Pilot trials are often conducted in advance of definitive trials to assess their feasibility and to inform their design. Although pilot trials typically collect primary endpoint data, preliminary tests of effectiveness have been discouraged given their typically low power. Power could be increased at the cost of a higher type I error rate, but there is little methodological guidance on how to determine the optimal balance between these operating characteristics. We consider a Bayesian decision-theoretic approach to this problem, introducing a utility function and defining an optimal pilot and definitive trial programme as that which maximises expected utility. We base utility on changes in average primary outcome, the cost of sampling, treatment costs, and the decision-maker’s attitude to risk. We apply this approach to re-design OK-Diabetes, a pilot trial of a complex intervention with a continuous primary outcome with known standard deviation. We then examine how optimal programme characteristics vary with the parameters of the utility function. We find that the conventional approach of not testing for effectiveness in pilot trials can be considerably sub-optimal.
Randomised pilot trials are a type of feasibility study which take the same form as a planned definitive randomised clinical trial, but on a smaller scale.1 Internal pilots constitute the initial phase of the definitive trial, with the pilot data being used in the final analysis. In contrast, external pilots are conducted separately to the definitive trial, with a clear gap between the two stages. A key goal of any pilot trial is to guide the decision of whether or not the definitive trial should go ahead, typically with a focus on feasibility issues such as recruitment rates and levels of missing data.2–4
Randomised pilot trials generally collect data measuring the effectiveness of the intervention, and this could be used to inform the decision of progression to the definitive trial. However, several authors have discouraged assessing effectiveness at the pilot stage due to concerns that the small pilot sample size will provide low power and lead to effective interventions being incorrectly discarded.5–8 This criticism rests on two assumptions. Firstly, it assumes that the pilot and definitive trials will share a primary endpoint. Secondly, it assumes that any pilot trial hypothesis test will be conducted with a significance level in the conventional range of 0.01–0.1. For example, consider a two-arm parallel group external pilot trial with a normally distributed primary endpoint and 35 participants per arm, as suggested by Teare et al.9 when the goal of the pilot trial is to estimate the standard deviation of the outcome. This would have a power of 23% (or equivalently, a type II error of ) to detect a standardised effect size of 0.3 when using a one-sided type I error rate of .
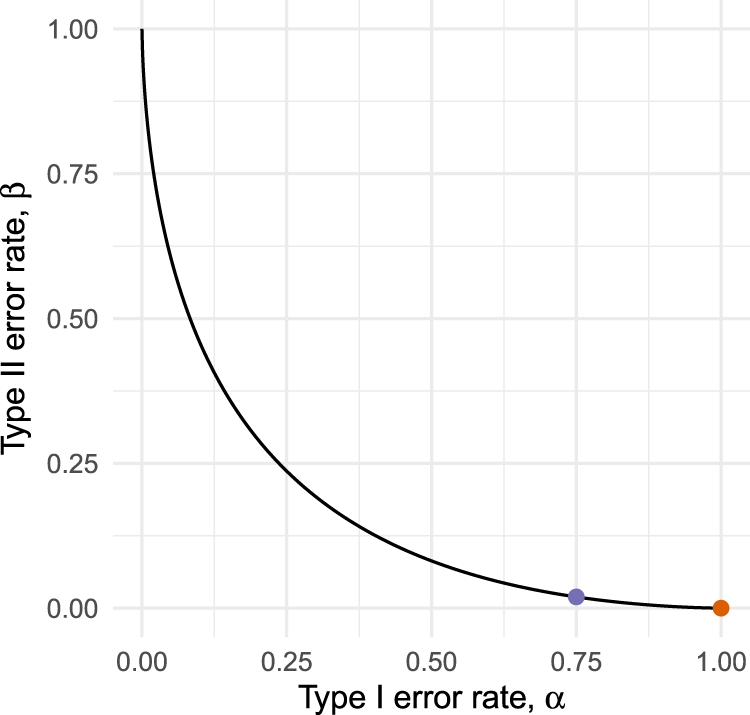
While the assumption of a shared primary endpoint will often hold, there is no obvious reason for type I error rates in pilots to be constrained at conventionally low levels. Indeed, by not testing at all we effectively obtain a procedure with error rates . This testing strategy is only optimal if we have an absolute preference for minimising type II errors over type I errors in the pilot, a preference too extreme to be expected in practice. As illustrated in Figure 1, it will often be possible to reduce considerably (in our example, from 1 to 0.75) at the cost of only a small increase in (from 0 to 0.027). Although relaxing the type I error rate in a pilot has been suggested before,10,11 there is a lack of methodological guidance for determining exactly how much it should be relaxed by, or for choosing an appropriate pilot sample size.
Operating characteristic curves for a hypothetical external pilot trial with fixed sample size testing efficacy.
One possible approach to defining optimal error rates is through Bayesian statistical decision theory. Under this framework we define a suitable utility function which encodes our preferences, and make decisions based on the expected value of this utility with respect to a prior distribution which expresses our uncertainty on the unknown parameters. Although the theory is well established12–14 and has been proposed in previous methodological work around optimal trial design,15 it has been argued that the requirement of specifying a utility function has led to low uptake in practice.16
In this article, we aim to propose a simple and general form for a utility function in two-arm, randomised, parallel group clinical trials, making clear the assumptions which are encoded in it and thus allowing its applicability or otherwise to the problem at hand to be judged. The utility we propose is closely related to several existing proposals in the literature,17 but with some key differences. One particular aspect we have considered is the decision-maker’s attitude to risk, an issue sidestepped by many existing proposals which assume, explicitly or implicitly, that the decision-maker is risk-neutral. We will show that the attitude to risk can have a considerable influence on optimal trial design, and is key to answering the principle motivating question of this paper: in what situations, if any, is it optimal to not test effectiveness in a pilot trial?
The remainder of this article is structured as follows. We define the specific problem under consideration in Section 2, and describe the proposed method in Section 3. In Section 4, we illustrate the application of the method to design an external pilot of a complex intervention. We evaluate the properties of the method over a range of possible scenarios in Section 5, and then outline some extensions in Section 6. Finally, we conclude with a discussion of the strengths and limitations of the proposed approach in Section 7.
Problem
Consider the problem of jointly designing an external pilot trial and subsequent definitive trial. We will denote these, respectively, as stages and of the overall programme. We consider the case where both trials are parallel group studies comparing an intervention to control. We assume that the comparison focuses on superiority in terms of the mean difference of a normally distributed primary endpoint with known standard deviation. For simplicity, we also assume that this standard deviation is common to both arms, although our approach can be applied equally to the heteroskedastic case. Finally, we assume that the endpoint is identically distributed within arms in both the pilot and definitive trial.
We denote the true mean difference by , and consider the case where the primary analysis at each stage will be a z-test of the null hypothesis . The test at stage will compare the sample mean difference between groups, denoted , to a pre-specified critical value, denoted . At the pilot stage, a positive result (i.e. ) will indicate that we should proceed to the definitive trial. At the definitive stage, a positive result (i.e. ) will indicate that the intervention should be recommended for use over the control treatment. The thresholds , along with the per-arm sample sizes at each stage , collectively define the design of the overall programme. The problem we consider in this article is to optimise .
Given some alternative hypothesis , we define the following operating characteristics:
These represent the type I and II error rates of the tests performed at each stage , and provide an alternative summary of the pilot and definitive trial programme. From these we can also derive the overall type I and II error rates of the programme. The probability of obtaining a final statistically significant result under the null hypothesis is , since the events of obtaining significant results in stages and are independent. Similarly, the overall probability of failing to observe a final statistically significant result under the alternative hypothesis is .
Maximising expected utility in trial programmes
We consider a Bayesian view of the frequentist design problem, and, therefore, require a prior distribution for the unknown true mean difference . This prior information will be used only to guide the choice of the frequentist design and analysis parameters, and not in any analysis of the trial data itself. As such, a non- or weakly informative prior is not appropriate; rather, the prior should be a subjective summary of the decision-maker’s knowledge and uncertainty about . For computational tractability, we will assume a normal prior with mean and variance .
We define optimal design variables as those which maximise the expectation, with respect to the prior , of a utility function. We construct the utility function in three steps, following the procedures described by Keeney and Raiffa.13 First, we identify the attributes which we consider will be of interest to the decision maker. We propose these are the total sample size of the trial programme, , the change in mean outcome following the trial programme, . and , an indicator where if the experimental treatment is adopted and otherwise.
We then define a value function over the space of these attributes, which encodes the decision-maker’s preferences under conditions of certainty. We propose that this takes the form of a weighted sum of the three attributes, denoting the weights by and . This gives values of for retaining the control treatment and for adopting the experimental treatment, indicating the latter will be preferred for sufficiently large . These values are then set against the cost of sampling, . The weights can be determined by eliciting two quantities: , a change in mean outcome that would justify increasing the total sample size from 0 to ; and , a change in mean outcome that would justify switching from the current standard treatment to the intervention under study. Having elicited these, we have
We then transform the value function into a utility function by incorporating the decision-maker’s attitude to risk. Drawing on Bayesian decision theory,13 we find that the structure of the value function implies the utility function must be of the form
where the parameter represents the decision maker’s attitude to risk with respect to uncertainty in the overall value of the three attributes. Here, implies risk aversion, risk neutrality, and a risk-seeking attitude. Full details of the derivation of equation (2) and suggestions of how the parameters and can be elicited are given in the appendix.
Expected utility
Denote by an indicator variable where if there is a positive test result at stage , and otherwise. For the problem considered here, . Noting that the attributes , and are completely determined by the fixed programme design , the realisations of and , and the true treatment effect , we re-write utility as . Focusing on the case where (the other cases will follow), we have
The expected utility conditional on is
Since the sample means are conditionally independent and normally distributed as , the conditional probabilities in equation (4) are easily calculated. We are then left with integrating out the unknown treatment effect :
As we are integrating with a normal density weighting function, we can use Gauss-Hermite quadrature (implemented in the ‘fastGHQuad‘ R package18) to evaluate this integral.
Optimisation
Optimal programme designs can be found by solving the optimisation problem
for a given prior distribution for the unknown . To solve this problem, we use the gradient-assisted local optimisation method of Byrd et al.19 as implemented in the R20 function ‘optim’. Full details are provided in the Supplemental Material.
Illustration
OK-Diabetes aimed to assess the feasibility of evaluating supported self-management for adults with learning disabilities and type II diabetes.21 The original target sample size was 30 patients per arm, chosen based on a rule-of-thumb5 and to allow the feasibility objectives of the study to be addressed. The team were asked by the funder to consider assessing the potential efficacy of the intervention to determine whether a confirmatory trial should go ahead. A continuous measure of the percentage difference in participant blood sugar levels (HbA1c) from baseline to six months was chosen as the efficacy outcome. The standard deviation of this outcome was identified to be 1.5%.22 A mean change of 0% was considered to be of no interest, whilst a mean reduction of 0.5% at 6 months was deemed the target difference.
The target sample size was increased to 56 participants per arm, giving power to detect a true mean reduction of 0.5% using a one-sided test with a type I error rate of . Although the error rates for the subsequent definitive trial were not specified, we note that a sample size of 190 participants per arm would lead to power to detect a true mean reduction of 0.5% using a conventional one-sided type I error rate of . In this section, we consider how the proposed method could be used to determine optimal choice of or, equivalently (see Section 2), of the operating characteristics .
Prior and utility
To apply the proposed method, we require a prior distribution on the treatment difference and a utility function . For the former, we use a conjugate normal prior with parameters and . This represents a sceptical prior, being centred at the null hypothesis of no difference and with a variance corresponding to a prior belief that with a probability of 0.20.
For the utility function, we first consider the change in outcome which would be enough to justify the costs of switching from the current standard treatment to the new treatment under study. To determine this value we note that a conventional definitive trial design, with a type I error rate of 0.025, the sample size of 191 participants per arm and a power of 0.9 to detect , would lead to 0.5 power when . This implies an indifference between adopting the new treatment and staying with the current standard if this was the true treatment difference,23 and thus gives a rationale for choosing . For the cost of sampling, we seek to identify a change in treatment effect which would justify an increase in the sample size from 0 to (where the choice of is arbitrary). For the purposes of illustration, we suppose that this leads to , meaning that we consider an increase in sample size of 5000 to be worth paying if we obtained a guaranteed change in treatment effect of 0.5, the target difference in this problem.
Given these judgements and using equation (1), we have the value function
Moving to utility, we set and (arbitrarily) and consider the change of treatment we would like to obtain for certain for it to be judged equivalent to a simple 50/50 gamble between and . We suppose a risk-averse attitude leads to a choice of , corresponding to . Our utility function is then
Optimal design
We consider two variations of the optimal design problem. First, we optimise jointly over the pilot and main trial programme (‘unrestricted’). Then, we optimise only the main trial whilst fixing (‘no pilot test’). In both cases, we note that the original OK-Diabetes sample size of 30 per arm was intended to allow feasibility questions to be addressed, and so we set this as a lower limit of (we will explore the effect of removing this lower limit in Section 5). The algorithm takes around 1 second to converge to a solution. The results are given in Table 1.
Optimal sample size and error rates for the OK-Diabetes external pilots trial () and subsequent definitive trial (), for the general unrestricted case and where we insist on not testing effectiveness in the pilot trial.
Problem
Expected utility
Unrestricted
41
146
0.39
0.110
0.041
0.132
No pilot test
30
110
1.00
0.000
0.036
0.254
In the unrestricted case we find that the optimal programme involves an external pilot sample size of participants per arm, between the initial and revised choices of sample size of 30 and 56 used in OK-Diabetes. The balance of error rates in the pilot is, however, substantially different to those chosen previously. We find that a large stage-1 type I error rate of (one sided) is used, allowing a high power of whilst maintaining a low sample size. Having allowed a large type I error rate in the pilot, the optimal definitive trial uses a lower stage-2 type I error . In isolation this is somewhat higher than the conventional choice of 0.025, but note that when combined with the type I error rate of the pilot trial it leads to an overall type I error rate of . The optimal definitive sample size of 146 per arm then corresponds to a power of 0.868, with an overall power for the programme of .
When we insist on not testing in the external pilot we obtain a lower definitive trial sample size of , with type I error rate and power . The expected utility of this programme is 0.00582 lower than the optimal unrestricted programme. To interpret this, we can translate utilities back to values and then into attribute units. Specifically, note that the utility function implies that an expected utility of can be translated into a value of
A difference in utilities can, therefore, be translated into a difference in values, and this can then be divided by to put it in units of sample size:
For the in our example the two optimal solutions have values of and , giving a difference in value of . Dividing this by leads to an effective difference of 66 participants. That is, we can consider the unrestricted optimal design to be more efficient than the restricted design by an amount equivalent to recruiting and following up 66 participants. Thus, in this case, the conventional policy of not testing effectiveness in pilot trials is considerably inefficient.
To examine the effect of the pilot sample size on the expected utility of the programme, we varied in the range and, optimising over the remaining parameters, calculated the improvement over the ‘no pilot test‘ approach in units of sample size. The lowest improvement in this range was 64 participants, indicating that the benefits derived from the ‘unrestricted‘ approach stem principally from the ability to test effectiveness at the pilot stage, as opposed to any particular choice of pilot sample size.
Sensitivity analysis
The suggested programme design is optimal only for a certain choice of prior and utility parameters, and so it is of interest to assess how robust the design is to deviations from these. To do this we consider a range of alternative parameter values and, for each, determine the optimal programme design. The expected utility of this optimal design can then be compared against that of the proposed design, converted into units of sample size as above in equation (7). We will refer to this difference as the regret. For example, the regret associated with the ‘no pilot test’ approach in Table 1 was 66 participants. We conducted two sensitivity analyses: first, we varied the prior parameters and ; secondly, we varied the utility parameters and . All other parameters were kept at their original values.
Figure 2 plots the regret over a range of prior means and prior standard deviations . We varied the prior mean from 0.5 to 0.5, moving from extremely sceptical to enthusiastic beliefs. We find that over this range there is little to be gained from moving from the proposed design to the locally optimal design, providing the prior standard deviation is equal to or greater than the initial choice of . As we decrease down to 0.48 the penalty of using the proposed design can increase, but the magnitude of these penalties depends on . From these results, we can conclude that the proposed design is quite robust to misspecification of the prior distribution, in the sense that if the choices of are not quite an accurate reflection of our prior beliefs, the design will still have an expected utility close to that of the true optimal design.
Amount of regret when using the proposed OK-Diabetes programme design as the prior mean and prior standard deviation vary. The boundaries of the shaded areas are contours with regret values of 2,…, 10.
Corresponding results for varying utility parameters and are given in Figure 3. We see that the proposed design is quite robust to misspecification of the attitude to risk, and to underestimation of the cost of sampling. However, if the cost of sampling is initially overestimated, the proposed design can become considerably sub-optimal. For example, maintaining but halving the cost of sampling from 0.005 to means the proposed design is worse than the true optimal design by an amount equivalent (through application of equation (7) to 24 participants. This analysis suggests that the choice of , in particular, should be carefully examined to ensure it is a true reflection of the decision-maker’s preferences.
Amount of regret when using the proposed OK-Diabetes programme design as the attitude to risk and cost of sampling vary. The boundaries of the shaded areas are contours with regret values of 5, 10,…,45.
Evaluation
In the OK-Diabetes example, we found that the standard policy of not testing for efficacy in an external pilot trial can be considerably sub-optimal. Here, we consider a range of different utility function parameter values and examine when, if at all, not testing in the pilot trial is optimal. Throughout, we maintain the same sceptical prior with and . We considered the nine scenarios formed by setting the cost of sampling to one of , and the treatment cost parameter to one of . For each of the nine scenarios, we varied the attitude to risk, with , finding optimal programme designs over this range. We did this for two cases: firstly, assuming that a pilot sample size of is required in order to address feasibility questions; and secondly, removing this lower bound.
The case
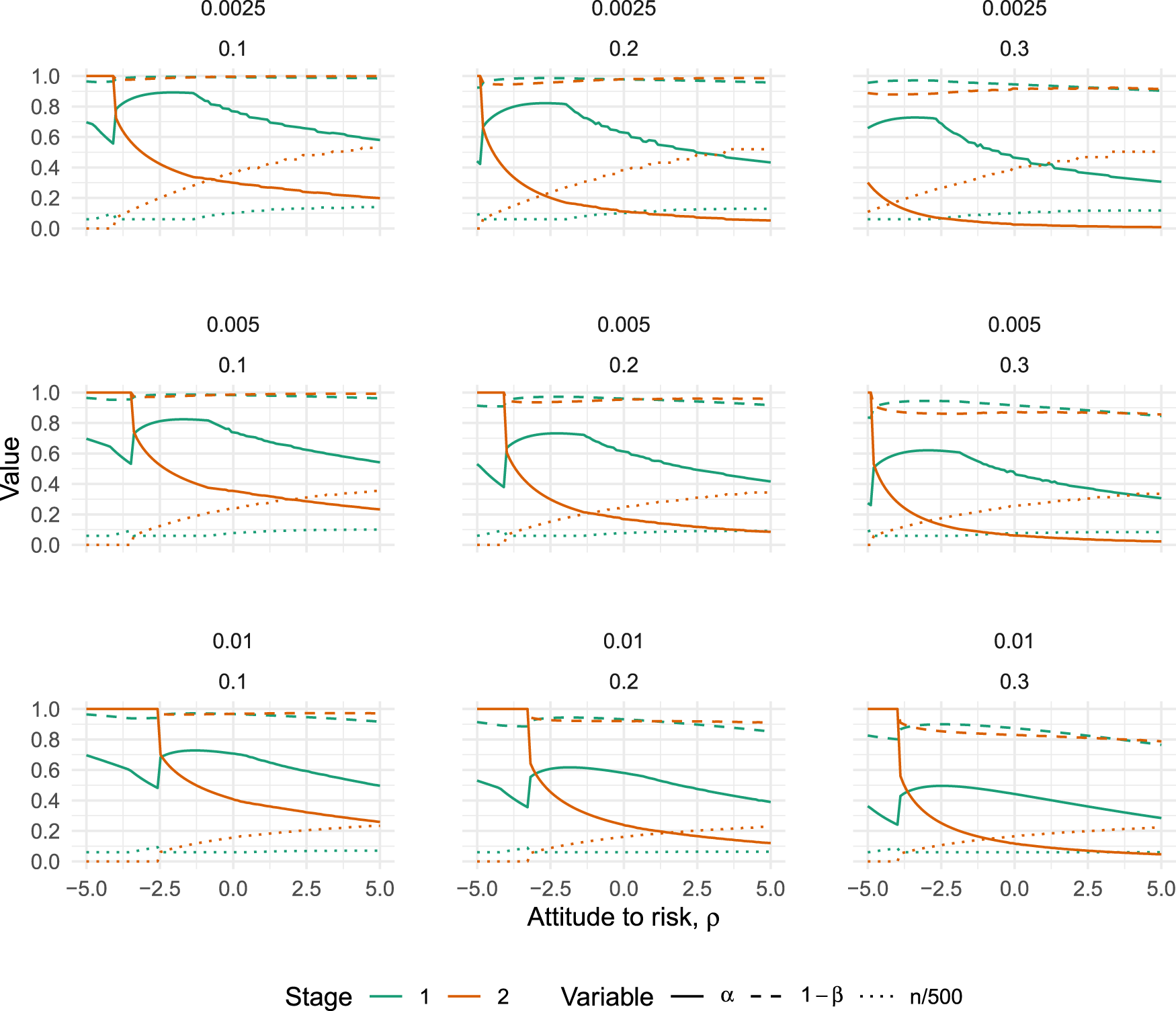
The results are given in Figure 4, which plots how the error rates of both the pilot () and definitive () trials vary with for each of the nine scenarios. It is always optimal to test for effectiveness in the pilot trial in these scenarios, although the type I error rate used can be quite high. The largest we found was , when and (top left panel in Figure 4). The trends in Figure 4 suggest that decreasing and/or could potentially lead to higher , but we failed to find any case where .
Optimal type I error rates (solid lines), type II error rates (dashed lines) and scaled sample size (dotted lines) for varying values of (the attitude to risk, where higher means more risk-averse), when the pilot sample size is constrained to . Plots vary horizontally with treatment costs, , and vertically with sampling costs, .
The broad trends which emerge from Figure 4 are that optimal type I errors tend to decrease as we become more risk-averse, while optimal type II errors stay relatively stable. As the treatment costs increase (moving from left to right in Figure 4), both type I and II errors tend to decrease. And, as the cost of sampling increases (moving from top to bottom in Figure 4), both type I and II errors tend to decrease. In all nine scenarios, we find there is a point where the definitive trial jumps to an optimal design of , meaning the pilot trial is the only trial which will be run. The point where this happens is always for a negative value of . That is, there is a point where a sufficiently risk-seeking attitude will imply the optimal action is to run only one trial.
The case
We now examine the characteristics of optimal programmes with no lower bound on the sample size at the pilot stage. This will be the case when the purpose of the pilot trial is only to assess effectiveness, as opposed to feasibility, and is similar to the problems considered in related work on optimal pilot and phase II trial design.24,25 The results are given in Figure 5, which plots how the error rates of both the pilot () and definitive () trials vary with , for each of the nine scenarios.
Optimal type I error rates (solid lines), type II error rates (dashed lines) and scaled sample size (dotted lines) for varying values of (the attitude to risk, where higher means more risk-averse), when the pilot sample size is unconstrained. Plots vary horizontally with treatment costs, , and vertically with sampling costs, .
The trends of how optimal error rates and sample sizes vary with the utility function parameters are broadly similar to those shown in Figure 4. We see similar inflection points, where now a sufficiently risk-seeking attitude will result in an optimal pilot trial sample size of , leaving only the definitive trial to be conducted. Optimal pilot trial type I error rates are only found to be when . In the scenarios considered here, we again fail to find a situation where it is optimal to run a pilot trial but not test for effectiveness.
Extensions
Internal pilots
Internal pilot trials are distinguished from external pilots by their data being used at the final analysis, with a seamless gap between the pilot and definitive trial stages. Extending our problem to the internal pilot setting, we continue to conduct a first test based on the pilot sample mean difference , but now follow this with a test of the overall sample mean difference , where
We can now apply equation (4) in the internal pilot by defining and . The relevant probabilities can be calculated by noting that the pair , conditional on , follow a bivariate normal distribution. Specifically (see the Appendix),
The probabilities in equation (4) are now with respect to this bivariate normal distribution, and can be calculated using (for example) the R package ‘mvtnorm’.26 Expected utility can then be calculated as before, integrating the conditional expected utility over the normal prior using quadrature.
The optimal internal pilot and definitive trial programme for the OK-Diabetes example is given in Table 2, where we also include the optimal programme for the external pilot case as found in Section 4. We find that the overall type I error rates are approximately equal for both the external and internal pilot cases, and overall type II rates are very similar. The internal pilot programme has a slightly higher expected utility, which we might expect given the fact that all of the data is being utilised in the final analysis.
Optimal sample size and error rates for the OK-Diabetes pilot trial () and subsequent definitive trial(), when the pilot is external and internal.
Problem
Expected utility
External
41
146
0.39
0.110
0.016
0.228
Internal
45
121
0.42
0.084
0.016
0.213
Heterogeneous effects
We have assumed to this point that the treatment effect is the same at both the pilot and main trial stages, but now relax this assumption to allow the effect in pilot trial, , to differ, thus leading to the type of bias highlighted by Sim.8 Specifically, we model the effect vector using the bivariate normal prior distribution
Calculating expected utility proceeds largely as before, but now the probabilities in equation (4) are based on the distribution of the pilot estimate conditional on the true main trial effect :
For example, in the OK-Diabetes example we suppose that the pilot effect has the same marginal mean and standard deviation as the definitive trial effect (i.e. and ). Suppose further that we set the prior correlation between the true pilot and definitive trial effects to be , noting that this is a relatively weak correlation in our context; it implies that our prior belief regarding the main trial effect would have a standard deviation of 0.26 even if the true pilot trial effect was known. Given this joint prior distribution, the optimal programme is given in Table 3. We provide the optimal programme in the case of perfect correlation for comparison.
Optimal sample size and error rates for the OK-Diabetes external pilot trial () and subsequent definitive trial (), for different correlations between pilot and main trial effects .
Expected utility
0.9
30
134
0.69
0.963
0.034
0.818
1.0
41
146
0.39
0.890
0.041
0.868
As we might expect, a less-than-perfect correlation reduces the optimal sample size of the pilot trial and increases its optimal type I error rate. This trend continues as we further reduce , as shown in Figure 6. We find that must be as low as 0.6 for the value of testing effectiveness in the pilot to diminish and the optimal type I error rate approach 1. Repeating this analysis for different values of , the attitude to risk, shows that the point at which the optimal pilot type I error rate approaches 1 increases as decreases and we become more risk-seeking (results not shown here, but see the supplementary material for the required code).
Optimal type I error rates (solid lines), type II error rates (dashed lines) and scaled sample size (dotted lines) for varying values of (the correlation between pilot and main trial effects) in the OK-Diabetes example.
Discussion
We have explored how Bayesian statistical decision theory can be used to define optimal type I and II error rates for trial programmes involving a pilot trial and a subsequent definitive trial. We have introduced a general utility function, outlining the associated assumptions, and demonstrated how its parameter values can be determined. When evaluating the conventional approach to pilot trial analysis we found that a policy of not testing effectiveness was consistently sub-optimal, even when we allowed for heterogeneity between the effects at the pilot and main trial stages. As a result, we recommend that pilot data can and should be used to conduct a preliminary test of effectiveness prior to the definitive trial, when the assumptions around the data generating mechanism, prior distributions and utility function described in this article hold. This would lead to a considerable improvement in the complex intervention evaluation pathway, as more ineffective interventions are identified and screened out at the pilot stage.
A key component of the decision-theoretic approach is the utility function. For simplicity, we did not include any set-up costs relating to the pilot or definitive trial. If these are important, expressing them in units of sample size would allow them to be included in the model easily. In terms of the resulting effect on optimal design characteristics, set-up costs would mean a design with either or becoming more attractive. As such, we might expect to see such designs becoming optimal over a larger range of values for in Figures 4 and 5. We did not attempt to predict the number of patients who will be affected by the results of the definitive trial, or the manner in which they will adopt the intervention following a significant result. Were such a model to be included, the utility function could be re-expressed in terms of individual patient outcomes rather than population parameters, allowing the utilities of the people participating in the trial to be weighted equally against the utilities of those who stand to benefit from the trial results. Such considerations will be particularly important in small population contexts, such as with rare diseases, where the trial population can form a considerable fraction of the overall target population.17 The exponential form of the utility function was derived from an additive value function and an assumption of utility independence, in addition to an assumed mutual preferential independence between the three attributes. Although the appropriateness of these assumptions must be judged in light of the problem at hand, we note that an additive utility function is often assumed in related decision-theoretic work.17,23,27–29 As shown in equation (2), an additive utility entails these assumptions while also assuming risk-neutrality on the part of the decision maker. Our approach can, therefore, recover risk-neutrality as a special case, while also being flexible enough to accommodate risk-averse and risk-seeking attitudes (noting that we would not generally expect to see the latter in the context of our trial design problems). We also emphasise that the utility parameters used in this paper are hypothetical. Future work could examine how the elicitation procedures described in the Appendix work in practice to help understand the feasibility of the proposed approach.
We have considered programmes where a hypothesis test is used in the primary analysis of the pilot and definitive trials. The type I error rates of the suggested optimal programmes have not been restricted, but if this is desired (e.g. the overall type I error rate may need to be < for regulatory purposes) the optimisation problem (6) could be augmented by adding appropriate constraints.30 Further work could explore how a Bayesian analysis of pilot trial data could be used to update prior beliefs and use the revised knowledge to optimise the subsequent definitive trial. At the programme design stage, the pilot trial sample size could then be determined using value of information methods.23 A potential difficulty with such an approach is the computational aspect of such calculations, although techniques for enabling fast calculation of the expected value of sample information may be useful in this context.31,32
We have focused on using pilot trials to test the efficacy of the intervention, but the broad strategy outlined here is quite flexible and could be applied or extended to other settings. For example, it could be used to optimise the design of a single confirmatory trial, helping us find the optimal balance of error rates and sample size.33,34 Programmes of non-inferiority trials could be considered by allowing for negative choices of the parameter , which denotes the amount of treatment difference we would consider equivalent to the costs of adopting the new treatment. The assumption of known variance could easily be relaxed by using t-tests when calculating the probabilities of equation (4) and integrating over a joint prior of effect and outcome variance. When we also want to allow for unequal variance in the two arms of the trial, we can apply the Satterthwaite approximation35 to the degrees of freedom of the t-test, and integrate over a bivariate prior of the two components of the outcome variance. The method for internal pilots described in Section 6.1 could be further extended to the general group sequential setting by allowing for more than one interim analysis and including an option to stop for efficacy as well as for futility. A more involved extension would be to recognise that pilot trials are often used to estimate other parameters relating to the feasibility of the definitive trial, such as recruitment, follow-up and adherence rates.36 These parameters have clear implications for the duration, cost and value of a trial, and as such could be included in the utility function so that learning about them can be offset against the cost of sampling.
The optimisation problem stated in Section 3.2 is not trivial, and we found some variability in performance of different optimisation algorithms. The suggested method was found to be robust, but it would be advisable to check for global convergence when applying to a given problem. This could be done by using other algorithms, such as the genetic optimisation algorithms implemented in the ‘rgenoud’ package,37 to check they agree or by using different starting points. Alternatively, several closely related problems could be solved and the resulting optimal programme characteristics plotted, much as we have done in the sensitivity analyses of Section 4.3. We would expect to see smooth variation, with any erratic behaviour would suggest some convergence issues. Note this is exemplified in Figure 5, where some small blips in the operating characteristic curves can be seen and would suggest a slight failure in convergence at these points. Alternative optimisation approaches may help to address these problems. For example, we could use exhaustive or bisection searches over the sample sizes and , solving the simpler problem of optimising the critical values in each case. As noted in Section 3, the use of a normal prior for the treatment effect aids computational tractability. If an alternative prior is deemed appropriate then the numerical integration in equation (5) would require more general quadrature or Monte Carlo methods, which will increase the time required to solve the optimisation problem.
The majority of our work has assumed the effect sizes in the pilot and definitive trials are equal, which we then relaxed in Section 6 by using a joint prior distribution for the two effects which allows for a correlation of . When applied to our illustrative example we found that testing effectiveness in the pilot remains optimal for , with considerable benefits when . As noted in Section 6.2, this is a relatively weak correlation which implies that the marginal standard deviation for the definitive effect prior reduced from to only when conditioning on the true pilot effect. Empirical studies comparing pilot and definitive trial pairs could potentially provide information to inform these prior beliefs.38 Our results suggest that there is value in trying to minimise the differences between the pilot and definitive trial effects. One way to do that would be to avoid the common practice of making modifications to the intervention following the pilot trial in an attempt to improve it, potentially by instead approaching the question of intervention optimisation through the Multiphase Optimisation Strategy (MOST).39
Supplemental Material
sj-pdf-1-smm-10.1177_09622802251322987 - Supplemental material for Optimising error rates in programmes of pilot and definitive trials using Bayesian statistical decision theory
Supplemental material, sj-pdf-1-smm-10.1177_09622802251322987 for Optimising error rates in programmes of pilot and definitive trials using Bayesian statistical decision theory by Duncan T Wilson, Andrew Hall, Julia M Brown and Rebecca EA Walwyn in Statistical Methods in Medical Research
Footnotes
Acknowledgements
We would like to thank Alex Wright-Hughes and the OK-Diabetes trial team for discussions which helped shape the scope of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research,authorship,and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research,authorship,and/or publication of this article: This work was supported by the Medical Research Council [grant number MR/N015444/1].
ORCID iD
Duncan T Wilson
Supplemental Material
Supplementary material for this article is available online.
References
1.
EldridgeSMLancasterGACampbellMJ, et al.Defining feasibility and pilot studies in preparation for randomised controlled trials: development of a conceptual framework. PLoS ONE2016; 11: e0150205.
2.
CraigPDieppePMacintyreS, et al.Developing and evaluating complex interventions: the new medical research council guidance. BMJ: British Med J2008; 337: a1655.
3.
ThabaneLMaJChuR, et al.A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol2010; 10: 1.
4.
EldridgeSMChanCLCampbellMJ, et al.CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ2016; 335: i5239.
5.
LancasterGADoddSWilliamsonPR. Design and analysis of pilot studies: recommendations for good practice. J Eval Clin Pract2004; 10: 307–312.
6.
ArainMCampbellMCooperC, et al.What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med Res Methodol2010; 10: 67.
7.
WestlundEStuartEA. The nonuse, misuse, and proper use of pilot studies in experimental evaluation research. Am J Eval2016; 38: 246–261.
8.
SimJ. Should treatment effects be estimated in pilot and feasibility studies? Pilot Feasib Stud2019; 5: 107.
9.
TeareMDimairoMShephardN, et al.Sample size requirements to estimate key design parameters from external pilot randomised controlled trials: a simulation study. Trials2014; 15: 264.
10.
CocksKTorgersonDJ. Sample size calculations for pilot randomized trials: a confidence interval approach. J Clin Epidemiol2013; 66: 197–201.
11.
LeeEWhiteheadAJacquesR, et al.The statistical interpretation of pilot trials: should significance thresholds be reconsidered?BMC Med Res Methodol2014; 14: 41.
KeeneyRLRaiffaH. Decisions with multiple objectives: preferences and value tradeoffs. Cambridge: John Wiley & Sons, 1976.
14.
LindleyDV. The choice of sample size. J R Stat Soc: Ser D (The Stat)1997; 46: 129–138.
15.
HeeSWHamborgTDayS, et al.Decision-theoretic designs for small trials and pilot studies: a review. Stat Methods Med Res2016; 25: 1022–1038.
16.
JosephLWolfsonDB. Interval-based versus decision theoretic criteria for the choice of sample size. J R Stat Soc: Ser D (The Stat)1997; 46: 145–149.
17.
PearceMHeeSWMadanJ, et al.Value of information methods to design a clinical trial in a small population to optimise a health economic utility function. BMC Med Res Methodol2018; 18: 20.
ByrdRHLuPNocedalJ, et al.A limited memory algorithm for bound constrained optimization. SIAM J Sci Comput1995; 16: 1190–1208.
20.
R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria, 2019. https://www.R-project.org/.
21.
WalwynREARussellAMBryantLD, et al.Supported self-management for adults with type 2 diabetes and a learning disability (OK-Diabetes): study protocol for a randomised controlled feasibility trial. Trials2015; 16: 342.
22.
HouseABryantLRussellAM, et al.Managing with learning disability and diabetes: OK-diabetes – a case-finding study and feasibility randomised controlled trial. Health Technol Assess (Rockv)2018; 22: 1–328.
23.
WillanARPintoEM. The value of information and optimal clinical trial design. Stat Med2005; 24: 1791–1806.
24.
StallardN. Optimal sample sizes for phase II clinical trials and pilot studies. Stat Med2012; 31: 1031–1042.
25.
KirchnerMKieserMG’otteH, et al.Utility-based optimization of phase II/III programs. Statist Med2015; 35: 305–316.
GittinsJPezeshkH. A behavioral bayes method for determining the size of a clinical trial. Drug Inf J2000; 34: 355–363.
28.
KikuchiTGittinsJ. A behavioral bayes method to determine the sample size of a clinical trial considering efficacy and safety. Statist Med2009; 28: 2293–2306.
29.
HeeSWStallardN. Designing a series of decision-theoretic phase II trials in a small population. Stat Med2012; 31: 4337–4351.
30.
VentzSTrippaL. Bayesian designs and the control of frequentist characteristics: a practical solution. Biometrics2015; 71: 218–226.
31.
StrongMOakleyJEBrennanA, et al.Estimating the expected value of sample information using the probabilistic sensitivity analysis sample: a fast, nonparametric regression-based method. Med Decis Making2015; 35: 570–583.
32.
HeathAManolopoulouIBaioG. Estimating the expected value of sample information across different sample sizes using moment matching and nonlinear regression. Med Decis Making2019; 39: 346–358.
33.
GrieveAP. How to test hypotheses if you must. Pharm Stat2015; 14: 139–150.
34.
WalleyRJGrieveAP. Optimising the trade-off between type I and II error rates in the Bayesian context. Pharm Stat2021; 20: 710–720.
35.
SatterthwaiteFE. An approximate distribution of estimates of variance components. Biomet Bull1946; 2: 110–114.
36.
AveryKNLWilliamsonPRGambleC, et al.Informing efficient randomised controlled trials: exploration of challenges in developing progression criteria for internal pilot studies. BMJ Open2017; 7: e013537.
37.
MebaneW JrSekhonJS. Genetic optimization using derivatives: the rgenoud package for R. J Stat Softw2011; 42: 1–26.
38.
YingXRobinsonKAEhrhardtS. Re-evaluating the role of pilot trials in informing effect and sample size estimates for full-scale trials: a meta-epidemiological study. BMJ Evid-Based Med2023; 28: 383–391.
39.
CollinsLMMurphySANairVN, et al.A strategy for optimizing and evaluating behavioral interventions. Ann Behav Med2005; 30: 65–73.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.