
Abstract
Introduction
The effective management of malignant tumours of the limb remains one of the most significant challenges for orthopaedic surgeons. Amputation was once the standard surgical treatment for these tumours. 1 However, management of bone malignancies has become more specific and advanced with limb-sparing surgeries performed in up to 90% of all patients with bone and soft tissue sarcomas of the extremities. 1 This is due to advancements in diagnostic imaging and effective chemotherapy.2,3 Limb-salvage surgeries are now performed worldwide, and the outcome has improved with modern medical implant technology. Implant materials such as Vitallium 4 and a series of different metals such as stainless steel have now been replaced by titanium alloys. 5 Some of these implants are coated with silver to reduce infection risk. 6
With an increase in the number of surgeries involving endoprosthesis over the past decade, an inevitable rise in complications associated with these surgeries have been reported, such as aseptic loosening, infection, and mechanical failure.7-10 These complications occur at higher rates than other clean orthopaedic surgeries as soft tissue dissection is more complex, the implants are more extensive, and the biomechanical reconstruction following the surgery is complicated.11-13
Endoprosthetic infections can be considered the most devastating complication in limb-salvage surgeries. These surgeries are associated with higher infection rates as the procedures are more complex, with more extensive surgical wounds and longer operative time. Such resections often leave behind large areas of tissue defects, which lead to seroma formation, a potential nidus for infection.12,13 Furthermore, these patients usually undergo chemotherapy and radiotherapy and are at the extremes of age as a result of which they are generally immunocompromised and are prone to infection.14,15
To date, although many studies involving endoprosthetic infections have been reported worldwide, the focus has been on common sites involved, modalities of salvage surgeries, factors contributing to the development of these infections, and the types of microorganisms involved.16,17 However, data focussing on the functional outcome of patients who develop endoprosthetic infections are scarce.
Thus, this study explores the functional outcomes of patients who develop an infection after undergoing an endoprosthetic replacement for primary bone tumours. We also analysed the implant survival in these patients.
Materials and methods
We performed a retrospective cohort study involving patients with primary bone tumours treated with wide resection and endoprosthesis replacement over 20 years (1 January 1996 to 31 December 2016). We excluded cases that defaulted follow-up. This study was conducted at a tertiary referral centre for Orthopaedic Oncology and was approved by the Hospital Medical Ethics Committee (MEC ID No:2017911-5563). As this was a retrospective study, informed consent was not obtained from the patients. All patients were followed up for at least 24 months post-surgery.
Clinical information was collected by reviewing the medical records and the orthopaedic oncology database. The picture archiving and communication service (PACS) retrieved data related to radiological images and reports. Demographic and clinical data collected included age and gender, primary tumour site, local recurrence, metastasis of tumour, type of implant used and the implant outcome, including salvage surgery required for infected cases. The patients were divided into three age groups, that is, <20 years, 20–50 years and >50 years old. This is because types of tumours vary by age group. Children and adolescents under 20 years are mainly affected by primary bone tumours such as osteosarcoma and Ewing sarcoma. In adults aged between 20 and 50 years, chondrosarcoma makes up the majority of primary bone tumours, while metastatic disease predominates in adults above 50 years.
The functional outcome was determined by the Musculoskeletal Tumor Society (MSTS) 18 and the Toronto Extremity Salvage Score (TESS) 19 scoring system. These functional scores were taken from the patient’s latest follow-up. The MSTS scoring system focusses on an overall evaluation of the limb involved and patients' physical health. The physician asked specific questions and examined the patient to determine factors contributing to this scoring, such as pain, functional activity, and emotional acceptance. For the upper limb, specific characteristics were analysed, such as positioning of the hand, manual dexterity and the ability to lift. For the lower limb, the ability to walk, gait and the use of orthosis or supports were evaluated. These factors were then scored based on the proportion of expected typical outcomes for the patient. The Toronto Extremity Salvage Score (TESS) determines the functional outcome from the patient’s perspective. This scoring system was developed by adapting the definition of disability, handicap and impairment described by the World Health Organization (WHO). These questions are site-specific, and a score is given based on their ability to perform day-to-day tasks.20,21
We compared the MSTS and TESS scores for both the infected and non-infected endoprosthesis groups. We aim to establish if factors such as age, gender, limb involved, local tumour recurrence and metastatic spread would affect their functional outcome, as reflected by the MSTS and TESS scoring. Implant survivability was also determined in cases that had their implant retained.
There were two analyses involved in this research. The Mann–Whitney U test was performed using the Statistical Package for the Social Sciences (SPSS) software version 23. The non-parametric test was used when data were not normally distributed. The Mann–Whitney U test was used to compare the significant distribution in two dependent groups (MSTS and TESS) and independent groups (infected and non-infected) to ensure equal distribution of both groups.
To further understand an independent variable’s effect on the dependent variable, the SMART Partial Least Squares (PLS) modelling was performed using the SMART PLS software version 2.0. PLS-SEM was used to determine the factors contributing to or affecting functional outcome scoring in infected and non-infected groups. Factors analysed included age, gender, local recurrence, cancer spread and the limb involved. This data was then analysed using Variance Inflation Factors (VIF) to check on multicollinearity. A cut off value for VIF is expected to be lower than 5 to avoid affecting the loadings. Indicators that hit the critical values were omitted. The
Results
During the 20-year study period, 168 patients underwent endoprosthesis replacement for primary bone tumours. However, seven cases were excluded either due to loss to follow up or untraceable medical records. Of the remaining 161 patients, 18 (11.2%) had infected endoprosthesis.
Characteristics of endoprosthetic patients based on age, gender, and presence of infection.
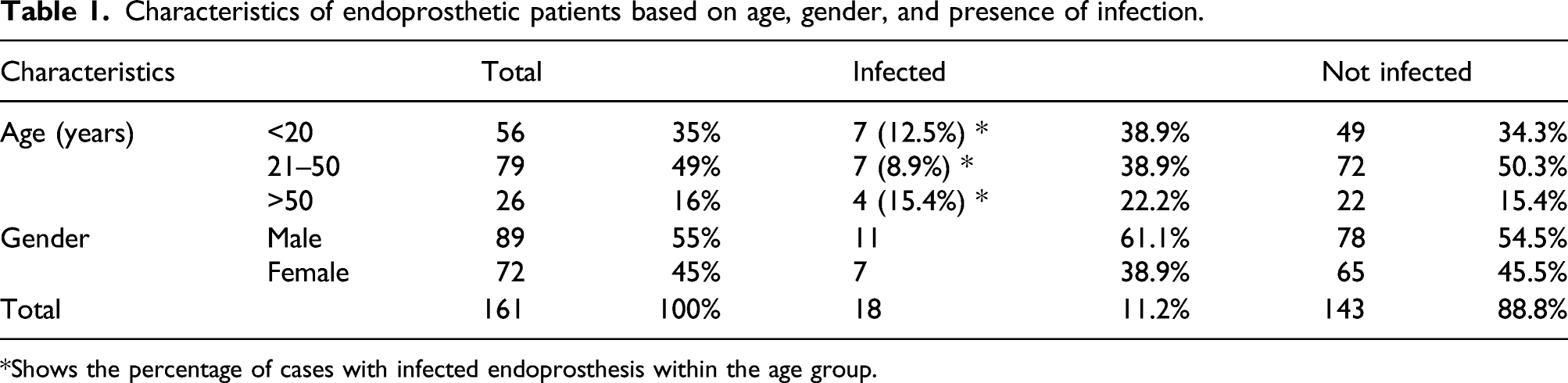
*Shows the percentage of cases with infected endoprosthesis within the age group.
Comparison between sites, local recurrence, and metastasis between infected and non-infected group.

Note: * excludes amputations and rotationplasty.
Infected endoprosthetic patients (

*Early: less than 90 days, Delayed: 90–365 days, Late: more than 365 days.
Comparison of Mean Rank between infected and non-infected implants and further subdivided into infected implant (resolved) and infected implant (persistent). MSTS AND TESS in both study groups.

Asterisks indicate significant results. **
MSTS AND TESS in both study groups without complications (excluding the amputation and rotationplasty).

Asterisks indicate significant results. **
MSTS AND TESS in infected implant (resolve) versus infected implant (persistent).

MSTS AND TESS in non-infected versus infected implant (resolved).

Asterisks indicate significant results. *
MSTS AND TESS in non-infected versus infected implant (persistent).

Asterisks indicate significant results. *
Factors contributing to functional outcome of infected endoprosthesis.

Asterisks indicate significant results. **
Implant survivability analysis was done for cases of the infected endoprosthesis, and results are shown in Figure 1. Out of the 18 patients with infected endoprosthesis, 10 (56%) had their implants removed. Of the 10 cases with removed implants, six were modular implants, and four were expandable implants. Out of the four cases involving expandable endoprosthesis, two (50%) underwent two-stage revision surgery. They had their implant changed to the modular type, while the remaining two cases underwent a rotationplasty. Of the six cases involving a modular endoprosthesis, two (33%) underwent two-stage revision surgery. One case underwent a rotationplasty, two cases underwent high transfemoral amputation and one patient underwent a hemipelvectomy (Figure 1). Outcome infected endoprosthesis cases.
The eight cases where implants were retained were the modular type. Six patients underwent repeated wound debridement. Out of these six cases, two cases involving the proximal tibia and one involving the distal tibia were cleared of infection. However, two cases involving pelvic tumours and one distal femur endoprosthesis had a persistent infection. The remaining two cases involving the distal humerus and the proximal tibia were not fit for two-stage surgery due to poor general condition.
Discussion
Deep surgical site infection is a devastating complication of endoprosthetic surgery. Out of 161 patients who underwent endoprosthetic replacement for primary bone tumours, 11.8% developed infected endoprosthesis. This rate concurs with other published studies, where the infection rates range from 10% to 17%.14,15,17,22 Infection rates of endoprosthesis replacements are generally higher than other orthopaedic implant-related surgeries as the surgical procedure is more complex, involving larger implants.11-13 The duration of surgery is also longer than routine orthopaedic surgeries, thus exposing large wounds to the external environment for extended periods. The bone tumour resection often leads to the formation of sizeable dead space, which eventually gets filled with seroma and haematoma, creating a focus for infection.12,13 Furthermore, many of these patients undergo neoadjuvant chemotherapy, which impairs their immunity, making them further susceptible to infection.14,15
This study’s main objective was to analyse the functional outcome of patients who developed infected endoprosthesis compared to patients without such infection. To the best of our knowledge, no other study has explored the functional outcomes of patients with an infected endoprosthesis in detail. Similarly, data are scarce on the contribution of age, gender, tumour site, infection, local recurrence, and metastatic disease on the functional outcome scoring in patients with an endoprosthesis. Thus, we carried out a detailed analysis to determine the functional outcome with other possible contributing factors.
Our results showed that the MSTS and TESS scores were significantly higher in those without an infected endoprosthesis, supporting the hypothesis that patients have a more unsatisfactory functional outcome once deep surgical site infection develops. Concurring with our findings, a recent study in Malaysia showed worsening functional outcomes in a small group of patients with endoprosthesis that developed deep surgical site infection. 23 We also found that patients' age significantly impacted the functional outcome in both the infected and non-infected groups. The favourable results in younger patients could be attributed to higher motivation, active lifestyle and better recovery compared to older patients.
Local tumour recurrence and metastatic spread contributed significantly to the functional outcome in the non-infected group but not the infected group. This disparity may be explained by patients with infected endoprosthesis already have lower functional scores due to the infection. Thus, local recurrence or metastatic spread did not contribute significantly to the worsening of the score. Gender did not significantly impact the functional outcome in both the infected and non-infected endoprosthesis cases.
Our findings showed that tumour recurrence was lower in cases of an infected endoprosthesis compared to uninfected subjects, however it was statistically insignificant. This is probably due to the small number of patients with local recurrence in the infected endoprosthesis group. We postulate that infection might confer a protective effect on the local recurrence of the tumour. Similarly, previous studies have shown that postoperative infection in osteosarcoma patients was associated with prolonged survival and reduced local recurrence compared to non-infected patients.24-26 Reports of tumours spontaneously regressing following infections had been described historically. In 1891, William B. Coley, often regarded as the ‘Father of Immunotherapy’, purposely injected live streptococcal organisms into a patient with an inoperable sarcoma, ultimately shrinking the tumour.
27
Because of the threats of live streptococcal, Coley developed a heat-killed streptococci vaccine combined with
The exact mechanism of how infection reduces the local recurrence rate is still unclear. Some authors believe that the infection has an antitumour effect by up-regulating the cellular immune system, which causes an increased release of tumour necrosis factor-α. 27 Buddingh et al. 29 (2012) stated that chemotherapy-resistant osteosarcomas could be lysed by natural killer cells (NK cells). Laboratory studies have shown that infection causes angiosuppressive effects on tumour cells. 30 These factors enhance the innate immune response and have a protective effect, which reduces the tumour recurrence rate. However, despite the findings that infection protects against local tumour recurrence, more advanced studies are needed to support the validity of these postulations. 24
In case of an infected endoprosthesis, treatment options include surgical debridement with irrigation, a single-stage or two-stage revision.31-33 Most surgeons currently perform a two-staged revision, as the success rate is higher than a single-staged revision in controlling the infection.34,35 The success rate of a two-stage surgery with the usage of antibiotic-impregnated cement is 90%. 36 The cases with persistent or repeated infections despite multiple surgical debridements or a two-staged surgery can be offered rotationplasty or amputation, depending on the tumour site. In our series, rotationplasty was performed in three patients and amputations in another three patients (2 above knee amputations and one hemipelvectomy). Other options, such as arthrodesis or resection arthroplasty are not commonly done in our centre as there huge bone gap after removal of these prosthesis and we do not use have the availability of fusion prosthesis.
Orthopaedic implant infections remain challenging to eradicate, contributed mainly by biofilm formation, protecting bacteria from the host immune response and systemic antibiotics. As colonization of the prosthesis precedes infection, newer implant coatings with antimicrobial properties have been explored to minimize bacterial colonization and ensuing infections. One promising technique involved iodine coating of the titanium implant, which was shown to have antibacterial activity, cytotoxicity and biocompatibility. 37 Tsuchiya et al. 38 subsequently conducted a clinical trial on 222 patients fitted with iodine-supported titanium implants. In 158 patients, these implants were inserted in patients with compromised status to prevent infection, while in 64 patients, it was inserted to treat an implant infection. Only three patients from the preventive therapy group developed an infection, which resolved without implant removal. In the infected group, all 64 cases had resolution of the infection. Another modality that is currently available is the silver-coated endoprosthesis. 39 Silver has excellent antimicrobial activity and low toxicity and has reduced the infection rate in primary and revision cases. 39 Even in cases of an infected endoprosthesis, patients with silver-coated implants needed more minor interventions, for example, debridement or one-stage revision, to overcome the infection than those without silver coating. Eradication of an established biofilm entails disrupting the extracellular polymeric substances (EPSs) and killing bacteria cells. 40 Phage therapy can achieve both, making it a promising new paradigm for the treatment of orthopaedic-device related infections. This treatment uses viruses with specific lysis ability injected into the infection site to kill the infecting organism. Preclinical and clinical studies using phage therapy have shown promising therapeutic effects and safety profiles, especially when combined with antibiotics, as both agents can work synergistically against biofilms. 40
This study has helped us improve our practise over the years to minimise the incidence of infection. We have now standardise our antibiotic regime. We now give intravenous antibiotics until the drains are removed and continue with oral for a total of 2 weeks. In additional to that, we intervene early in cases of wound dehiscence and those cases with persistent high drainage postoperatively by doing wound wash outs.
We acknowledge that our study has a few limitations. Since this was a retrospective study, the functional scores for patients before developing infection were not available. Thus, the comparison could not be made between the functional scores before and after infection. Moreover, this study had a relatively small number of infected cases, resulting in a low statistical power to detect true association.
Conclusion
We found that infection significantly affected the functional outcome of patients with an endoprosthesis. Age was a significant contributing factor for the functional scoring in both the infected and non-infected endoprosthesis cases. Local recurrence and metastatic cancer spread significantly impacted the scoring of the non-infected group compared to the infected group. Intriguingly, patients with infected endoprosthesis had a significantly lower recurrence rate of the tumour. In only 44% of the infected endoprosthesis cases, the primary implant was retained.