
Abstract
Keywords
Performance anxiety (PA) is a ubiquitous experience that often strikes when least desirable, such as in anticipation of, or during, a musical performance, a competition, or important presentation. The experience is typically unexpected and under-managed, highlighted by a strong fear of negative evaluation, reduced self-efficacy, and a strong sense to avoid, mask or flee the situation (Brugués, 2011). Formally situated in the
PA has been shown to particularly affect individuals in situations where performance is a fundamental component of their role, such as musicians, athletes, public speakers, and health professionals. Within these professions, individuals can often perform well in preparation for a performance but are impacted during the performance itself, such as when a musician recites a concerto beautifully in the practice room but freezes on stage. The introduction of an evaluative space (i.e., audience members or an outcome-based performance) often results in PA, where anxiety increases beyond a facilitative level. While some level of anxiety (or more appropriately arousal/activation) is understood to aid performance (Csikszentmihalyi, 1990), unmanaged PA can be detrimental not only to the performer and performance itself but also to the performance experience (Brugués, 2011). Importantly, the musician’s evaluation of potential threat is key to the level of anxiety they may experience. This is highlighted by both Osborne and McPherson (2019) and Murphy et al. (2024), where the appraisal of not only the performance environment, but also their internal experience has been demonstrated to impact the level of state anxiety experienced.
Regardless, the negative impact of pe has been demonstrated to contribute to negative perceptions and attitudes towards performance, such as an underestimation of ability (Abbott & Rapee, 2004), in addition to overall decreased coping perceptions, as well as one’s overall enjoyment in performing (Kenny, 2011). Current PA research is focused across a range of research areas (i.e., academic tests, music, and sport), with limited interdisciplinary synthesis, impacting how best to conceptualise and treat PA. Emerging research has demonstrated the applicability of sport psychology performance principals to musicians, with Osborne et al. (2014) demonstrating performance skills training is effective in building musicians’ mental skills and managing symptoms of MPA.
Research emphasising the distinguishing characteristics of different domains of PA is perhaps indicative of the desire to explore PA in an ecologically valid setting. Some researchers focusing on assessing and treating PA for musicians have suggested that musicians experience a particular type of PA that is potentially unique to their context (Brodsky, 1996; Kenny, 2005; Salmon, 1992). This is supported by the high prevalence rates of PA in musicians, as high as 60% in some studies (Fernholz et al., 2019), as well as the hypothesised unique technical nature of musical performance (Kenny, 2011). The anecdotally high dropout rate of musicians from the industry due to PA is not surprising given such high prevalence rates (Fernholz et al., 2019), and the accounts by individuals of the stress and pressure that performance can have on their overall health (Kenny, 2011). As such, the development of effective prevention and intervention strategies to assist this prevalent problem is warranted. Identifying efficacious and timely interventions is essential in addressing both the high prevalence of PA and dropout rates for musicians.
Previous systematic reviews
The most recent systematic review (Fernholz et al., 2019) assessed literature on the prevalence, risk-factors, and treatment effects for PA in musicians among professional musicians. Fernholz et al. (2019) built upon previous reviews (Brugués, 2011; Kenny, 2005) which noted the need to explore a wider range of studies to account for methodological problems. Tentative conclusions supporting cognitive-behavioural therapy (CBT) or cognitive-based techniques, and pharmacotherapy (i.e., beta-blockers) as the most effective interventions were made; however, meta-analytic techniques have yet to be employed comparing treatments or to assess aggregated effect sizes.
Kenny (2005) highlighted the impact of a lack of thorough definition, potentially effecting model development and treatment interventions based on model-based rigour. Kenny (2005) noted that the integration of PA as a subtype of SAD was potentially too restrictive, favouring conceptualising PA for musicians as a specific contextual form of anxiety, but also noted further exploration of the precipitating and maintaining factors associated with PA was needed to inform treatment. Current conceptualisations based on
Brugués (2011) concluded that cognitive-behavioural interventions appeared to result in the greatest reduction in symptom measure scores, while noting the need for preventative strategies to be disseminated. These included (1) choosing/performing a repertoire that the musician can perform well, (2) providing appropriate support for musicians and placing realistic expectations on musicians from a young age, (3) an emphasis on repeated exposure to performance situations in line with ability, and (4) early engagement with pedagogical processes around self-management anxiety strategies. These strategies, combined with awareness of PA symptoms, should result in the development of greater automaticity and cognitive confidence for musicians to perform in front of others (Brugués, 2011). Audition training, stress inoculation training, cue-controlled relaxation, and workshops all helped relieve a degree of stress for musicians. Brugués (2011) highlighted the lack of randomised studies as impeding a substantiative conclusion on the most efficacious treatment for PA in musicians. Of those categorised as being sound methodologically, a substantial number of papers appeared to explore ‘other’ interventions, indicating a lack of treatment protocols grounded in sound theoretical underpinnings (although this is improving with new research) and subsequent treatment targets. Treatments identified, however, were effective to a degree. Like Kenny (2005), this perhaps demonstrates the undiscovered ‘active ingredient’ in the treatment process for PA in musicians.
Interestingly, across three systematic reviews, authors identified three key challenges in concretely identifying effective treatments: (1) inconsistent assessment or diagnostic agreement, which is perhaps rooted in the lack of consensus on a definition for PA; (2) lack of methodological rigour, namely in randomisation, inclusion of control groups, and follow-up; and (3) assessment of subgroups of PA, that is, low versus high levels of PA, instrument subcategories, and stage of career. Importantly, previously published systematic reviews have provided a strong platform for further research to be conducted, and all emphasise the importance of methodological rigour in future research.
Previous meta-analysis
To the authors’ knowledge, only one meta-analysis has been published to examine the efficacy of treatments for PA in musicians. Recently, Faur et al. (2022) published a meta-analysis on cognitive-behavioural interventions for PA in musicians. This study explored an array of cognitive-behavioural interventions, including traditional CBT, interventions using specific cognitive or behavioural components, and Acceptance and Commitment Therapy (ACT) incorporating both randomised controlled and uncontrolled studies. The authors found CBT to have moderate to large effect sizes for most studies, with no statistically significant impact of treatment characteristics on outcomes. Results must be interpreted with caution as Faur et al. (2022) acknowledged that studies with no control groups rendered higher effect sizes than those with control groups. Interestingly, only two out of the 14 studies were individual treatments, and preliminary conclusions demonstrated no greater efficacy when compared with group interventions.
Aims and objectives
Over the last decade, there has been a strong increase in the number of studies exploring interventions for PA in musicians, such as ACT. Increased research focus on these new interventions has led to calls for their evaluation in the context of PA in musicians (Öst, 2014; Taylor et al., 2020). The consistent critique from previous reviews (Kenny, 2005) highlighted the need for methodological rigour and defined assessment protocols to assist in the development of consistent and replicable research. Therefore, the primary aim of this study is to provide an updated systematic review of available treatments for PA across the lifespan, with a focus on recognising the available assessment tools and quality assessment of the included studies, including a risk of bias analysis.
Recognising the breadth of studies available and the emphasis on quality and research integrity of past systematic reviews, the secondary aim of this article is to provide an updated meta-analysis of randomised controlled trials (RCTs) of interventions targeting PA in musicians. It is hypothesised that CBT will be the most efficacious treatment for PA in musicians in line with Fernholz et al. (2019), the findings of Faur et al. (2022), and guidelines for the treatment of SAD (Andrews et al., 2018). The authors also aim to assess the impact of the type of intervention (group vs. individual), and the population being treated (professional vs. college, vs. high school vs. mixed) on treatment outcomes.
Method
Protocol and registration
This article was structured in line with the Cochrane review guidelines (Higgins et al., 2022), following the PRISMA protocol (Hutton et al., 2015). This study was registered with the National Institute for Health Research (PROSPERO) on the 15 April 2022 [CRD42022316739], available from https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022316739.
Primary outcomes
We were interested in specifically assessing treatment effectiveness by exploring a reduction in PA symptomology as measured through symptom scores, self-reports, clinical interviews, or follow-up assessments. While acknowledging the number of other outcomes measured across studies, the focus of this review will be primarily on PA outcomes.
Search strategy
A systematic search of the databases PsycINFO, Scopus, MedLine, Cochrane, and IIPA was conducted. Keywords related to anxiety, PA, music, musicians, treatment, intervention, and management were used, resulting in a search line of (music* OR musician*) AND (‘performance anxiety’ OR ‘music performance anxiety’ OR ‘stage fright’) AND (intervention* OR treatment* OR therapy*). The search strategy is available on request. In addition to these searches,
Inclusion criteria
The inclusion criteria for this study were as follows:
a. Intervention was used to assess a change in PA scores;
b. Populations were musicians (any age);
c. Studies were published journal articles;
d. Studies were RCTs, experimental studies (uncontrolled trials), pilot studies, or case studies;
e. Studies were written or translated in English.
Data extraction
Data were extracted by the two authors using COVIDENCE (2022). After the search was completed and duplicates removed, each author individually assessed the title and abstract of the remaining papers. Of the studies included, Author 1 completed a full-text analysis in line with the inclusion criteria. Any disagreement was resolved by internal discussion; consultation of a third reviewer was not needed.
Appraisal of quality
Eligible articles were assessed to extract necessary data, including study design, participant characteristics, outcome variables, intervention type, treatment characteristics, and conclusions. Cohen’s
Risk of bias was appraised using three methods. RCTs were evaluated using Cochrane’s Collaboration Tool for Assessing Risk of Bias (Higgins et al., 2011). Studies were assigned low, medium, or high, risk of bias for the following categories: selection bias, performance bias, detection bias, attrition bias, and reporting bias. Non-randomised studies were assessed using the Risk of Bias in Non-randomised Studies of Interventions (Sterne et al., 2016). Studies were assigned a low, some concern, or high risk of bias for the following categories: confounding, selection of participants, classification of intervention, deviations from intended interventions, missing data, measurement of outcomes, selection of the reported result. Case studies were assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports (2020). A second rater randomly assessed 10% of articles, and 80% agreement was obtained.
Data analysis
Comprehensive Meta-analysis Version 4 (CMA V4; Borenstein, 2022) was used to conduct the meta-analysis. The authors assumed that the true effect studies would vary given the range of methodologies and samples, and therefore ran the analysis using a random effects model (Borenstein, 2022). Hedge’s
Subgroup analysis was conducted to assess the pooled effect size of treatment conditions against control conditions. The authors hypothesised that treatment groups would perform significantly better than control conditions. Moderation analysis was also conducted to assess for any effects of age of participants (adolescent, college, mixed), intervention type (intervention or control), and intervention setting (group or individual).
Results
Systematic review
Results of the search strategy
Following a comprehensive search, a total of 57 published articles were found to assess the impact of an intervention on PA scores in the context of musicians. Refer to Figure 1 for a comprehensive description of the search strategy.

PRISMA Flow Chart of Study Selection Process (Page et al., 2021).
Demographics, assessment and outcomes measures
Please refer to Table 1 for details on the demographic, assessment measure, and outcomes measures in the studies.
Descriptive Statistics for Included Studies.

Participant characteristics
There were a total of 1,639 participants across the 57 studies, with sample sizes ranging from 1 to 84. The mean age of participants 25.6 years, and the median was 24. The mean percentage of female participants across studies was 64.2%.
Study design characteristics
The study designs of included papers were: 25 RCTs (44%), 24 experimental (non-randomised) trials (E; 42%), and 8 case studies (14%). A total of 32% of studies included a follow-up outcome measure.
Assessment measures
Most studies relied on participant self-report or self-identification as experiencing PA (40%), while others used clinical interviews (11%), or structured diagnostic measures (9%). Of the structured diagnostic measures, the Structured Clinical Interview for
Outcome measures
Across studies, there was some inconsistency in the use of a specific measure to assess PA. Many studies used a specific PA scale (63%), with the Kenny Music Performance Anxiety Inventory (K-MAPI and MPAI-A; Kenny, 2009, 2011) and Performance Anxiety Inventory (PAI; Nagel et al., 1989) used most frequently. Only six studies (11%) use a clinical interview, most of which were case studies. A State/Trait anxiety measure was also commonly used (54%), such as the State Trait Anxiety Scale (38%, STAI; Spielberger, 1983), often in conjunction with another PA measure. Several studies included a physiological measure to assess PA, such as pulse or blood pressure (33%). Performance quality was also measured to assess the impact of anxiety on performance (35%), in addition to including a stress/depression index (21%). A proportion of studies used other outcomes measures to help answer their specific research questions (41%). A small proportion of studies relied on clinician judgement and subsequently did not report using any psychometric outcome measures (7%).
Treatment programme characteristics
A wide variety of treatments were utilised to target PA, focusing on either trait (characteristic) or state (situational) anxiety. The studies that targeted state PA did so in manufactured performance environments to elicit an analogue experience to performing in front of a naturalistic audience.
Of the 57 papers included in this review, the majority utilised a form of CBT to assess a reduction in PA symptoms. Yoga, hypnotherapy, pharmacotherapy, and music therapy were the next most common treatments. A large portion of studies assessed novel treatments, such as specific skills courses to target PA. A summary of the treatment characteristics is found in Table 2.
Summary of Interventions for Performance Anxiety in Musicians.

Papers included in the meta-analysis.
Treatment results summary
Cognitive-behavioural therapies
A variety of treatments fall under the umbrella of CBT (i.e., traditional CBT, individual cognitive or behavioural components, ACT). Thirteen studies reported use of a traditional CBT intervention, five studies used ACT, two studies used systematic desensitisation (i.e., exposure) and two used virtual reality (VR). Treatments varied in application (individual vs. group psychotherapy vs. clinician training music teachers). In traditional CBT interventions, cognitive (i.e., cognitive restructuring, thought challenging) and behavioural (i.e., behavioural activation, exposure) strategies were effective, while acknowledging the beneficial impact of non-specific therapeutic factors (i.e., therapist modelling, the therapeutic relationship, active engagement). Within the ACT interventions, a reduction of ‘experiential avoidance’ was noted as a factor contributing to some reductions in PA.
Pharmacotherapy
Seven studies employed pharmacotherapy to reduce PA experienced by participants. Each study adopted a double-blind randomised crossover design in relation to a repeated live performance. Results were not able to demonstrate a clear reduction in PA across studies; however, some studies found that trait anxiety and performance quality improved following the intervention. Participants appeared to consistently self-report stable PA.
Hypnotherapy
Three studies used hypnotherapy as the mechanism to reduce the level of PA experienced by participants. Results showed an increase in enjoyment during performances; however, when compared with Eye Movement Desensitisation and Reprocessing (EMDR), EMDR was demonstrated to be more effective at reducing both trait anxiety and self-reported PA.
Yoga
Four studies assessed a yoga intervention for PA. Results demonstrated that PA scores significantly reduced following the intervention, particularly during ‘solo’ performances.
Music therapy
Three studies used a unique technique to reduce PA in musicians. Studies varied significantly in their treatment approach, with a focus on reducing distress. Results showed active engagement in a music-based therapy programme encouraged performance development and reduced overall stress. Statistical significance, however, was not obtained.
Other
Fourteen studies used a unique mechanism to target PA symptoms. These included psychodynamic therapy, biofeedback, music analysis, audition training, performance skills courses, and the Alexander Technique. Results varied significantly with difficulty assessing true change in PA scores. Many participants appeared to self-report reductions in PA; however, many studies did not include any psychometric measures.
Overall treatment effects
Overall treatment effects were assessed by measuring the effect size of the impact of the intervention on each group. Means and standard deviations were used to calculate the Cohen’s
Risk of bias
Randomised controlled studies (RCTs) were assessed using Cochrane’s Collaboration Tool for Assessing Risk of Bias (Sterne et al., 2019). Non-randomised controlled studies were assessed using the Risk of Bias in Non-randomised Studies of Interventions (Sterne et al., 2016). Risk of bias for Case Studies was assessed using the JBI Critical Appraisal Checklist for Case Reports (Moola et al., 2020). Results can be found in Tables 3 to 5. The overall risk of bias for the studies included in the review is low–moderate, with a lack of detailed information on study design and participant awareness noted as key contributors to studies falling in the moderate risk of bias range. For RCTs, ‘deviation from intervention’ was deemed ‘unclear’ for several studies, notably where the authors were unable to determine if participants were at all aware of the condition they were placed in or whether the authors took into consideration their facilitation of interventions as impacting their overall interpretation of results. For non-randomised studies, similar queries around the possibility of confounding participants’ understanding of the treatment and possible impacts on treatment effects, in addition to general reporting of results. For case studies, many did not report adequate outcome measures or results to demonstrate meaningful change or impact of the intervention. These findings are in line with the results of Fernholz et al. (2019) where methodological shortcomings were identified, including similar difficulties with participant selection, diagnostic tools, and issues with allocation.
Risk of Bias for Randomised Controlled Trials.

Risk of Bias for Non-Randomised Trials.

Risk of Bias for Case Reports.

Meta-analysis
Results of the search strategy
A total of 25 published RCTs were found to assess the impact of an intervention on reducing PA scores in participants. Of these, data for only 16 studies were available following contact with authors.
Participant characteristics
There were a total of 543 participants included across the 16 studies. Samples sizes ranged from 16 to 70, with the mean age of participants 25.7 years. The mean percentage of female participants was 63.7%.
Assessment and outcome measures
All except one study relied on participant self-report of PA. One study used the ADIS (Silverman & Albano, 1996), while the remaining studies did not report a diagnostic measure. While having a specific outcome measure was an eligibility criterion for this study, multiple PA measures were used. The STAI (Spielberger, 1983) was used commonly as a secondary anxiety measure.
Overall treatment effects
Hedge’s

Forest Plot of Hedges’
For control groups (
The between-groups analysis indicated a significant difference between the intervention and control groups,
Given the support for CBT the suggested efficacious intervention for PA (Brugués, 2011; Fernholz et al., 2019), we wanted to compare the effect sizes of CBT against other interventions. However, given the significant variability of interventions that fall under the cognitive-behavioural umbrella, any analysis would have been met with significant variability/discrepancy. As such only an intervention versus control analysis was completed.
Moderators
The categorical variables of type of intervention delivery (individual or group) and age of participants (adolescents, college students, or a mixture of ages) were explored in a meta-regression analysis for PA symptoms using the random effects model. Two separate meta-regressions found that there was no significant impact detected for intervention delivery,
Publication bias
Funnel plot (Figure 3) examination indicated a skew towards smaller studies being included with a larger effect size. One study demonstrated significant publication bias. Trim and fill analysis under the random effects model remains unchanged.
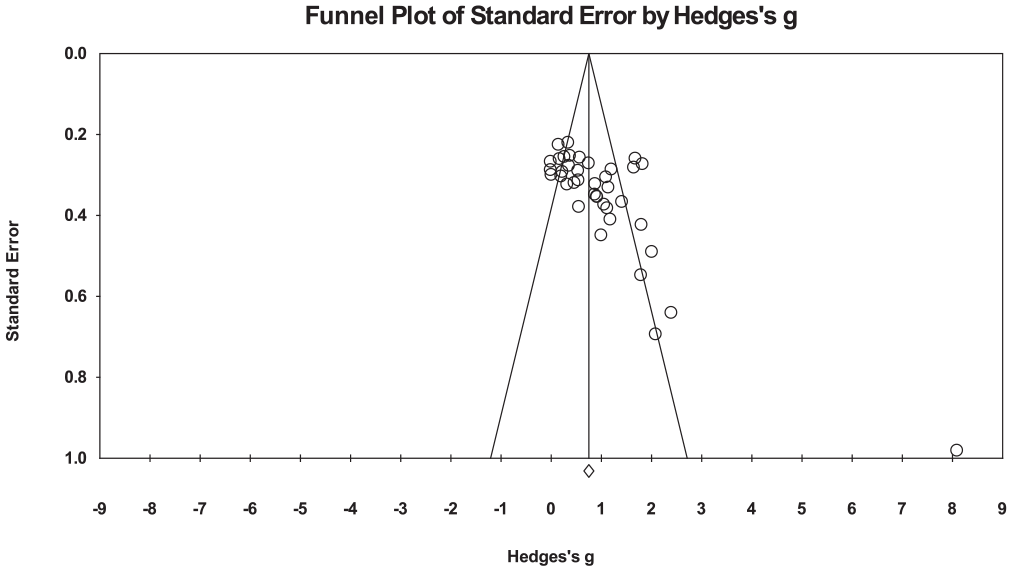
Funnel Plot of Standard Error by Hedges’
Discussion
The large number of studies included in this systematic review and meta-analysis is evidence of the volume and breadth of research that is actively investigating efficacious treatments for PA in musicians. Building on the work of Fernholz et al. (2019), this systematic review presents an updated review of published articles exploring treatments to reduce PA in musicians across the lifespan. The broad inclusion criteria utilised culminated in the inclusion of 57 papers, with randomised controlled and non-randomised experimental designs, as well as case studies that explored a wide range of treatment modalities comprising individual and group formats, personalised and standardised interventions, and both short- and long-term treatment. The current review additionally aimed to include a standardised assessment of research quality and treatment effectiveness. To the authors’ knowledge, this is the first study to systematically review interventions for PA in musicians across the lifespan in addition to assessing study quality and including a meta-analysis.
The systematic review found a substantial number of intervention approaches were used to target PA symptoms in musicians across the lifespan. CBT was noted as the most studied treatment approach, with some interventions specifically targeting a core component of CBT (i.e., cognitive restructuring, systematic desensitisation, or exposure). This finding is in line with recommended interventions for SAD (Andrews et al., 2018), where CBT is identified as the first line of treatment. A vast number of studies explored novel treatments, with skills and performance classes emerging as a popular way to target PA among college and younger musicians. Many of the ‘other’ interventions assessed focused on modifying the way in which interventions were delivered (i.e., skills courses and seminars). Interestingly, participant preference resulted in differences in approach success, with some participants preferring more cognitive approaches (Kendrick et al., 1982), while others benefitted more from behavioural interventions (Lazarus & Abramovitz, 2004). Therapeutic factors were also identified to contribute to the outcome of studies, including therapist modelling (Norton et al., 1978) and the importance of the therapeutic relationship (Sweeney & Horan, 1982). Unsurprisingly, participant engagement was also noted as a key component to participant results (Osborne et al., 2007). The timing of interventions was also explored, with Su et al. (2010) finding that certain components of interventions given prior to 30 min before a performance were not effective. These findings are valuable for the development of further interventions, which can continue to assess specific cognitive components to target in treatment, therapeutic factors involved in the change process, and the timing of interventions to best support outcomes.
The quality and impact of interventions targeting PA in musicians varied. A wide range of studies were deemed effective, spanning from children to college musicians to professionals; while others were unable to demonstrate superiority to control groups, or the significance of findings could not be maintained at post or follow-up. Many findings needed to be interpreted with caution, as often participants with higher pre-intervention scores had the greatest reduction in PA symptomology, even though many still met the clinical cut-off for severe PA, necessitating greater emphasis on achieving clinically significant outcomes.
The quality of papers included in this review also supports recommendations for the continued development of rigorous research methods and practice. Under-reporting of components (i.e., participants being aware of treatment characteristics, or the impact of researchers running interventions) was often the key difficulty in assessing any impact of bias. It is recommended that future studies ensure the reporting of all methodological components, particularly when including characteristics about the running of interventions (participant awareness of the intervention/controls available, length of treatment in keeping with reporting guidelines). Uncontrolled trials and case studies continue to have merit in the emerging assessment of processes involved in treatment effectiveness; however, more rigorous RCTs are required. When assessing for confounding factors, it is suggested that studies also examine intervention-related factors such as engagement, therapeutic relationship, and the individual processes being targeted. Overall, these findings are in line with Fernholz et al. (2019), indicating an improvement in the quality of studies being developed.
The meta-analysis demonstrated that for RCTs, interventions for PA were found to be more effective than controls. The moderators of intervention types (group or individual) and participant age (adolescent, college, or mixed) did not demonstrate more significant contributions to outcomes. The original hypothesis, that cognitive-behavioural interventions would be the most effective, was not able to be tested. Given the limited number of ‘similar’ studies that included traditional elements of CBT, any comparison would be misleading. The significant variability and heterogeneity among the data indicates the need to analyse studies based on shared components, which was not possible here. The findings of Faur et al. (2022) indicate that CBT is effective in treating PA in musicians, with future studies examining the specific cognitive and behavioural components that contribute to the effectiveness of cognitive-behavioural-based therapies being warranted.
Kenny (2005) and Brugués (2011) highlighted the lack of methodological rigour as a matter of urgency more than a decade ago. The findings of this article highlight the development of more sound research approaches to PA in musicians; however, further development is still warranted. This is perhaps a symptom of the larger challenge around the definition, assessment, and disorder-specific model used in the field of PA. The spurious number of assessment tools, lack of conceptual focus, and lack of replicability continue to present substantial challenges. The wider acceptance and incorporation of models for SAD (Barlow, 2002; Clark & Wells, 1995; Heimberg et al., 2014; Hofmann, 2007; Rapee & Heimberg, 1997) is supported by the launch of the
One key component that has not been assessed in this review is the basis of the interventions conducted. That is, what theoretical lens is being applied to justify the intervention chosen for the population. On face value, many studies used a transdiagnostic approach, perhaps linking to the use of Barlow’s (2002) triple vulnerability model, highlighted by Kenny (2011), where the reduction in overall anxious apprehension is the basis for intervention. Complementary model components could allow for the further study of the complexities that are suggested in MPA research (i.e., depression/hopelessness, early life experiences, maladaptive schemas, generational, and parental influences). The complexities can be acknowledged, on one hand, but they do not account for the absence of an updated model or reliance on a simplified anxiety induction model. Future reviews should look to assess the theoretical basis of interventions, exploring the relevant mechanisms being targeted which can support more rigorous intervention development, that is, the relevant cognitive processes targeted in SAD treatments, and examine their applicability to PA in musicians, such as has been explored by Osborne and Franklin (2002).
Interestingly, the movement away from interventions simply targeting symptom reduction and working towards ‘optimal performance’ and flourishing was a positive inclusion in recent papers (e.g., Cohen & Bodner, 2019). It was also encouraging to see the emerging recognition that PA in musicians and sport are more interrelated than separate (Braden et al., 2015; Osborne et al., 2014). This could lead to the development of performance skills courses (pre-emptive, rather than post-mortem interventions) such as that of Steyn et al. (2016), Hoffman & Hanrahan (2012), and Cohen et al. (2019). The emergence of therapies such as ACT (in addition to the increased focus on somatic and active therapies, such as yoga) also indicates the growth in less targeted interventions that positively impact other areas of well-being. This supports the development of incorporating lifestyle and general well-being components into interventions.
A stepped-care approach for mild and moderate anxiety could benefit individuals with mild or a recent experience of PA; such approaches are starting to manifest in the literature (Osborne et al., 2014). Individuals who specifically identify challenges in one area of performance (e.g., fear of judgement) could be directed to a specific skills-based course prior to being referred to more intensive 1:1 formalised cognitive-behavioural treatments, whereas those who identify a fear of making a mistake (e.g., playing a wrong note) could be supported through technical and practice-based training. Further developments would need to be made regarding methodological consistency for such studies, noting appropriate measurement of PA and intervention fidelity (i.e., from trained professionals such as psychologists). Within a stepped-care approach, consensus could be developed on the targeting of specific processes.
Limitations
The conclusions of this study are impacted by the breadth of studies included in this article. The large number of studies included demonstrates difficulty within the literature in synthesising the necessary core features of interventions to achieve symptom reduction. The specific focus on English and published papers also reduces the breadth that is possible for this review, recognising the significant number of unpublished dissertations that were excluded. With those in mind, and while the quality of the papers may have been impacted, the scope of the interventions provided and number of participants available would have been greater. The significant number of papers included in the meta-analysis also limits the specificity of the results generated. As there was significant heterogeneity, the efficacy of CBT when compared with other interventions was not possible to assess. Future research should also examine the theoretical underpinnings of the interventions available, in addition to the findings based on the assessment measures used. Many interventions rely on unique self-report measures; it would be useful to recognise the relative strength of findings based on standardised assessment tools and symptom outcome measures.
Conclusion
The aim of this systematic review and meta-analysis was to assess the efficacy of available interventions targeting a reduction in PA symptoms in musicians across the lifespan. The results of the systematic review identified a vast array of available treatments, with a focus on targeting general cognitive and behavioural components of PA. The meta-analysis found that in RCTs, interventions for PA in musicians are more effective than for controls, demonstrating a large average effect size relative to wait-list controls. Moderators of intervention type (individual vs. group) and age of participants demonstrated no significant effect on treatment efficacy.
Based on the findings of this study, there is evidence for the recommendation of CBT as the first line of treatment for PA in musicians. This recommendation is based predominantly on the effect sizes of interventions (medium to large). Recognising the variation in treatment application and results, emphasis should also be placed on assessing other factors associated with intervention success, including maintaining processes and identifying other ‘active ingredients’ in treatment to reduce PA for musicians across the lifespan.