
Abstract
Keywords
Abbreviations
BSI - Bloodstream Infection, CDC - Centers for Disease Control and Prevention, CI - Confidence Interval, CLABSIs - Central Line-Associated Bloodstream Infections, CRBSI - Catheter-Related Bloodstream Infection, CRI - Catheter-Related Infection, CVAD - Central Venous Access Device, CVC - Central Venous Catheter, CVL - Central Venous Line, EPIC - European Prevalence of Infection in Intensive Care, ETB - Ethiopian Birr, HAI - Hospital Acquired Infection, HCW - Health Care Workers, ICU - Intensive Care Unit, INICC - International Nosocomial Infection Control Consortium, NGO - Non-Governmental Organisation, UK - United Kingdom, US - United States, USA - United States of America, WHO - World Health Organisation.
Introduction
Healthcare-associated infections (HAIs) are a major public health concern worldwide, being a leading cause of illness and death among hospitalised patients.[1] Central line-associated bloodstream infections (CLABSIs), primarily stemming from the use of central venous catheters (CVCs), represent a major complication in critical care and emergency medicine environments.[2] CVCs allow healthcare professionals to measure central venous pressure, which in turn offers an indication of fluid status and right ventricular function.[3] When major surgery carries a significant risk of blood loss or if the patient has a serious heart condition, central venous pressure monitoring is recommended. Furthermore, patients needing long-term treatment with total parenteral nutrition, chemotherapy or antibiotics, and medications that can harm smaller veins may benefit from having a CVC placed.[4]
Catheter-related bloodstream infection (CRBSI) is a type of bacteraemia that originates from an intravenous catheter. This infection typically arises due to the introduction of microorganisms from the patient’s skin or the hands of healthcare personnel involved in catheter insertion or maintenance. It has been noted that approximately 60% of CRBSI results from this form of contamination. Infections can have serious consequences for patients, potentially progressing from local symptoms to widespread systemic illness, including conditions like endocarditis, and in severe cases, can be fatal. The length of inpatient stay increases by approximately one week in intensive care and by two to three weeks in the hospital as a result of CRBSI. This has implications for the patient and his or her family, as well as the service provider.[1,5]
CLABSIs are characterised as bloodstream infections that develop at least 48 hours after a central catheter is placed and are not linked to any other source of infection. In intensive care settings, a number of factors have been linked to an increased risk of CLABSIs. These include how long the catheter stays in, microbes found at the insertion site and on the catheter itself, and not properly maintaining the CVC after it’s placed.[2]
CLABSIs contribute to extended hospitalisations, escalating healthcare expenditures, and heightened mortality rates. An estimated 250,000 bloodstream infections occur annually, and most are related to the presence of intravascular devices. Central line-associated bloodstream infections are common HAIs with a reported mortality of 12%-25%.[3]
Prevention of CLABSI involves meticulous hand hygiene prior to CVC care, utilising either an alcohol-based hand sanitiser or an antibacterial soap with thorough water rinsing.[6] According to the WHO, up to 30% of intensive care unit (ICU) patients develop HAIs, primarily bloodstream infections linked to catheter presence in veins.[5]
Several international organisations have published clinical practice guidelines for preventing CLABSIs, intended for healthcare workers (HCWs) who insert and manage CVCs. ICU nurses have the most direct and continuous role in high-risk CVC procedures. Therefore, they are well-positioned to implement the recommendations and have a unique opportunity to contribute to the primary prevention of these infections via evidence-based best practices.[3]
The International Nosocomial Infection Control Consortium (INICC) reports a pooled CLABSI incidence of 4.9 infections per 1,000 central-line days across its ICUs (Africa, Asia, Europe, and Latin America), nearly five times higher than US rates.[2] The Centres for Disease Control and Prevention (CDC) estimated that HAIs affect 2 million patients annually, causing nearly 100,000 deaths.
These infections increase mortality, prolong hospital stays, and raise healthcare costs for patients, insurers, and facilities.[7] In 2020, U.S. ICUs had a CLABSI rate of 0.87 per 1,000 central line days.[8]
United States (US) hospitals experience nearly 250,000 CLABSIs annually, resulting in 28,000 deaths and a $2.3 billion burden on the healthcare system.[9] The CDC considers CLABSIs the deadliest HAI, with a mortality rate of 25%, making it the most devastating HAI consequence.[7] Patients with CLABSI have a 2.75 times higher risk for hospital death as compared to those without CLABSI.[10]
CLABSIs cost an estimated $49,201 per case.[7] In the US, CLABSIs have an 18% mortality rate, cost about $18,432, and result in an average hospital stay of 12 days.[11] CLABSIs pose a serious risk to neonatal health.[9] Additionally, CLABSIs are the second leading cause of death among patients with renal issues.[12] Moreover, CLABSI is the most important complication in critical care and cancer settings.[1] HCWs may struggle to consistently follow CLABSI prevention guidelines due to various internal and external barriers.[13] Assessing HCW contributions to CLABSI prevention is crucial, as success relies on monitoring insertion processes and routine CVC maintenance.[14,15]
To minimise CLABSI incidence, the CDC recommends guidelines focusing on education and training, maximal sterile barrier precautions, the use of >0.5% chlorhexidine with alcohol for skin antisepsis, avoiding routine catheter replacement, and implementing bundled strategies.[4] Studies indicate that inadequate knowledge and skills among HCWs are key barriers to preventing CLABSIs.[4] Despite inconsistencies, sex, length of time in ICU nursing, educational level, nursing level, hospital grade, and incidence of CLABSI are the factors associated with HCWs’ knowledge and practice in preventing CLABSI.[10] In our country, there is a lack of evidence on HCW’s knowledge, practice, and factors for preventing CLABSIs, making it essential to evaluate these factors in cardiac units. Therefore, this study is intended to assess health workers’ knowledge, practice, and associated factors towards CLABSIs in cardiac units of Addis Ababa, Ethiopia, in 2024.
Methods and Materials
Study Area and Period
This study was conducted in seven cardiac centres in Addis Ababa from January 10 to February 10, 2024. Addis Ababa is composed of 11 sub-cities and 118 woredas and has an estimated total population of 3,854,863, including 2,004,529 females and 1,850,334 males.[16] Cardiac centres in Addis Ababa consist of: Cardiac Centre-Ethiopia, St. Peter’s Specialised Hospital Cardiac Centre, Tazma Medical & Surgical Specialised Centre, Tikur Anbessa Hospital Cardiac Centre, Elouzeir Cardiac Centre, Gesund Cardiac Centre and Addis Cardiac Hospital. Cardiac centres in Addis Ababa give cardiac outpatient services, including echocardiography, electrocardiogram, cardiac ward, cardiac catheterisation, cardiac operation theatre, and cardiac ICU services. The total number of HCWs in the seven cardiac centres is 588.
Study Design and Population
We employed a hospital-based cross-sectional study design. The source population comprised all HCWs working in the seven cardiac centres of Addis Ababa, Ethiopia. The study population included all HCWs working in the cardiac unit of the selected cardiac centres.
Inclusion and Exclusion Criteria
All HCWs who worked six months and above in the cardiac unit involving central line catheterisation practice and were available during the data collection period were included in the study. Those who were seriously ill during the data collection period and HCWs who did not have direct patient care responsibilities involving CVL were excluded from the study.
Sample Size Determination and Sampling Procedures
The sample size was calculated by using the single population proportion formula by taking the proportion of knowledge and practice towards prevention of CLABSIs (P) at 50%. Since there was no study conducted in our country regarding this title, the margin of error (d) was 0.05, with a 95% confidence interval and a non-response rate of 5%. The sample size became 403. Where n is the minimum sample size required for the study, d is margin of error, p is proportion of knowledge and practice towards prevention of CLABSIs, and Zα/2 is the value of the standard normal distribution.
Sampling Techniques and Procedures
All seven cardiac centres in Addis Ababa (Cardiac Centre-Ethiopia, St. Peter’s Specialised Hospital Cardiac Centre, Tazma Medical & Surgical Specialised Centre, Tikur Anbessa Hospital Cardiac Enter, Elouzeir Cardiac Centre, Gesund Cardiac Centre, and Addis Cardiac Hospital) were included in the study. Data reviewed from each cardiac centre showed that the number of HCWs in each centre was: Cardiac Centre-Ethiopia = 50, St. Peter’s Specialised Hospital Cardiac Centre = 111, Tikur Anbessa Hospital Cardiac Enter = 121, Tazma Medical & Surgical Specialised Centre = 101, Addis Cardiac Hospital = 57, Elouzeir Cardiac Centre = 75, and Gesund Cardiac Centre = 73.
The total sample size was then proportionally allocated to the selected using Baurley’s method of proportionate allocation technique[17] based on the number of HCWs in each cardiac centre. Baurley’s method of proportional allocation follows the formula
Schematic Presentation of Sampling Procedure for the Study of Assessment of Knowledge and Practice and Factors Associated Towards Prevention of CLLABSIs

Measurement
Study Variables
Dependent Variables
Knowledge towards prevention of CLABSIs.
Practice towards prevention of CLABSIs.
Independent Variables
Socio-demographic Professional Characteristics: age, gender, marital status, education level, and work experience.
Profession and job-targeted factors: infection prevention training, participating in peer education programmes, and presence of guidelines.
Workplace-related factors: infection prevention equipment, water supply.
Data Collection Tools and Procedures
Data was collected using a pretested, self-administered questionnaire. The questionnaire contains open-ended and closed-ended questions designed to collect data on socio-demographic factors, knowledge and practice towards the prevention of CLABSI, the presence of guidelines, profession- and job-targeted factors, and workplace-related factors. After reviewing literature, the questionnaire to assess knowledge and practice was modified from CDC recommendations,[3,9,14,18,19] and questions related to independent variables were prepared after reviewing different literature. Data was collected by four BSc nurses for one month with close supervision of the assigned supervisors. The data collectors and supervisors were given three days of training on confidentiality and the objective of the study. During data collection, the completeness of each questionnaire was checked on a daily basis. The instrument tried to cover all relevant aspects of the construct being measured. The study used a standard CDC checklist for the prevention of central line-associated bloodstream infections. In addition, pilot testing of the instrument was conducted before the actual study.
Operational Definitions
CLABSI is a bloodstream infection that happens because of pathogens entering the bloodstream through a central line in a patient who had a central line at the time of infection or within 48 hours before the development of the infection.[20]
Healthcare Workers: are individuals who work in a healthcare setting and provide direct or indirect patient care, or who handle patient data or materials.
Knowledge towards prevention of CLABSIs was assessed using knowledge questions from the CDC Checklist for Prevention of Central Line-Associated Blood Stream Infections. The questions were modified. Eight questions were used to assess the knowledge towards the prevention of CLABSIs with three response options. Among the questions, one question is reverse coded, which says, ‘It is recommended to use topical antibiotic ointment on the catheter insertion site.’ Correct responses were recorded as 1, and incorrect responses were recorded as 0. The responses were summed up, and a mean score was calculated.[1,19]
Good knowledge: Participants who scored above or equal to the mean score of the CDC Checklist for Prevention of Central Line Associated Blood Stream Infections.
Poor knowledge: Participants who scored below the mean score of the CDC Checklist for Prevention of Central Line Associated Blood Stream Infections.
Practice towards prevention of CLABSIs was assessed using practice questions from the CDC Checklist for Prevention of Central Line-Associated Blood Stream Infections. A correct response was recorded as 1, and incorrect responses were recorded as 0. The responses were summed up and a mean score was calculated.[19]
Good practice: participants who scored above or equal to the mean score of the CDC Checklist for practice towards Prevention of Central Line Associated Blood Stream Infections.
Poor practice: Participants who scored below the mean score of the CDC Checklist for practice towards Prevention of Central Line Associated Blood Stream Infections.
Data Quality Control
Before data collection: Before data collection, the questionnaire was pretested on 5% of the total sample at the International Cardiac and Medical Centre (ICMC) Hospital’s HCWs to determine the response rate, clarity, sequence, and consistency of the questionnaire. The sequence of the tool was adjusted based on the results of the pretest. An inter-rater reliability test was performed for nurses who were collecting the data using pilot testing, training, and standardisation. The data collectors were given two days of training on the study’s objective, relevance, and confidentiality of information, respondents’ rights, informed consent, and interview techniques. In addition, a practical interview demonstration was held in a classroom.
During data collection, the data collection was strictly supervised throughout the data collection period by the assigned supervisors and the principal investigator. The questionnaires were checked for completeness and consistency at the site of the data collection by the principal investigator.
During data entry and analysis, the collected data were coded and entered into EpiData software version 3.1. The quality of the data was controlled through skipping patterns that must enter and reduce transportation errors in EpiData. Finally, cleaning and analysis were performed using SPSS version 25.
Data Processing and Analysis
Data was coded and entered using EpiData version 3.1 and exported to SPSS version 25 for further analysis. Data were cleaned by performing the frequency of each variable to check the accuracy, inconsistency, and missed value of the data. Before analysis of the data, the recoding of variables was employed to make it easy for analysis. Descriptive statistics including frequencies, mean, median, and interquartile range were computed. Additionally, for continuous variables, normality was checked using histograms, boxes, and whisker plots.
Bivariate logistic regression analysis was employed to determine the association between each independent variable and knowledge and practice among HCWs on the prevention of CLABSIs. Before performing bivariate logistic regression analysis, assumptions for logistic regression were checked. Those variables with
Finally, multivariable logistic regression analysis was performed to identify the independent predictors of knowledge and practice of HCWs towards the prevention of CLABSIs. Those variables with a
Results
Socio-demographic Characteristics
From the total of 403 HCWs recruited, 400 completed the questionnaire adequately, making the response rate of 99.25%. Two hundred twenty-three (55.8%) of the respondents were male. The mean age of the respondents was 34.27 ± 8.819 SD years. From the participants, 141 (35.3%) of them were diploma nurses in profession, and 211 (52.8%) were married. Approximately half (51%) of the respondents had five years and below work experience. The majority (25%) of the respondents were ordinary nurses [Table 1].
Socio-demographic Characteristics of HCWs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)

Knowledge of the Participants’ Towards Prevention of CLABSIs
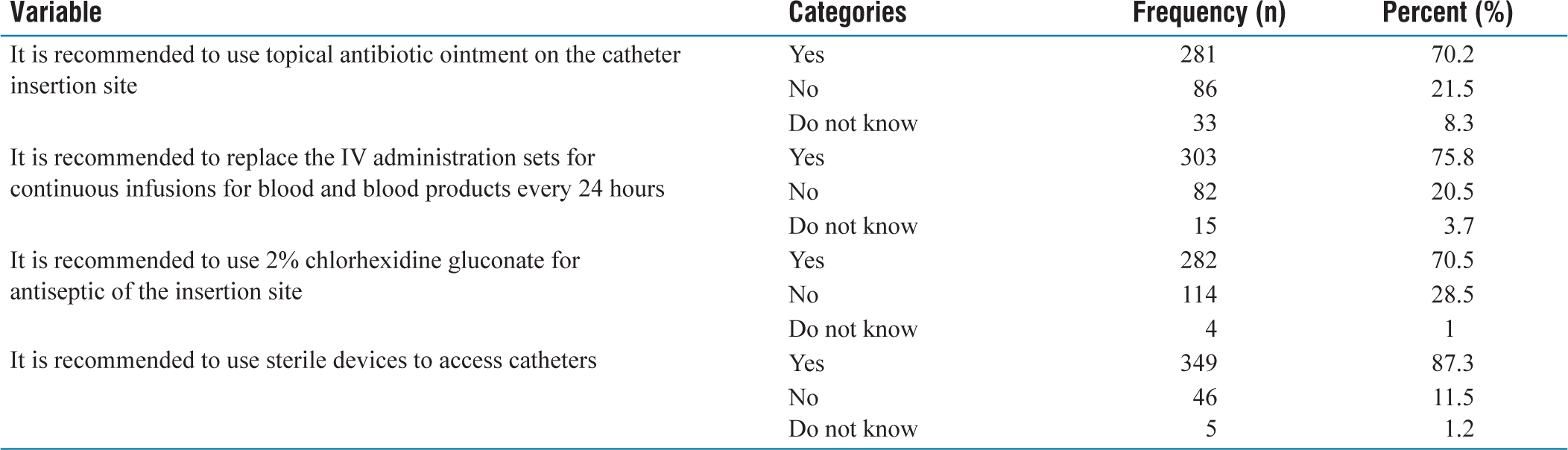
Of the participants, 343 (85.8%) had good knowledge towards prevention of CLABSIs [Figure 2]. Three hundred fifty-seven (89.3%) of them answered the recommendations correctly concerning flushing the lumen with saline after the administration of medication or fluid. In addition, 373 (93.3%) answered the recommendations correctly concerning using sterile gauze or a sterile transparent semipermeable dressing to cover the catheter site. Three hundred twenty-three (80.7%) of the participants answered the recommendations to comply with hand hygiene requirements correctly. Three hundred twelve (78%) of them answered the recommendations correctly to replace catheter site dressings every two days for gauze dressings, every seven days for sterile semipermeable dressings, or if the dressing becomes visibly soiled or loosened. Two hundred eighty-one (70.3%) of the participants answered incorrectly regarding applying topical antibiotic ointment on the catheter insertion site. Three hundred three (75.8%) of them answered the recommendations to replace the IV administration sets for continuous infusions of blood and blood products every 24 hours correctly. Finally, 282 (70.5%) of them answered the recommendations correctly using 2% chlorhexidine gluconate for antiseptic of the insertion site
Overall Knowledge Status of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)

Knowledge of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)

Practice of the Participants Towards Prevention of CLABSIs
From the participants, 294 (73.5%) of them had good practice towards prevention of central line-associated bloodstream infections. From the participants, 344 (86%) of them used to change the dressing on the CVC insertion site. Two hundred 10 (52.5%) of them used to clean the CVC site before disinfection. The majority of the participants (66.5%) used to allow the antiseptic to dry before proceeding. The majority (78.3%) of them used to perform the disinfection of the CVC access port before administering therapy. Finally, two hundred sixty-six (66.3%) of them were used to replace the intravenous (IV) administration sets
Practice Status of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)


Sources About Prevention of CLABSIs
HCWs indicated workshops and courses (31%) as their main source of information about the prevention of CLABSIs, followed by colleagues (22%), and the internet (12.7%). The vast majority (86.3%) reported that they would like to learn more
Source of Information of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)

Profession and Job-targeted Factors Towards the Prevention of CLABSIs
From the participants, 332 (83%) of them liked their profession. Three hundred forty-four (86%) of them were not satisfied with their salary. Two hundred twenty-four (56%) of them have taken training regarding infection prevention on CLABSIs. Two hundred twenty-one (55.3%) of them have never been recognised for their best performance
Profession and Job-targeted Factors of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)

Work-place-related Variables
Of the participants, 352 (88%) thought that their workplace was suitable for them, and 361 (90.3%) of them thought that their work unit was well designed for ventilation. Three hundred eighty (95%) of them knew that the garbage pit was always available at the work unit
Workplace-related Factors of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)

Factors Associated With HCWs Knowledge Towards Prevention of CLABSIs
Bivariate analysis was conducted to identify factors associated with HCWs knowledge towards CLABSIs. Sex of respondents, age category, educational level, work experience, participation in peer education programmes, and training regarding infection prevention on CLABSIs were found to have
The odds of having good knowledge towards prevention of CLABSIs by HCWs in this study were two times higher among HCWs with having bachelor’s degree or higher as compared to those with a diploma educational level (AOR: 2.086, 95% CI: 1.127, 3.860),
Bivariate and Multivariate Analysis Knowledge of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)

Factors Associated With HCWs Practice Towards Prevention of CLABSIs
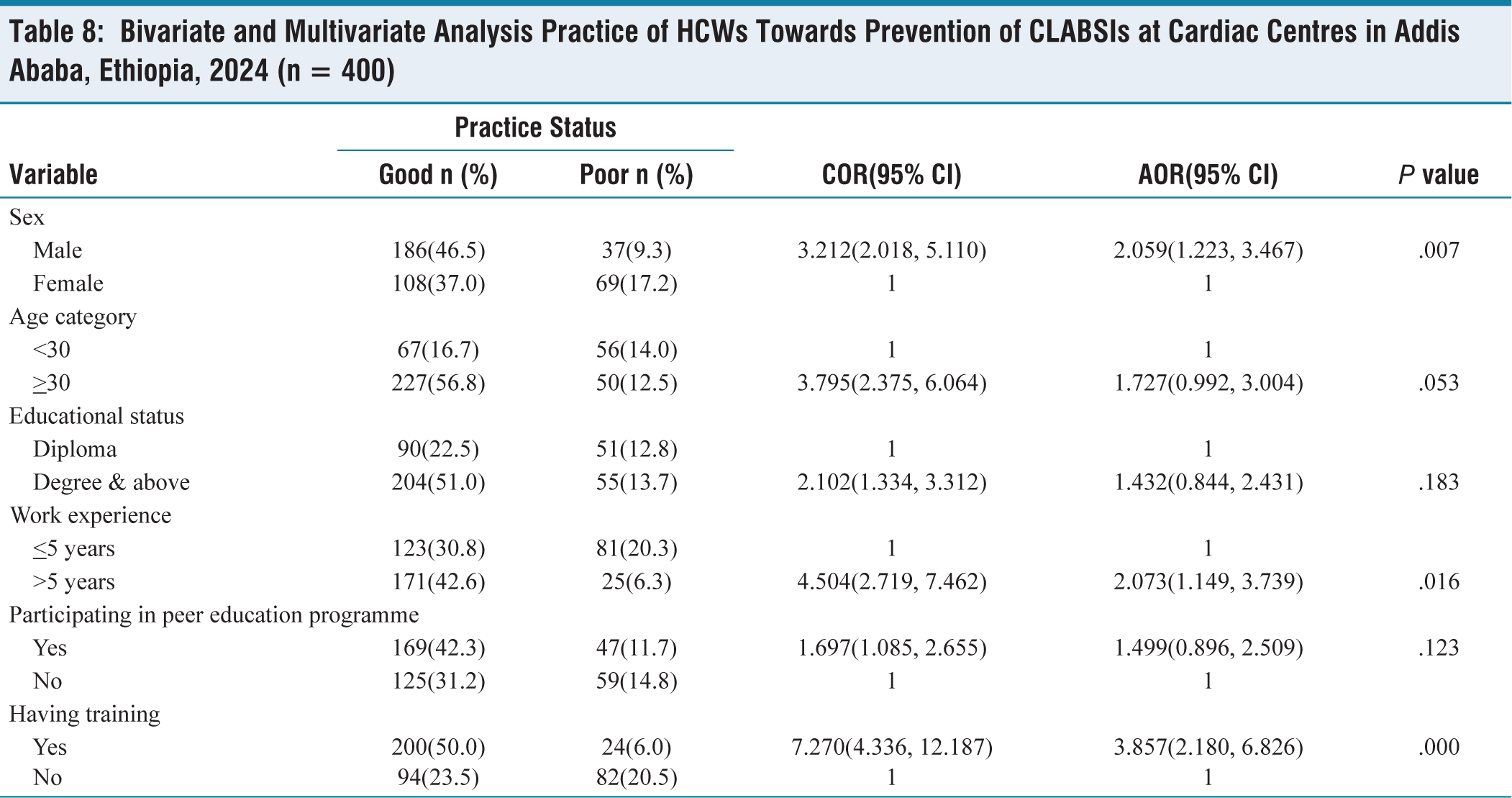
Bivariate analysis was conducted to identify factors associated with HCWs practice of CLABSIs. Sex of respondents, age category, educational level, work experience, participation in peer education programmes, and training regarding infection prevention on CLABSIs were found to have
The odds of having good practice of
Bivariate and Multivariate Analysis Practice of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)
Discussion
HCWs Knowledge Towards Prevention of CLABSIs
The study showed that 85.8% (95% CI: 82.38%, 89.22%) of the study participants had good knowledge towards prevention of CLABSIs. This was in line with a study conducted in Debre Markos (84.7%)[21] and Dessie (86.4%).[22] This level of knowledge was lower than in a study conducted in Malaysia (94.2%)[23] and Gonder (90%).[24] The possible explanation for this difference might be due to differences in sampling procedure, sample size, study period, and study population.
This level of knowledge was higher than a study conducted in Saudi Arabia (71%),[25] Italy (43%-72.9%),[26] Nigeria (64.4%),[27] Alexandria (20.6%),[28] Axum Saint Mary Hospital (52.5%),[29] Northeast Ethiopia (70.8%),[30] Northwest Ethiopia (40.3%),[31] Southern Ethiopia (45.5%),[32] and Arsi (53.7%).[33] This might be due to the difference in study period, sample size, and socio-demographic characteristics with other European and African countries.
Educational level was significantly associated with HCWs’ knowledge towards prevention of CLABSIs. Those HCWs who have a bachelor’s degree or higher had two times higher odds of good knowledge as compared to those having a diploma educational level. This was supported by a study conducted in Debre Markos,[21] and Southern Ethiopia.[32] This might be due to the fact that being at a higher education level enables the HCWs to improve their capability of reading and understanding.
Participating in peer education programmes is important in increasing knowledge of HCWs’ towards prevention of CLABSIs. In this study, the odds of good knowledge towards the prevention of CLABSIs were two times higher among HCWs who participated in peer education programmes as compared to those who did not. This could be because experience sharing is vital in improving the knowledge of HCWs.
On-the-job training is important to refresh HCWs motivation to work and close the knowledge gap. Training on CLABSIs prevention was significantly associated with knowledge HCWs had towards the prevention of CLABSIs. Those HCWs who got training on prevention of CLABSIs had three times higher odds of good knowledge than those who did not have training. This was supported by a study conducted at Axum Saint Mary Hospital,[29] Southern Ethiopia,[32] Northeast Ethiopia,[30] and Northwest Ethiopia.[31] This might be due to the fact that training improves knowledge and gives new insight to the participants.
HCWs Practice Towards Prevention of CLABSIs
This study revealed that the magnitude of good practice towards prevention of CLABSIs was 73.5% (95% CI: 69.17%, 77.83%)
Overall Practice Status of HCWs Towards Prevention of CLABSIs at Cardiac Centres in Addis Ababa, Ethiopia, 2024 (n = 400)

The level of good practice in this study is greater than studies done in: Saudi Arabia (65%),[25] Nigeria (27.5%),[27] Alexandria (44%),[28] Axum Saint Mary Hospital (48.6%),[29] Northeast Ethiopia (55%),[30] Debre Markos (57.3%),[21] Southern Ethiopia (64.8%),[32] Gonder (36%),[24] Dessie (23%),[22] Arsi (36.3%)[33] and Northwest Ethiopia (48.75%).[31] The possible reason for this discrepancy could be due to sample size differences in Nigeria, Alexandria, Axum, Gonder and Dessie where these studies conducted with smaller sample sizes than this study. Additionally, study period differences could have contributed to the discrepancy.
In this study, the odds of good practice towards prevention of CLABSIs among males were two times higher as compared to females. This finding is supported by studies done in Ghana.[34] The odds of having good practice about prevention of CLABSIs by HCWs in the study were two times higher among HCWs who had more than five years of work experience as compared to those who had five years and below work experience. This finding is supported by studies done in Axum Saint Mary Hospital[29] and Debre Markos.[21] The possible reason could be that as the work experience year increases, HCWs will improve their practice through time. Additionally, HCWs with more prolonged exposure to patient care have a greater chance to learn how to prevent CLABSIs from their own mistakes and their colleague’s experience.
Finally, in this study, HCWs who had taken training on CLABSIs prevention were four times more likely to have good practice towards the prevention of CLABSIs as compared to their counterparts. This finding is supported with studies done in Northeast Ethiopia[30] and Arsi.[33] The possible reason could be the fact that training on current guidelines could upgrade the knowledge and skill of HCWs in that they would easily understand basic principles standards of practice and implement them consistently. In addition, up-to-date knowledge and skill regarding infection prevention could also increase the confidence of HCWs in complying with recommended guidelines and the available supply.
Limitations of the Study
This study has several limitations. Reliance on questionnaires for assessing knowledge and practice can be susceptible to recall bias and social desirability bias. HCWs might overestimate their knowledge or underreport practices they perceive as negative. Since there was limited observation of practice, the questionnaire might not capture the actual practice of HCWs in real-world clinical settings. Direct observation of practices would provide a more accurate assessment but can be challenging to implement. The study might not comprehensively assess all relevant contextual factors that influence HCWs’ behaviour, such as workload, staffing levels, and organisational culture. As the study used a cross-sectional study design, it is difficult to relate the temporal relationship. It also has a short duration of study.
Conclusion
In this study, more than three-fourths of HCWs in cardiac centres in Addis Ababa had good knowledge towards the prevention of CLABSIs. Furthermore, approximately three-fourths of HCWs in cardiac centres in Addis Ababa had good practice towards the prevention of CLABSIs. Educational level, participation in peer education programmes, and training on CLABSI prevention were factors associated with knowledge towards the prevention of CLABSIs. Additionally, sex, work experience, and training on CLABSIs prevention were factors associated with practice towards prevention of training on CLABSIs prevention.
Cardiac centres should give mandatory and regularly updated training on CLABSIs prevention for all HCWs involved in patient care, particularly those working in high-risk units (e.g., ICU, surgery). They should also integrate CLABSIs prevention training and peer education into existing professional development programmes for new hires and continuing education initiatives. In addition, they should utilise multiple training modalities (e.g., online modules, workshops, simulations, case studies) to cater to different learning styles and ensure knowledge retention.
Furthermore, implementing peer education programmes through training peer educators and establishing a peer education network is recommended. Finally, implementing structured mentorship programmes that pair experienced HCWs with newer colleagues and offering opportunities for skill development and training that are tailored to different levels of work experience are recommended.
Healthcare professionals should actively participate in CLABSIs prevention training and utilise the knowledge gained in their daily practice. Additionally, they should embrace continuous learning and advocate for the implementation of best practices and protocols related to CLABSIs prevention within their teams and departments. Furthermore, they should foster collaboration and communication between different HCWs involved in patient care to ensure consistent adherence to CLABSIs prevention strategies.
Educational institutions should integrate CLABSIs prevention education into nursing, medical, and other healthcare professional curricula. In addition, they should consider developing specialised training programmes focused on CLABSIs prevention for HCWs. Moreover, they should collaborate with healthcare organisations to provide practical training experiences and opportunities for students to apply their knowledge in real-world settings.
Footnotes
Acknowledgements
We would like to thank the data collectors and study participants for their cooperation in the process of data collection and provision of their information.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
Prior to conducting the study, an ethical clearance letter was obtained from Saint Paul’s Hospital Millennium Medical College, institution review board (IRB) Pm 23/410. Written informed consent was obtained from each study participant to ensure willingness. Information about the benefits and harms of the study, the usefulness of their participation, the confidentiality of the information, and the right not to participate were given to the participants. The data collectors were given two days of training on the study’s objective, relevance, and confidentiality of information, respondents’ rights, informed consent, and interview techniques in order to address potential ethical vulnerabilities of participants not to feel obliged to participate in the study.
Consent to publication
Consent to publication was not applicable, as this had no identifiable information of the patient.
Credit author statement
AWG: conception, design, acquisition, data collection, analysis and interpretation of the data, and drafting of the manuscript. ADW critically reviewed the study design, analysis, write-up of the report, and interpretation and drafting the manuscript. Both authors read and approved the final manuscript.
Data availability
All necessary materials used and/or analysed during the current study were included in the manuscript.
Use of Artificial Intelligence
Nil.