British Columbia (Kolla et al., 2024) and may be attributed to stigma toward people who use drugs as well as SSPs. Structural stigma is inclusive of societal norms and institutional policies that impact resources and the welfare of a group of individuals (Hatzenbuehler, 2016). Participants reported that iOAT policies (access to less potent forms of opioids, having to receive witnessed dosing several times a day at the clinic) acted as barriers to access and optimal treatment outcomes. Safer supply service providers have previously reported that these policies result from community and political pressure as well as provincial regulations on prescribing specific safer supply medications (Nafeh et al., 2025). These authors recommend evidence-based, safer supply practice guidelines to ensure guidance on the types of medications, dosage, and practices that SSPs should follow to ensure that individuals with the most complex needs receive appropriate care. To better address the needs of those accessing services, SSPs should offer a variety of medications, ranging in potency and formulation, to reflect the substances that are available in the illicit market (Kolla et al., 2024; Xavier et al., 2024).
Many participants reported improvements in their mental health, but there were also reports of unmet mental health needs. Including psychosocial care as part of SSP operations, as suggested by Krausz et al. (2024), could be beneficial, especially given not only the high rates of mental health comorbidities in those with substance use disorders (Bakos-Block et al., 2020) but also the potentially stigmatizing experiences that people who use drugs may experience when accessing services in the broader community.
Participants also explained that certain barriers to accessing safer supply were present, including transportation challenges and constraints related to daily attendance requirements. The barriers reported in the current study have been expressed by participants in SSP (Henderson et al., 2024) and more specifically, iOAT (Friedmann et al., 2024) program evaluations. Barriers such as these highlight the importance of considering individual challenges that might be associated with program adherence, and to tailor programs to best meet the needs of clients (Oviedo-Joekes et al., 2023). However, iOAT service providers have also reported on the physical (e.g., space, transportation) and institutional barriers (e.g., prescribing practices) that emerged in the current study, noting that they in part resulted from a lack of consistent political leadership, fluctuating support from policy makers for SSPs and strict regulatory environments (Karamouzian et al., 2023; Nafeh et al., 2025).
Recommendations
Based on the results from the current study, and the consensus in the literature, future SSP implementation should ensure that programs operate as low-threshold harm reduction services, as this emerged as central to the experiences of participants in this iOAT program. In addition, although it may not currently be feasible given the medicalized nature of SSPs (Macevicius et al., 2024), nonmedicalized approaches to operating programs could be helpful to reduce stigma toward people who use drugs and to increase service accessibility. Nonmedicalized models, such as compassion clubs, are SSPs that are not based on physician prescriptions, but allow individuals to purchase substances for their consumption that have been tested for unknown contaminants and labeled appropriately (Kalicum et al., 2024). This is especially relevant given that only a small proportion of individuals at high risk for overdose are accessing safer supply (Palis et al., 2024). Increasing the types of safer supply models that are available, including nonmedicalized SSPs, could also be helpful to reach individuals who are at the highest risk for overdose but are not accessing services due to factors associated with medicalized models (e.g., stigma, criminalization, racism, and colonization; Macevicius et al., 2024). Safer supply programs should provide wrap around services (primary care, social supports) to counter accessibility issues and healthcare stigma. Ensuring that sufficiently potent opioids are prescribed (e.g., Fentanyl patches), having an accessible location and satellite clinics, and more flexible policies (allowing take home doses or home deliveries, etc.) could address treatment barriers. However, several harm reduction programs report challenges finding an adequate location given the “not in my backyard” phenomenon, where community members and stakeholders oppose the implementation of services for people who use drugs due to fear, stigma, and financial concerns (Côté-Lussier & Rodrigues, 2024). Interventions that engage and increase contact between people who use drugs, community members and stakeholders can be useful to curb the impacts of the “not in my backyard” phenomenon, to reduce stigma toward people who use drugs, and to educate community members and stakeholders on the benefits of harm reduction services (National Academies of Sciences, Engineering and Medicine, 2016).
Strengths and Limitations
The current study evaluated an iOAT program from the perspectives of individuals accessing the program. Hearing from the voices of individuals who are affected by substance use is critical, especially considering the underrepresentation of people who use drugs in research and the stigma encountered by people who use drugs (Brener et al., 2024). In addition to the study being evaluated from the perspectives of individuals accessing the program, those with living/lived experience were also engaged throughout the study design (e.g., informing research questions and study materials) and research dissemination processes.
However, participants in the current study had recently engaged with the iOAT program and their experiences may fluctuate over time. More long-term evaluations are needed to assess the trajectories of individuals in iOAT programs and the sustainability of these programs. Furthermore, several forms of SSPs have been implemented and the results of this study may not reflect the experiences of individuals accessing other SSPs models or services.
Conclusion
The current study adds to the literature in support of SSPs reducing the harms associated with the opioid toxicity crisis. This research comes at a critical time when the sustainability of SSPs in Canada has come into question due to lack of stable funding (Kolla et al., 2024). Recent controversies surrounding the potential diversion of safer supply medications into communities has negatively impacted people who use drugs and their access to healthcare services, such as SSPs (Michaud et al., 2024). It is estimated that less than 10% of individuals with opioid use disorder in British Columbia have accessed SSPs (Kolla et al., 2024). In this context, rather than expanding SSPs accessibility in Canada given the growing body of literature that supports their positive impact, federal SSP funding (Major, 2025) has been halted at the same time that involuntary drug treatment is increasingly discussed despite limited evidence in its favor and concerns that it may increase opioid overdoses when people who use drugs complete the program (Canadian Centre on Substance Use and Addiction, 2025; Fischer et al., 2025). In light of the current findings, which demonstrate the impact of this program on its clients, the need for diverse models of care that can meet the substance use health needs of all individuals is necessary.