
Abstract
Depression is the leading cause of disability world-wide (Whiteford et al., 2013). The risk and protective factors that contribute to the development and maintenance of depression are important for understanding how to prevent the pain and suffering of those experiencing symptoms and to relieve the burden on health care systems. Mattering is a construct salient to depression. It refers to the tendency to evaluate oneself as important or significant to others (Flett, 2018a; Marshall, 2001). Lower levels of mattering have been associated with depression symptoms both cross-sectionally and longitudinally (e.g., Taylor & Turner, 2001). However, one issue with the longitudinal studies conducted to date is that most include only two time points of assessment, thus precluding a true examination of temporal ordering. To our knowledge, one study examined mattering over three time points (i.e., Marshall et al., 2010) but focused on growth trajectories and none have exceeded three time points. In the present study, we examined depression, mattering, and anti-mattering across four years of development in a cohort of young adults assessed yearly from age 20 to 23 using a cross-lagged panel model (CLPM).
Depression Symptoms
The median age of onset for depression is 30 years, although many first onsets occur in adolescence and young adulthood, and recurrence is common (American Psychiatric Association [APA], 2013; Kessler et al., 2005). For those who experience a depressive episode in adolescence, about 45% will have another episode in young adulthood, before age 24 (Lewinsohn et al., 1999). In a systematic review of the development of depression symptoms from ages 15–25, depression symptoms were found to peak in late adolescence (ages 15–17) and decline in young adulthood. The peak and decline are similar when trajectory groups are examined (i.e., low, moderate, and high groups increase in late adolescence and decrease thereafter; Schubert et al., 2017). Given this developmental pattern, it is important to examine factors that may be related to the promotion or maintenance of depression at a time in which there is a high reoccurrence rate. In the present study, we examined how mattering and not mattering related to symptoms of depression across 4 years of young adulthood.
Mattering and Depression
Those with a strong sense of mattering have a perception of being recognized for their uniqueness or of being truly understood as a person (Flett, 2018a). Mattering can vary over time in relation to the accrual of recent interpersonal interactions at different times in the lifespan, as well as based on recent experiences with others, which can influence how much a person believes they matter to others. Negative interpersonal interactions or the absence of positive interpersonal interactions can contribute to lower feelings of mattering. Relationships are formed and lost over the lifespan and even changes in roles can relate to an increase or decrease in mattering. The discrepancy between one’s ideal and current level of mattering to others relates to feelings of satisfaction or dissatisfaction. In one study, Marshall et al. (2010) examined growth trajectories of mattering to mothers, fathers, and friends over three years in an undergraduate student sample with ages ranging from 17–21 at the first time point. Results indicated that mattering to fathers and friends was stable over time and mattering to mothers decreased over three years in young adulthood.
Mattering can be viewed as an interaction between the individual and the interpersonal environment, whereby the interpersonal environment impacts the individual and the individual impacts the interpersonal environment (Flett, 2018a). Although mattering can include the behavior of others, the perception of mattering is the combination of an interpersonal interaction and the interpretation of that interaction. Some individuals may not have an accurate impression of mattering to others; some may have perceptions of mattering that are more favorable (e.g., those with narcissistic personality traits), while others may have an impression that is more unfavorable than may rationally be the case (e.g., those with internalizing problems).
Mattering and anti-mattering are construed not as opposite ends of a continuum but are separate constructs where mattering activates approach tendencies and anti-mattering activates avoidance tendencies (Flett, 2018a). The construct of anti-mattering relates to acquiring a history of multiple negative interpersonal experiences that demonstrate a lack of worth for attention or demonstrate insignificance of the target. These experiences, particularly when they are salient or painful, can become overgeneralized where individuals come to believe they do not matter to anyone. The anticipation of continued negative interpersonal experiences and the related feeling of not mattering may then lead to the avoidance of interpersonal interactions and relationships.
Depression symptoms and mattering are negatively associated concurrently in young adults (Cha, 2016; Dixon & Kurpius, 2008; Flett et al., 2012; Flett et al., 2020; Rosenberg & McCullough, 1981; Taylor & Turner, 2001). In cross-sectional analyses, lower mattering partially mediated the positive relation between socially prescribed perfectionism and depression symptoms (Cha, 2016; Flett et al., 2012). In another cross-sectional study, the importance to others subscale of mattering mediated the relation between self-criticism and depression symptoms (Joeng & Turner, 2015). A concurrent negative association of depression symptoms and mattering in dating relationships was also found when controlling for prior depression symptoms (Nash et al., 2015). Of note, in all of these cross-sectional studies, mattering and depression symptoms shared a negative association.
Taylor and Turner (2001) conducted one of the first longitudinal studies on mattering and depression symptoms and found that mattering in adults (i.e., 3415 participants, age 18–55 years) was negatively associated with depression symptoms one year later after accounting for prior depression symptoms. Gender moderated this association such that mattering and depression symptoms were associated over time for women but not men. Mattering also negatively predicted depression symptoms from adolescence to young adulthood after accounting for prior depression symptoms, stress, socioeconomic status, and ethnicity (Turner et al., 2004). Mattering was shown to moderate stress or have a stress-buffering effect on depression symptoms in this study. Elliott et al. (2005) examined the associations among mattering, self-esteem, depression, and suicidal ideation and found that the relation between mattering and suicidal ideation was fully mediated by self-esteem and depression. In another study, the associations between mattering (i.e., mattering to mother, father, and friends) and depression symptoms were examined over two time points in adolescence (i.e., age 11–15 at the first time point and assessed again one year later) using a two-wave CLPM (Marshall et al., 2019). Cross-lagged panel models account for the stability of constructs and the associations within time when examining bi-directional associations among constructs across time. In this study, a positive association from mattering to friends and later depression symptoms and a negative association between depression symptoms and later mattering to mothers were found. They also found concurrent negative associations among mattering and depression symptoms at both time points for mattering to mothers and fathers but only at the first time point for mattering to friends. The authors suggested co-rumination as an explanation of the positive association between mattering to friends and later depression symptoms. Although individuals with depression often have negative interpretations of others, in this study there were no associations between depression symptoms and later mattering to fathers or friends, but there was a negative association with mattering to mothers, suggesting that how mothers were responding to depressed youth may relate to youth’s perceptions of not mattering.
Longitudinal studies on mattering have been limited to two time points, and while some studies account for prior depression symptoms, most assume that mattering leads to depression and do not account for the possibility that depression symptoms may also impact mattering. Marshall et al. (2019) did examine both directions of association in a CLPM; however, this study used two time points. Further, although mattering to specific people or groups (e.g., mother, father, and friends) may be important, examining specific people or groups may miss some important contributors to mattering in general (e.g., romantic partners and co-workers). Thus, the associations of the general construct of mattering may be important in understanding the links to depression symptoms.
The construct of anti-mattering is in the early stages of development and has been examined far less frequently than mattering (Flett, 2018a). Some studies have found strong cross-sectional associations between loneliness and anti-mattering (MacDonald et al., 2020; McComb et al., 2020). In a recent study, a positive association between anti-mattering and distress (i.e., stress, anxiety, and depression) was found, although these data were collected during the COVID-19 pandemic (Besser et al., 2020). One study examining the validity of the anti-mattering scale showed a positive association between anti-mattering and depression symptoms (Flett et al., 2022). There has been little research to make predictions regarding anti-mattering and depression symptoms. Nevertheless, anti-mattering and depression symptoms should be theoretically more closely linked than low mattering. In the cognitive triad of depression (Beck et al., 1979), negative cognition regarding the self, others, and the world are salient in maintaining depression symptoms. The belief that one does not matter to others is a negative belief about the self in relation to others that may become more entrenched in the presence of depression symptoms. Individuals with depression symptoms tend to view themselves negatively and interpret experiences negatively, including interpersonal experiences. For example, they may be treated poorly by other individuals and overgeneralize these experiences as not mattering to anyone. They may then begin to avoid others, which in turn reduces opportunities to provide evidence to challenge this assumption. Those interactions that do occur tend to be viewed in an overly negative manner, where individuals are more likely to find evidence of their belief of not mattering. When individuals are still approaching others, as in the case of low mattering, there may at least be the possibility for more frequent opportunities that may challenge the idea of mattering less than when individuals are actively avoiding social interactions. The perception of being treated by others as though one does not matter (whether this has occurred, is a negative perceptual bias, or both) can also lead to further low mood and less desire to interact with others.
It is important to know whether (1) mattering or anti-mattering predicts depression symptoms, or (2) depression symptoms impact mattering or anti-mattering, or if (3) they exist in consort. Lower mattering or anti-mattering predicting depression symptoms may imply low mattering or anti-mattering is a mechanism to target in the prevention or early intervention of depression symptoms. Whereas, if depression symptoms predict mattering or anti-mattering, then it is possible that lower levels of mattering or higher levels of anti-mattering may be a factor in the maintenance of depression symptoms and mattering or anti-mattering may be a possible target in treatment. If a reciprocal association is found over time that accounts for the level and stability of depression symptoms, then intervening on mattering or anti-mattering may be most fruitful in the prevention and treatment of depression symptoms.
Present Study
The stress-generation hypothesis suggests that individuals with a history of depression or depression symptoms tend to experience later stressful events and specifically, stressful events that involve interpersonal stressors (e.g., conflict in relationships) as opposed to other stressful events that are independent of individual influence (e.g., accidental death of a loved one; Hammen, 2005). Symptoms-driven models support a similar notion, that depression symptoms can impact interpersonal areas of functioning. For example, depression symptoms have been consistently linked to later peer problems (i.e., peer victimization, peer rejection, and low peer acceptance) in CLPMs (e.g., Kochel et al., 2012; Krygsman & Vaillancourt, 2017; Vaillancourt et al., 2013). The interpersonal risk model suggests that negative interpersonal interactions pose risk for the development of subsequent depression symptoms (e.g., Cole, 1990; Ttofi et al., 2011). The transactional model emphasizes the nature of the individual as changing over time and where the individual impacts the environment and the environment impacts the individual, which supports bi-directional associations over time (e.g., Sameroff, 2009). The transactional model better describes the theoretical description of mattering and anti-mattering denoted by Flett (2018a). Although some short-term longitudinal studies have shown links between mattering and later depression symptoms, researchers have not considered both directions of association over more than two time points. The temporal priority has important implications regarding what to focus on during treatment.
Our aim was to examine the associations of depression symptoms, mattering, and anti-mattering over four years of development in young adulthood using a CLPM. Cross-lagged panel models have an advantage of being able to examine the relations from mattering (or anti-mattering) to later depression symptoms, and the reverse, while attenuating for the within- and across-time associations among these constructs (Masten & Cicchetti, 2010). This approach allowed us to examine the dynamic unfolding of depression symptoms, mattering, and anti-mattering over time and the consistency of their associations. Our study is uniquely suited for this aim because, to our knowledge, no other studies to date have examined depression symptoms, mattering, and anti-mattering, assessed annually, over four years.
Researchers have consistently documented that having lower socioeconomic status and being female are associated with elevated depression symptoms (APA, 2013; Musliner et al., 2016; Schubert et al., 2017). Given the associations with income, education, and gender with depression symptoms, these constructs were accounted for as covariates. The last data point at age 23 occurred within the first several months of the COVID-19 pandemic, thus we examined whether fear of COVID-19 was related to depression symptoms, mattering, and anti-mattering by adding this construct as a covariate.
Methods
Participants
Participants were drawn from the McMaster Teen/Young Adult Study, a longitudinal study examining continuity and change in mental health, bullying, and academic achievement that began in spring of 2008. Participants included 875 youth (age 10 at study commencement) and their parents (in years 1–8) recruited from a school board. Youth who participated in two or more time points up to year eight included 701 participants. Participants who provided data in early adulthood (i.e., age 20–23) were selected for the current study. Questionnaires were screened for validity and five individuals were omitted due to invalid responses. These inclusion criteria resulted in a final analytic sample of 452 participants who were on average 19.97 years of age (
Procedures
Young adults provided annual consent and compensation for participation in the questionnaire was $50 in Time 10, Time 11, and Time 12 and $75 in Time 13. Each year bonus compensation was provided for completing the survey within several weeks of consent. In Time 10, a draw for 1 of 2 $100 gift cards was conducted for those who completed surveys within 2 weeks. At Time 11 and Time 12, participants received a $20 bonus for completing the survey within 2 weeks and $10 if the survey was completed within 3 weeks. At Time 13, a $25 bonus was provided to those who completed surveys within 2 weeks of receiving the survey. In Time 8, parents were compensated with a $35 gift card of their choice for participating in the telephone interview and entered into a draw for 1 of 2 $100 gift cards for participating in the telephone interview within 2 weeks. The study has maintained annual ethics approval. Questionnaires were completed online and paper questionnaires were provided for those who preferred the questionnaire in this format or who did not have regular internet access.
Measures
Depression symptoms
Self-reported depression symptoms were measured using the depression subscale of the Behavior Assessment System for Children-Second Edition (BASC-2), the self-report of personality college version (SRP-COL; ages 21–23; 13 items; Reynolds & Kamphaus, 2004). Items were rated as 2 =
Mattering and Anti-mattering
The general mattering scale and anti-mattering scale were used to measure self-reports of mattering (Marcus & Rosenberg, 1987; Rosenberg & McCullough, 1981) and anti-mattering (Flett, 2018a). The scales consisted of five items assessing mattering (e.g., “How important do you feel you are to other people?”) and another five items measuring anti-mattering (e.g., “How often have you been treated in a way that makes you feel like you are insignificant?”). The items were rated on a 4-point frequency scale and response options were 1 =
Given that the literature is new on this topic, we also conducted principal axis factoring with Promax rotation to determine whether mattering and anti-mattering loaded onto different factors in each year. Principal axis factoring has been supported over principal components analysis in that the procedure allows for error (not using all the variance) and in providing more accurate population estimates in Monte Carlo studies (Russell, 2002). For each year of the study, two factors were extracted consistent with mattering and anti-mattering items. The two factors explained between 59% and 62% of the variance across the four time points in the study. Factor correlations were high and negative,
Demographic Features
Demographic information was provided by the person most knowledgeable (PMK) about the child on household income and education of the PMK. Household income was rated in categories ranging from 1 =
Fear of COVID-19
The Fear of COVID-19 Scale was used to assess fear of COVID-19 (Ahorsu et al., 2020). COVID-19 related fear was examined at age 23 using seven items measured along a 5-point Likert-type scale with response options ranging from 1 =
Analytic Plan
A CLPM with full information maximum likelihood (FIML) and maximum likelihood robust (MLR) estimation was performed in Mplus version 8.0 (Muthén & Muthén, 2017). Model fit was assessed using the comparative fit index (CFI) and the root mean square error of approximation (RMSEA). Comparative fit index values of .95 and greater indicated fit was adequate and RMSEA values less than .08 indicated fit was adequate, where lower values indicated better fit (Browne & Cudeck, 1992; Hu & Bentler, 1999). The chi-square test was used as a fit indicator although we also considered the sensitivity to large samples (Kline, 2011). The Satorra–Bentler scaled chi-square difference test was used to test for differences among competing models (Satorra & Bentler, 2001). The Akaike information criterion (AIC) was used to compare non-nested models where lower values represent a better fitting model (Kline, 2011). We began with a base model (Model 1) that included the auto-regressive paths (one-year and two-year), covariances among depression symptoms, mattering, and anti-mattering within the same time point, and the one-year cross-lagged paths among depression symptoms, mattering, and anti-mattering. Next, the auto-regressive paths, covariances, and cross-lagged paths were each constrained to be equal over time to determine whether the auto-regressive paths, covariances, and cross-lagged paths were invariant over time (Models 2–6). To test whether the symptoms-driven paths from depression symptoms to mattering and depression symptoms to anti-mattering were contributing to the model, these paths were constrained to 0 and this model was compared to Model 1. This was completed separately for depression symptoms to mattering (Model 7a) and depression symptoms to anti-mattering paths (Model 7b). To test whether the interpersonal risk paths were contributing to the model, the paths from mattering to depression and anti-mattering to depression symptoms were constrained to 0 and the model was compared to Model 1. This was completed separately for mattering to depression symptoms (Model 8a) and for anti-mattering to depression symptoms (Model 8b). Because the symptoms-driven paths and interpersonal risk paths were theoretically relevant, they were freely estimated in the model with the appropriate cross-lagged constraints irrespective of the statistical significance of the paths. When invariance constraints did not cause a deterioration in fit compared to the baseline model, these constraints were retained in the final model (Model 9) and when the constraints did differ from the baseline model, then the paths were allowed to be free in the constrained model. In Model 10, covariates were added to the final model to determine if these constructs had an impact on the significance of paths or if the results remained after accounting for these constructs. The Benjamini-Hochberg (B-H) false discovery rate (FDR; Benjamini & Hochberg, 1995) was applied to the parameters within the final model to account for multiplicity (Cribbie, 2007).
Results
Missing Data
Those in the analytic sample (
Descriptive Statistics
Descriptive Statistics of Depression Symptoms, Mattering, and Anti-Mattering.

Cross-Lagged Panel Model
Model Fit Statistics for the Cross-Lagged Panel Model of Depression Symptoms, Mattering, and Anti-Mattering.
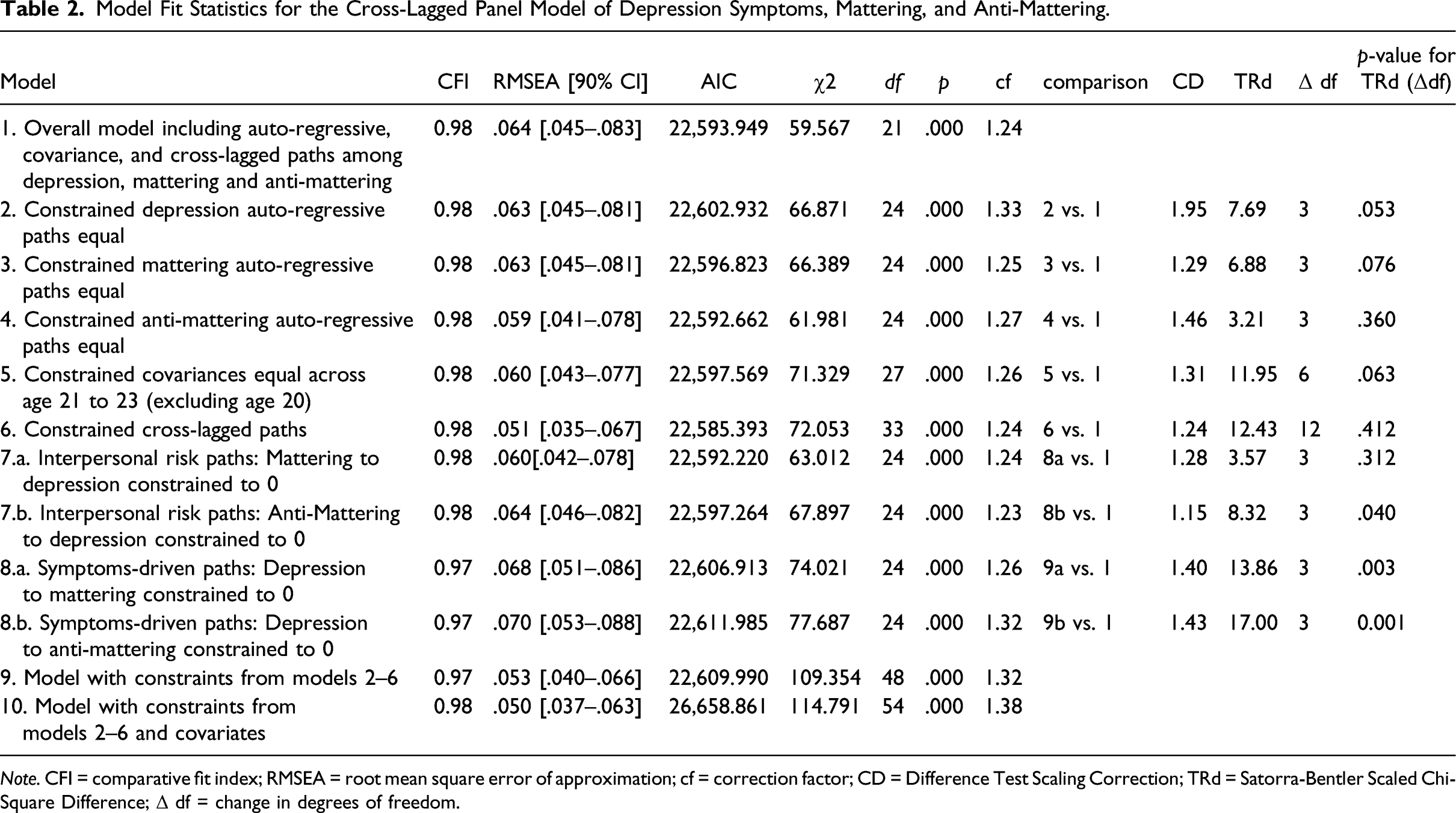
Invariance of similar paths across time was examined to determine if the unstandardized paths could be constrained to be equal across time or should be freely estimated. We found that similar auto-regressive paths for depression symptoms, mattering, and anti-mattering could each be constrained to be equal across time (Models 2–4). We constrained auto-regressive paths of depression symptoms to be equal and this did not have an impact on the model. Nor did constraining mattering auto-regressive paths equal or constraining anti-mattering paths equal impact the overall model. Residual covariances within-time were constrained to be equal across ages 21, 22, and 23 each for depression symptoms, mattering, and anti-mattering (Model 5) and this was not found to impact the overall model. Finally, similar cross-lagged paths were constrained to be equal across time each for depression to mattering, depression to anti-mattering, mattering to depression, anti-mattering to depression, mattering to anti-mattering, and anti-mattering to mattering (Model 6). This did not have an impact on the overall model fit. Next, cross-lagged paths related to interpersonal risk paths (i.e., mattering to depression [Model 7a] and anti-mattering to depression [Model 7b]) were constrained to 0 and this was compared to Model 1. Model 7a did not result in a deterioration of fit. Model 7b resulted in deterioration of fit indicating that the interpersonal risk paths were making a significant contribution to the model for anti-mattering but not mattering. In Model 8a and Model 8b, the symptoms-driven paths were constrained to 0 and compared to the constrained model which resulted in a deterioration of fit indicating the symptoms-driven paths were also making a significant contribution to the model. Although the mattering to depression paths were not contributing to the model statistically, we retained them in the model due to being theoretically relevant. Thus, a constrained model (Model 9) was built with the above constraints imposed on Models 2 through 6.
Due to the number of parameters in the model, to account for multiplicity, the B-H FDR was applied to the parameters in the model. This resulted in a FDR of Cross-lagged panel model of depression symptoms, mattering, and anti-mattering.
The covariates of gender, household income, and parental education were added to the model. Following the B-H correction, the same paths remained significant in the model as in Model 9. Household income negatively predicted depression symptoms at age 21, parental education positively predicted mattering at age 20, and gender positively predicted depression symptoms at age 20 and anti-mattering at age 20 (i.e., women > men). COVID-19 fear showed no statistically significant associations with any constructs in the model. Given that the AIC was considerably higher for the model with the covariates, and although there were a couple significant associations, the covariates did not impact the significance of any of the associations in the model and therefore, Model 9 was selected as the final model.
Discussion
We examined the dynamic interplay of depression symptoms, mattering, and anti-mattering across four years of early adulthood using a CLPM. We found that a transactional model best described the associations between anti-mattering and depression symptoms over time and a symptoms-driven model best described the associations between mattering and depression symptoms over time. We also found considerable consistency within each construct and the associations among constructs over a 4-year period. All auto-regressive paths, associations within time at ages 21 to 23, and all cross-lagged associations demonstrated equality across time. Finally, these results remained when accounting for covariates of education, income, gender, and COVID-19 fear.
These findings suggest that there are some important differences between mattering and anti-mattering that support the assertion that they are indeed related but distinct constructs (Flett, 2018a). First, the correlations among mattering and anti-mattering within time were strong (.50; Cohen, 1992), but they were not collinear (>.80; Mason & Perreault, 1991) and ranged from .51 to .61. The magnitude and invariance of auto-regressive paths for mattering and for anti-mattering over a 4-year period at 1-year intervals within the CLPM was interesting. This suggests that, at least in young adulthood, there is considerable stability in mattering and anti-mattering over time and the strength of the association from one year to another is similar. The differential associations of depression and mattering and depression and anti-mattering over time also support the distinction between the constructs. Mattering and anti-mattering items were shown to load on different factors. Taken together, our findings provide some support that the constructs are distinct.
One of the theoretical distinctions between mattering and anti-mattering is that mattering relates to approaching interpersonal relationships and anti-mattering relates to avoiding interpersonal relationships, where the avoidance occurs likely because of the emotional pain that anti-mattering evokes (Flett, 2018b). Future research would be helpful in examining whether the avoidance of emotional experiences is indeed uniquely linked with anti-mattering. This would further assist in distinguishing the constructs. Avoidance of emotional experiences is a common issue not only with depression but with a variety of other mental health problems such as anxiety disorders and posttraumatic stress disorder (PTSD; Kennedy & Barlow, 2018). Avoidance of emotional experiences could at least partly explain the association between anti-mattering and depression symptoms. If this is the case, anti-mattering may also relate to anxiety disorders, and PTSD as well as depression.
Anti-mattering and depression symptoms shared a reciprocal positive relation over time. That is, after accounting for the within-time associations between anti-mattering and depression symptoms and across-time stability within constructs, anti-mattering predicted depression symptoms one year later and depression symptoms predicted anti-mattering one year later, which occurred consistently from ages 20 to 23. In fact, the relation did not vary in magnitude over time. Although we do not know if depression symptoms or anti-mattering started this cascade, the presence of both directions of association has some important implications for intervention. Results suggest that intervening on anti-mattering may have an impact on later depression symptoms and that lowering depression symptoms may have an impact on anti-mattering. More research is needed to determine whether a change in one domain leads to a change in another. Further, the consistency over time among these constructs also suggests that a clear plan on how to intervene when these symptoms are already in place will be needed. Importantly, we likely need to intervene as early as possible to prevent anti-mattering from becoming consolidated and the related beliefs from becoming entrenched. The consistency of the mattering and anti-mattering auto-regressive paths indicates there is already considerable stability of these constructs over time during young adulthood. Examining these constructs at younger age groups may reveal the ages or conditions under which within-person heterogeneity is greatest, which could offer insight on the optimal time to intervene prior to the consolidation of low mattering or anti-mattering. Most first episodes of depression begin in adolescence (APA, 2013; Kessler et al., 2005), which suggests a need to examine how these associations unfold in younger populations to have the greatest impact.
We found that depression symptoms led to later mattering and had a consistent negative association. This may mean that high depression symptoms relate to later lower mattering but also that lower depression symptoms may relate to higher mattering. This highlights the importance of considering both directions of the association; it may be the case that the association is driven by increases in depressive symptoms because when both were examined together, we found that the depression symptoms were consistently and negatively associated with later mattering but not the reverse. As mentioned, perceptions of mattering may or may not be an accurate perception of reality; those with depression symptoms tend to have a bias toward negative interpretations of the self, others, and the future (Beck et al., 1979). However, this explanation is not consistent with the findings of Marshall et al. (2019) where a negative association was found between depression symptoms and later mattering to mothers but not mattering to fathers or friends. If the negative perceptual bias was driving the effect, we would likely see some consistent negative views across people.
Another possibility is that how others are responding to the behavior of individuals with depression symptoms leads to feelings of low mattering. Interpersonal theories of depression suggest that the interactions of depressed individuals can be perceived as aversive to others and that others may engage in behavior that then promotes negative feedback (Hammen, 1991; Hammen & Shih, 2014; Joiner et al., 1999). Indeed, some of the vulnerabilities that contribute to the development of depression symptoms also impact interpersonal problems, which places individuals at risk for recurrence (Hammen & Shih, 2014). Some of the ways individuals convey they matter to others may include asking what others think, sharing in past and current life events (i.e., positive and negative), or wanting to know about hopes and fears (Flett, 2018a). When an individual has higher depression symptoms, when interacting with another person with a consistent world view (e.g., friends), these individuals may share more negative events, want to know about fears, and ask for their thoughts. These types of behavior may contribute to the perception of being understood and may relate to higher perceptions of mattering relating to later depression symptoms for friends as Marshall et al. (2019) found. Individuals with depression also tend to engage in excessive reassurance seeking, which over time can lead to disengagement in the relationship as the feedback provided repeatedly appears to be ineffective in assuaging the concern (Evraire & Dozois, 2011; Starr & Davila, 2008). This may be perceived by the individual with depression as others not asking about them or wanting to know about them, resulting in the impression that they do not matter. In order to continue to demonstrate behavior that leads to the perception of mattering, individuals interacting with a person with depression may need to be very comfortable with the highly negative content (and have the capacity to be able to manage their own reactions of listening to the negative content) in order for the usual signs of mattering to be conveyed.
Our results suggest that anti-mattering could be intervened upon in the prevention of depression symptoms and both anti-mattering and low mattering may be targets in the treatment of depression symptoms. Although research is needed on how to intervene of mattering, there are some clues in the literature on the intersection of depression symptoms and interpersonal problems. There are multiple cognitive-behavioral applications that could be used to support interpersonal relationships and decrease depression symptoms that are discussed and described by Dobson et al. (2014). As emphasized by Flett (2018a), great care should be taken with the intervention of low mattering and high anti-mattering to prevent inadvertently supporting previously held beliefs related to not mattering. We need to know more about which behavior of others consistently has an impact on mattering and anti-mattering in order to attain evidence-based information on how to intervene on mattering or anti-mattering. We also need to know more about how new environmental experiences may (or may not) become integrated into perceptions of mattering or anti-mattering. Moreover, in the prevention of anti-mattering, those experiencing negative interpersonal events may benefit from assessment for brief counselling support to assist in the prevention of the overgeneralization of negative interpersonal events into aspects of the self. Certainly, approaching those who have experienced any form of negative interpersonal event and those with depression symptoms with unconditional positive regard may assist in integrating the validation and supportive behavior that can lead to a perception of mattering.
Another consideration for those experiencing depression or depression symptoms who present with low mattering or high anti-mattering is that, should these topics be addressed as goals in treatment, additional sessions may be required in order to address these concerns. Indeed, while the onset of depression symptoms is common in late adolescence, there is often significant delay in obtaining treatment for mood disorders of 6–8 years, and the longer the delay, the poorer the outcome (Malla et al., 2018; Wang et al., 2005). Individuals that perceive they do not matter to the community may have difficulty seeking services for depression (Flett, 2018a; Shannon et al., 2019). Experiences of not mattering to the community may support perceptions of not mattering to others, which in turn may further exacerbate or maintain depression symptoms over time. This suggests that those seeking treatment may already have a significant history of depression symptoms, which may also include a history of low mattering or anti-mattering. Research examining interventions of mattering may require consideration of the additional mental health care needs of those presenting with depression symptoms and mattering concerns who have experienced a history of depression symptoms, low mattering, and/or anti-mattering.
Given that the last time point of data collection occurred within the first several months of the COVID-19 pandemic, COVID-19 fear was included as a covariate to determine whether the pandemic may have had an impact on the data. Fear of COVID-19 was unrelated to any of the constructs in the study. Further, we found consistency in associations over time; estimates involving the last time point were not different than prior estimates. This may have been because data were collected at the beginning of the pandemic and there was not yet enough time for an impact to occur. The consistency of depression symptoms, mattering, and anti-mattering and their inter-relations may not yet have been impacted by the pandemic or not impacted in relation to fear of COVID-19.
Strengths and Limitations
Our study had many strengths such as a relatively large sample collected over four time points one year apart, the use of psychometrically sound valid and reliable measures, and accounting for within- and across-time associations when examining cross-lagged paths. In fact, to our knowledge, this study has the longest time period over which depression symptoms, mattering, and anti-mattering have been assessed longitudinally. Examining depression symptoms and mattering over four years has the advantage of being able to examine the consistency of constructs and their inter-relations over time. However, the study was not without limitations.
First, although the sample was randomly drawn from schools with fifth grade classrooms, there was attrition over time, and individuals with higher family income and parental education tended to continue to participate in later waves of the study. Second, we do not know whether beliefs of anti-mattering or depression symptoms developed prior to young adulthood. Given that many episodes of depression begin in adolescence, studies during this period including measures of depression symptoms, mattering, and anti-mattering are needed to determine whether depression symptoms or anti-mattering develop first and the risks of developing anti-mattering. Negative interpersonal interactions of the most salient relationships during adolescence, such as peers, may be good candidates for initiating this cascade. Studies with large samples that examine clinical status as a moderator of the association between mattering and depression symptoms or anti-mattering and depression symptoms may give insight into these associations when individuals are experiencing clinical symptoms or not. Finally, common associations of both depression symptoms and mattering or anti-mattering may give insight into the interpersonal contributions to the maintenance of depression symptoms. For example, rejection sensitivity is a construct that may relate to the development and maintenance of depression symptoms and be associated with mattering or anti-mattering (Flett, 2018a; Hammen & Shih, 2014). Those who are higher on rejection sensitivity tend to expect rejection, be highly reactive to the suggestions of rejection, and sometimes respond with aggression to perceived rejection, leading to unstable and conflictual relationships (Beeson et al., 2020; Hammen & Shih, 2014).
Conclusion
Mattering and anti-mattering are related constructs yet share different associations with depression symptoms over time—anti-mattering and depression symptoms shared a positive and bi-directional association over time, whereas mattering and depression symptoms shared a consistent negative association from depression symptoms to mattering and not the reverse. Depression symptoms, mattering, and anti-mattering all showed consistent auto-regressive, concurrent, and cross-lagged associations across four years of development in young adulthood. Addressing interpersonal concerns related to mattering and anti-mattering may be important considerations in the prevention and intervention of depression symptoms.
Supplemental Material
sj-pdf-1-jpa-10.1177_07342829211050519 – Supplemental Material for Depression Symptoms, Mattering, and Anti-mattering: Longitudinal Associations in Young Adulthood
Supplemental Material, sj-pdf-1-jpa-10.1177_07342829211050519 for Depression Symptoms, Mattering, and Anti-mattering: Longitudinal Associations in Young Adulthood by Amanda Krygsman, Ann H. Farrell, Heather Brittain and Tracy Vaillancourt in Journal of Psychoeducational Assessment
Footnotes
Declaration of Conflicting Interests
Funding
Data Availability
ORCID iD
Supplementary Material
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.