
Abstract
Introduction
Alopecia areata (AA) is a frequent and common immunologic disorder that causes loss of hair over the scalp. It manifests as an isolated patchy area of hair loss [Figure 1] or total hairlessness [Figure 2]. The proposed pathomechanism is autoimmunity, which can occur simultaneously with additional autoimmune ailments. In addition to autoimmunity, there is also an interplay of genetic, infectious, oxidative and psychological stress factors involved. AA also substantially influences several atopic individuals, decreases the quality of life and also has an impact on the overall well-being of patients suffering from the condition.[1,2]
Patchy alopecia over beard area

A clinical picture of alopecia totalis

AA history goes back to Roman physician Cornelius Celsus, who called hair loss patterns alopecia. ‘Alopecia Areata’ became the term’s name in 1763 when Sauvages used it, and English literature mentions Robert Willan’s perspective calling it ‘Porrigo decalvans’. Hebra and Kaposi discussed it in much more detail, keeping the concept more similar to modern times. Multiple theories on an infectious and even trophoneurotic hypothesis were being considered before Rothmund was voicing the autoimmune theory during discussions on Van Scott’s article.[1-4]
The predisposing factors of AA include genetics, autoimmune factors and environmental catalysts. The role of immunopathogenesis is characterised by the excessive inflammatory cytokines attacking the hair follicles and disrupting the immune cells, leading to the loss of immune privilege in the hair bulb.[5] Nevertheless, hospital-based studies worldwide observed different prevalence rates of AA, varying between 0.57% and 3.8%. In Indian studies, the incidence rate is 0.8% and the episodes last for less than six months.[3-7] No gender difference with incidence has been established, and conflicting evidence surrounds gender predominance.[4,9] Males are diagnosed at an earlier age and are predominantly occipital, while females show higher levels of extensive disease and medical comorbidities.[10-12]
The disease affects mainly younger individuals, with approximately 20% of patients reporting an onset before the age of 20 years.[13,14] Nail disorders are common and strongly associated with the severity of the disease, accounting for significant morbidity and psychosocial impact of the disorders that are frequently observed.[3,6,13] Atopy, especially atopic dermatitis, is common, and there is an association with a high prevalence of the diverse autoimmune diseases, supported by the presence of autoimmune antibodies in over 50% of patients.[3,14-16] This evidence suggests that AA might be a polygenic autoimmune disorder, sharing many genetic determinants and causes with other autoimmune diseases.[17-19]
The main target of this study is to summarise the various interesting clinical features of AA and its correlation with autoimmune diseases in an outpatient clinic. These different clinical aspects of the disease broaden understanding of possible management for the multifaceted disease.
Methodology
Patient Selection
This study is an observational cross-sectional study which includes 102 patients and was conducted for a period of 18 months from November 2019 to October 2021 in patients attending the dermatology outpatient department in a tertiary care centre at Warangal City, Telangana. The study included patients with alopecic patches of all ages and both sexes presenting to the outpatient department of dermatology. The exclusion criteria included patients who were not willing to participate and patients with background scarring alopecia to avoid unnecessary biases in the study.
Study Procedure
After detailed explanation and informed consent, all diagnosed cases of AA were enrolled in the study to include information such as name, age, sex and other relevant demographic details. The details and medical history were noted based on a predesigned Proforma covering the chief complaints: the period and course of onset of patchy hair loss, family history, medication history, dietary habits, any exposure to pets, concomitant systemic illness such as thyroid disorders, diabetes mellitus and connective tissue disorders.
Thorough, systematic and head-to-toe dermatological examinations were performed, including character traits of pattern, number, secondary changes and nail conditions. Visual inspection of the mucosa has also been conducted. Severity dimension of AA was estimated using severity of alopecia tool (SALT) rating scale assigning categories of mild, moderate and severe cases.
Basic blood tests like complete blood picture, renal function tests, random blood glucose, liver function tests and thyroid function tests were performed and values noted.
Statistical Analysis
The data was entered into the Microsoft Excel spreadsheet, and the final analysis was done with the use of Statistical Package for Social Sciences (SPSS) software, IBM manufacturer, Chicago, USA, version 25.0. For demographic data, the analysis was done in ratios and percentages. For clinical factors and to assess the autoimmune association in relation to severity, chi-square and logistic regression analysis were performed to find out the significance of the association. For statistical significance, a
Results
This research in-depth involved an overall analysis of 102 individuals diagnosed with AA, which is represented by a close-up investigation of different issues.
Demographic Characteristics [Table 1]
Within the cohort, there was a slight predominance of males, constituting 51.9% of patients compared to 48% females, resulting in a male-to-female ratio of 1.08:1. While the case here is a slight magnification of the gender gap, the influence of AA becomes quite similar among two sexes. Evidently, the majority of patients (64.9%) were aged between 16 and 45 years, which is congruent with the evidence of the articles in recent academic journals indicated about the condition’s typical onset early or middle adulthood. An interesting discovery is that the disease has a female predominance in this age group, even though overall there is male predominance. Males also had the overall history with the affected family member of 8.82%, although smaller but significant compared to females of 2.94%.
Demographic breakdown

Clinical Manifestations
It was widely seen that the scalp served as the primary region of the onset of this kind of alopecia, in around 85.3% of all cases, the occiput being the most commonly affected region. The pattern confirmed that the majority of patients (81.4%) suffered from the patchy subtype, and only 5.9% revealed subtotal destruction traced through ophiasis area. Particularly, nail changes represented in as much as 22.54% of patients, being pitting, is the most common actual alteration (13.72%) [Figure 3].
Nail pitting in AA

Through the SALT score, severity assessment was used to establish that most patients had mild variation (77.45%); furthermore, approximately 11.76% of patients had shown as severe, and only 10.78% of patients classified in the moderate category. This fact, however, illuminates significantly a very heterogeneous nature of AA with all the diverse clinical spectrums presented within the cohort. Another interesting point is that out of 12 patients in severe type, 10 patients (83.3%) had nail changes, emphasising the occurrence of nail changes as severity progresses.
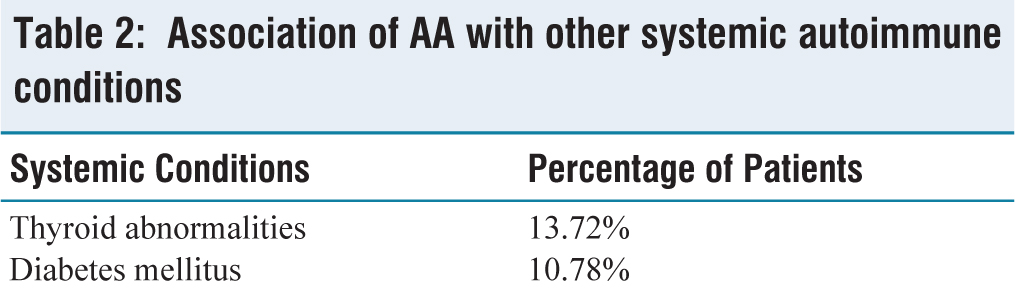
Associations with Systemic Conditions [Table 2]
Besides this, the research conducted a comprehensive analysis to explore the connections between AA and other systemic disorders with autoimmune aetiology, which resulted in the obtaining of invaluable data, which has opened up a discussion about their interdependency. Thyroid problems were the most diagnosed in 13.72% [Figure 4] of the patients out of which clinical hypothyroidism was the most prominent clinical finding. Interestingly, as the average severity of the disease rose, the percentage of patients having thyroid problems rose as well, what could indicate a correlation between the degree of the condition and the presence of thyroid abnormality. The chi-square analysis performed indicated a value of 18.69 which equals the
Association of AA with other systemic autoimmune conditions
Bar graph representing the percentage of thyroid illness across genders in relation to severity

The graph from logistic regression demonstrates that the probabilities increase significantly from mild-to-severe indicating a strong correlation between severity and the likelihood of thyroid abnormalities

Besides, whereas diabetes mellitus was observed in 10.78% [Figure 6] with equal frequency in males and females. In terms of severity of AA and diabetes mellitus, the logistic regression, although showed the odds of diabetes increase for moderate and severe cases compared to mild cases, the result is not statistically significant in this cohort of patients [Figures 7 and 8]. However, its increasing trend implies that there is an absolute need for detailing the metabolic tests in the AA patients because the results play an important role in managing the disease as well as in prognosis.
Bar graph representing the percentage of patients with diabetes mellitus across genders in relation to severity

Bar graph representing the probability of diabetes mellitus across the severity levels. Mild represents the baseline probability derived from logistic regression. The probability of moderate and severe illness increases compared to mild, but remains below 50%

The plot of regression analysis displays the log-transformed odds ratio for diabetes mellitus across severity levels along with 95% confidence intervals. The horizontal dashed line represents the baseline (mild severity with odds ratio = 1). The blue points show odds ratio for moderate and severe disease with error bars indicating the 95% confidence interval. Although the increasing trend of odds ratio with severity is evident, the wide confidence interval highlights the statistical insignificance between severity and diabetes mellitus

Discussion
Sex distribution analysis unveiled a marginal male predominance, with 52% of the cohort being males and 48% females, encapsulating a male-to-female ratio of 1.08:1. This finding, while slightly favouring males, aligns with previous research[6] indicating a similar trend of male preponderance with a ratio of 2:1. Psychological stress, including anger, frustration, and even depression, can emerge when social distancing and isolation become routine because of the disease. Age made a distributive nature of the elderly mostly belonging to the 15 to 45 versus of the age as 64.9% account for this age behind the cohorts.[20,21] The average age of detection resembled the statistics of Mirzoyez et al.[15] which showed the incidence at about 31 years, inferring that AA was susceptible for manifestation during early to middle adulthood, in all likelihood the result of underlying genetic predispositions and environmental triggers.
About 74.5% presented within three months of onset of the disease, signifying the immediate intervention sought by the patients to improve their cosmetic concerns.[10,21] A key element is the hereditary predisposition, which was immensely significant as there were 10.7% of the patients who reported a family history of AA of whom more males were identified. The close grouping of family members among the previous studies[3,8,10] has led to the conjecture of a hereditary nature in the initial causation, with an encouragement for more research works on classical genetics and genetic factors.
By far the scalp is the central area where the alopecia was observed to develop in 87 of the 102 (85.2%) cases, and most of the time the patients presented with patchy alopecia (81.37%), as other studies would depict similar cases. Although conditions like coronary heart disease, insulin resistance and metabolic syndrome have been mentioned in the literature before noticing the nail changes, it was not much explored. It was found that 22.54% had nail changes where pitting was very common, and it was a sign of the severity of the condition.[1,3,21,22]
There were more facial lesions in AA that correlated with the severity of the disease compared to mild-to-moderate forms, as eye and eyebrow hair involvement was more frequently found for severe ones. At the same time, the patients showed skin rash in 33.3% of cases, with atopic dermatitis (also mentioned by other studies) being the most observable.[3,6,10,23]
Individuals with certain manifestations of AA declared information related to the involvement of AA with systemic conditions, based on the influencing role of thyroid abnormalities in 13.72% of cases that were mainly hypothyroidism and an interesting fact that males had a higher incidence (64.2%) of this condition and there has not been much difference between the mean age of onset of disease between patients with the presence and absence of thyroid illness. More number of lesions were frequently seen in cases with thyroid disorder in comparison to diseased patients without thyroid illness. This study correlates with several other ones[1,3,10,16,24] and lends its supporting voice to the probability of a link between thyroid disorders and disease severity. AA has been linked to diabetes mellitus in 10.78% of the cases in our study, as similar to the study by Thomas and Kadyan.[24] Although the current data suggest increasing odds of diabetes with severity, the statistical significance is lacking. Although insignificant, this trend aligns with clinical expectations that disease progression might exacerbate the comorbidities like diabetes and suggest the need for evaluating it. Recent studies suggest that it is also associated with cardiovascular risk factors predisposing to coronary heart disease, insulin resistance and metabolic syndrome.[22] Thus, it is imperative for a comprehensive metabolic evaluation to be replete with all systemic measures and holistic treatment options to be considered in patients seeking treatment of AA.
Limitations
It is also important to consider the inbuilt limitations of this study here. Since the sample involved in the study is limited to a single hospital setting, that limits the external validity of the findings due to differences in patients’ characteristics and demographic factors across different hospitals. Also, since there is no long-term follow-up, the disease’s evolution over time and development of systemic conditions in future cannot be elucidated because of the cross-sectional design of the study. Considering the above factors, these might affect the generalisability of these findings compared to large cohort studies with long-term follow-up. Although the statistical association with diabetes suggests insignificance in our study, it might be of note that this might be the reflection of a smaller number of moderate and severe cases compared to milder presentations, which are the most common presentation in our cohort of patients. Nevertheless, in addition to thyroid, this association also needs to be evaluated in all the cases of AA for better management and holistic care of the patient.
Conclusion
This research focuses, nonetheless, on AA, and it is aimed at uncovering the connected clinical aspects and other probable causal factors. Distinguished research results include a 10.7% familial predisposition and a predominance of scalp involvement, especially in the occipital region, in 53.2% of these cases. Nail changes are detected in 12.74% of patients chance to be greater in the severe cases. Moreover, the survey’s respondents present a 13.72% rate of thyroid gland issues, most commonly hypothyroidism and 10.78% had diabetes mellitus. The findings reflect the autoimmune feature of the AA and support the multidiscipline solution in its care. Similarly, there is a need of conducting long-term, multicentric studies that are essential for enhancing the knowledge of the disease and refining the treatment regimens and, thus, yielding better results for patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
This study was approved by the ethical committee of Kakatiya Medical College, Warangal, in 2019
Informed consent
Obtained from patients and guardians in case of minors.
Credit author statement
Breethiga Velusamy, Shaik Noushin and Gugulothu Mounika helped in idea, conceptualisation, supervision and writing draft.
Breethiga Velusamy, Gugulothu Mounika, Shaik Noushin, Tirupathi Usha Rani and Kamatham Sruthi contributed to resources, project administration, writing and revision of the draft and approval of final draft.
Data availability
N/A.
Use of artificial intelligence
N/A.