
Abstract
Introduction
Reassurance has been defined as the removal of fears and concerns about illness (Traeger et al., 2017). The importance of delivering effective reassurance, to modify patients’ thoughts, reduce their distress, or change behavior (Linton et al., 2008), is reflected in low back pain (LBP) and sciatica guidelines (NICE, 2016; Oliveira et al., 2018), and recent Low Back Pain Clinical Care Standards (Australian Commission on Safety and Quality in Health Care (ACSQHC), 2022). These guidelines/standards recommend that clinicians provide patients with consistent and reassuring messages about the benign nature of LBP, and a favorable prognosis (ACSQHC, 2022). Clarifying patients’ concerns and understanding their agenda is considered a fundamental prerequisite for giving effective and targeted reassurance (ACSQHC, 2022; Pincus et al., 2013). However, health professionals can feel challenged with regard to eliciting patients’ concerns, resulting in a negative impact on the consultation. For example, in medical encounters, it has been demonstrated that clinicians seldom elicit the patient’s agenda (Singh Ospina et al., 2019) and interrupt the patient’s disclosure (Beckman & Frankel, 1984; Coyle et al., 2022; Roberts & Burrow, 2018), reducing the chance of them orienting to a patient’s priorities. Physiotherapy is no exception in this regard with physiotherapists demonstrating similar challenges in balancing their own “professional” agendas with those of the patient (Cowell et al., 2019; Hiller et al., 2015; Josephson et al., 2015). These conflicting professional and patient agendas (Hamilton & Britten, 2006) represent a potential impediment to effective reassurance if the patient’s perspective and concerns have not been successfully solicited (Cowell et al., 2019).
Although clinical guidelines emphasize the importance of reassurance in the consultation, they provide little guidance on how physiotherapists should best deliver and optimize the reassurance they offer patients (NICE, 2016; Oliveira et al., 2018; Wellman et al., 2020). It has been suggested that “good” clinical practice should include a combination of affective reassurance (displaying empathy and building patient rapport) and cognitive reassurance (improving the patient’s knowledge and understanding of their condition through education) (Cheung & Soundy, 2021; Holt et al., 2018). In primary care consultations, it was found that cognitive reassurance was associated with improving patient satisfaction, building patients’ sense of empowerment to self-manage, reducing patients’ concerns, and improvements in patient clinical symptoms, and reduced health care utilization rates (Pincus et al., 2013). However, these findings were from a 2013 systematic literature search and there is currently limited evidence as to why these different components of reassurance are important to clinical practice (Cheung & Soundy, 2021).
Moreover, the best approach to reassure patients with back pain–related fears and concerns remains unclear. This may be partly because the evidence on the effects of reassurance on pain-related problems is limited and inconsistent (Linton et al., 2008; Traeger et al., 2017). While some studies demonstrate lasting positive effects of giving reassurance (Traeger et al., 2015), other studies specify the importance of clear guidance and understanding when the clinician is giving reassurance. Without this, the aim of the reassurance is not clear and this can have potentially negative consequences. These can include increasing patient concern and emotional distress including catastrophization, avoidance behavior, and negative affect (Fantry, 2016; Linton et al., 2008; Traeger et al., 2017) leading to overutilization of health resources (Giroldi et al., 2014).
There are currently no published systematic or scoping reviews that describe the content and methods of delivery of effective reassurance for patients with LBP. Therefore, building a better understanding of how physiotherapists reassure patients and how patients respond to those efforts during an initial consultation is important to optimize how reassurance is delivered effectively to patients with LBP. There are no previous studies that have microanalyzed, in granular detail, how physiotherapists and patients interactionally co-construct reassurance during an initial consultation for patients with LBP.
The aim of this observational study, employing conversation analysis (CA) (Maynard & Heritage, 2005), was to examine, in forensic detail, actual instances of when and how physiotherapists reassure patients and how patients respond. Our previously published research, based on the same data corpus (Cowell et al., 2019), explored how physiotherapists solicit and explore patients’ concerns, and focused mainly on the spectrum of communication styles (i.e.,
Methods
Setting
The setting for this study was two outpatient physiotherapy departments in primary care in the North-East London Foundation Trust (NELFT), England.
Participants
This observational study was nested in a larger study, conducted over a 3-year duration, examining the training requirements for the implementation of a bio-psychosocially oriented behavioral intervention called cognitive functional therapy (CFT) (Kent et al., 2023; O’Sullivan et al., 2018). These data were collected in 2016 prior to the CFT training program. Twenty initial physiotherapy consultations were video-recorded (10 physiotherapists and 20 patients). To ensure heterogeneity, 12 physiotherapists were purposively sampled based on sex, age, levels of clinical experience, and previous bio-psychosocial training. Two physiotherapists declined to participate due to time commitments. Their clinical experience ranged in years qualified from 4 to >14, with the majority of the experience gained in a musculoskeletal setting (range 3 to >14 years). Previous post-graduate bio-psychosocial training ranged from 0 to 12 days. Twenty-seven patients between the ages of 18–70 years, reporting non-specific chronic LBP >3 months, including a range of risk profiles for predicting non-recovery from LBP (see below for more details), were identified in two NELFT physiotherapy departments from either the triage clinic or the musculoskeletal clinical assessment and treatment service. The patients were contacted by a member of the research team (RP) and the NELFT direct care team. For patients willing to participate, an initial face-to-face meeting was then arranged with the lead researcher (IC) to explain the reasons for the study and the requirement for the interaction to be recorded and for the lead researcher to be present during the consultations. One patient declined to participate, as she did not want to be video-recorded, four withdrew due to resolution of symptoms, and two failed to attend their initial assessment, leaving 20 patients included in the study (11 women and 9 men). The ages of the patients ranged from 26 to 67 years (mean of 47.2 years). The patients completed several questionnaires, which included the Ørebro Musculoskeletal Pain Screening Questionnaire (ØMPSQ) (Boersma & Linton, 2005), Roland and Morris Disability Questionnaire (RMDQ) (Roland & Morris, 1983), the STarTBack Screening Tool (Hill et al., 2008), and a measure of pain intensity on a 0–10 pain numerical rating scale (NRS) (Boersma & Linton, 2005). These questionnaires were administered to understand the risk profile of the patients included in the study in terms of predicting non-recovery from LBP and were consistent with usual practice in the NELFT physiotherapy departments. The ØMPSQ scores ranged from 69 to 163 (mean score of 115.9). The RMDQ scores ranged from 1 to 22 (mean score of 10.8). The patients’ estimated risk profile for developing persistent LBP measured on the STarTBack Screening Tool included 4 patients at low risk, 8 medium, and 8 high. The NRS scores ranged from 2 to 10 (mean score of 6.6). The recorded consultations ranged in duration from 35 minutes to 1 hour. The lead researcher was present at the recorded assessments to adjust the camera as required. Follow-up treatment sessions were not recorded.
Analysis
Transcription Convention Used in Extracts.

Ethics
The local research ethics committee approved the study (Reference Number: 2352), and it was successfully reviewed by the East Midlands-Nottingham 2 National Research Ethics Service committee (14/EM/1045). All patients and physiotherapists that agreed to participate in the study were sent an invitation and information sheet and provided written informed consent prior to participation in this study which included authorization to use their transcripts and images in scientific articles.
Results
Summary of Extracts.

Physiotherapists’ Reassurance Not Targeted to Patient’s Concerns
Failure to Solicit Patient’s Concerns During a Reassurance Sequence
Description of Key Features
Extract 1 comes at the end of the consultation, in the explanation and planning phase. It starts with the physiotherapist’s empathic statement recognizing the impact that the LBP has had on the patient: “I can see …. is .. really affectin- you.” This is acknowledged by the patient with a simple nod of the head. What follows in the next turn is the physiotherapist’s attempt to reassure the patient, which is initially constructed as a broad reassuring statement (lines 07–08): “don’t be too concerned.” The physiotherapist then specifically targets the patient’s scan findings (lines 09–10 and 12–14), presuming that this is the patient’s focus of concern. The physiotherapist frames the patient’s findings as minimal: “it’s not it’s not a [major thing].” We observed similar examples in these data of physiotherapists minimizing the patient’s condition in this way to communicate more positive perceptions about patients’ scans (see also extract 2, lines 40–45; extract 3, line 16; extract 4, lines 49–52). However, the patient’s overlapping response (lines 15–16) and the interactional features of that response indicate some resistance to this. The cut-offs on “[Yeah that’s]- that's,” and the quiet downward intonation of

Failure to “Pick Up” on the Patient’s Lack of Response to Concern-Seeking Question
Description of Key Features
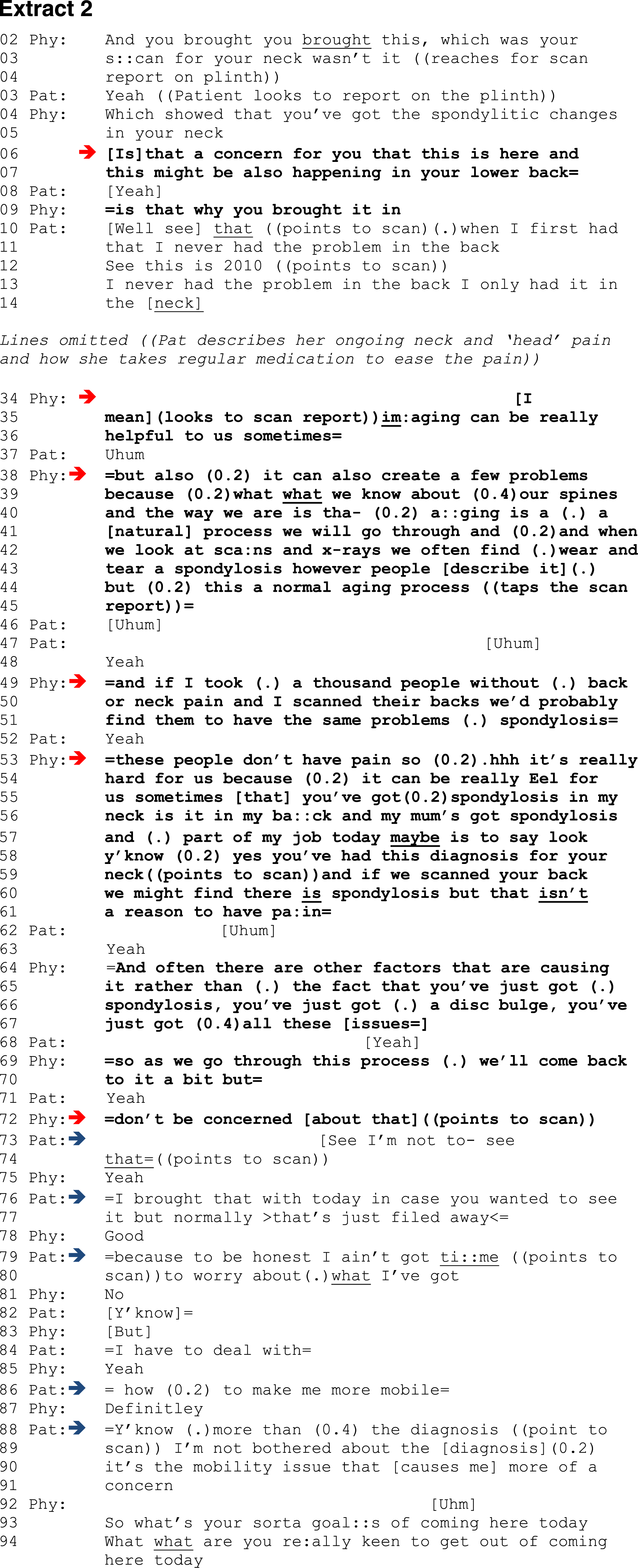
Extract 2 is positioned early in the interview and starts with the physiotherapist’s reference to the patient’s MRI report of her cervical spine. The physiotherapist’s concern-seeking question is a polar/closed question that invites a constrained yes/no response: “Is [that] a concern” … “is that why you brought it in,” (lines 06–07 and 09). The question appears to reflect his presumption that the patient has brought the scan report to the consultation due to concerns that similar “wear and tear” changes have developed in her back. The patient’s response in line 10 is “well” prefaced and operates here as an indication that the answer is unlikely to be straightforward. The patient does not answer the physiotherapist’s question but instead launches a narrative over multiple turns describing how she has learned to live with neck pain and is now more concerned about developing LBP. Although the patient does not directly answer the question about the report, the physiotherapist still attempts to offer the patient reassurance about the scan findings over multiple turns (lines 34–36, 38–45, 49–51, 53–61, 64–67, 69–70, and 72). This “normalizing,” which continues over multiple turns, fits a typical structure in these data (see also extract 3 lines 21 and 25; extract 4 lines 49–50)—that ageing is a normal process and that these findings are common in the asymptomatic population. The physiotherapist also speculates that the patient may harbor some fear about the diagnosis: “fearful for us sometimes.” Despite receiving only simple acknowledgments from the patient throughout this sequence: “[Uhum]” and “Yeah,” the physiotherapist signals to the patient that her concerns about the report will be discussed further during the course of the examination: “we’ll come back to it a bit.” The physiotherapist’s reassurance statement in line 72: “=don’t be concerned [about that]” ((points to scan)), makes clear his assumption about the patient’s concerns, and prompts an overlapping disaffiliative1 response from the patient:
Extract 2 provides further illustration of the difficulty some physiotherapists have in establishing the patient’s main concern and the importance of picking up on the patient’s responses to concern-seeking questions (in this case a lack of response). Part of the issue lies in the fact that the cues that patients give may be misleading and dissonant from their actual concerns. As in extract 1, this extract illustrates how the physiotherapist handles/mishandles the patient’s concerns, presuming the patient is concerned about the MRI report of her cervical spine and so directs reassurance to this end. This presumptive approach results in misalignment between patient and physiotherapist. It also highlights how physiotherapists can risk wasting considerable time by providing generic evidence-based information largely irrelevant to the patient’s specific agenda of concerns.
Not Engaging With the Patient’s Explicit Response to Concern-Seeking Question

Description of Key Features
Extract 3 is positioned halfway through the interview and starts with the physiotherapist asking whether the patient has had previous imaging for his LBP. The patient reports that he had had an x-ray which had revealed “nothing” or possibly a “slight ↑curvature.” In lines 12–13, the physiotherapist’s concern-seeking question is designed to solicit any concerns that the patient may have about these findings: “how do you feel about that is it something that’s bothered you at all.” The patient’s response in line 14 rather emphatically conveys that this is not of concern to him: “No ((shakes head)) no it ain’t bothered me.” Despite the patient’s response, the physiotherapist provides a reassurance sequence over the next two turns minimizing the patient’s x-ray findings as minor and common. This receives only minimal acknowledgment from the patient (“Yeah,” “Uhum,” “Okay”). Extract 3 provides further illustration of the importance of “actively” listening and engaging with patients’ responses to concern-seeking questions in order to target reassurance more effectively to patients’ actual concerns.
Reassurance Targeted to Patient’s Concerns
Engaging With Patient’s Responses to Concern-Seeking Questions

Description of Key Features
Extract 4 is positioned toward the end of the interview. The extract starts with the physiotherapist and patient discussing the patient’s recent x-ray findings, which had revealed “a bit of arthritis.” As similarly observed in extracts 2 and 3, the physiotherapist employs a concern-seeking question (lines 25–26): “Have you got any concerns about what was on (.) the x-ray or.” In this extract, the patient voices his concern that working outdoors might exacerbate the arthritic changes observed on the x-ray (lines 28–35). The physiotherapist’s follow-up question seeks to fully understand the patient’s perspective and to clarify whether the patient attributes his current stiffness symptoms to the arthritic changes on the x-ray. The patient’s response is typical of how patients offer their perspectives on symptom attribution in these data with the use of weak evidential markers3: “Quite possibly yeah,” “contributes to it,” and “whether it is or not,” which seem to be used to downgrade assertions and indicate uncertainty about their knowledge. Although the physiotherapist acknowledges the patient’s perspective, he suspends judgment about the specific association of the x-ray findings to the patient’s symptoms at this point in the examination: “We’ll look into that.” However, in the next two turns, the physiotherapist does attempt to offer the patient some reassurance by providing evidence-based information about x-ray findings. This reassurance sequence casts doubt on the relevance of these findings to the patient’s symptoms. The “mixed message,” “we all have some,” and “normal process” communicate to the patient that the findings are “normal” and not significant. The physiotherapist’s assessment of the patient’s x-ray (lines 52 and 55): “doesn’t look horrific or anything we need to worry about,” includes the lexical choice of “horrific” which, although semantically extreme, is designed here to reassure the patient by providing a non-literal reference to more extreme cases. The physiotherapist emphasizes that his reassurance is based on the report and suspends a full assessment until further data gathering has been completed: “we’ll see if that’s [contributing] to what you’re having there.”
Extract 4 provides further illustration of how physiotherapists commonly offer reassurance through normalizing imaging findings. However, in contrast to extracts 1–3, the physiotherapist first solicits the patient’s concerns about the x-ray findings and engages more appropriately with the patient’s responses before offering reassurance clearly tailored to the patient’s concerns. This collaborative communication approach allows the patient to participate more in the interaction and helps to accurately establish the patients’ concerns as a platform for targeted reassurance.
Disconfirming Patient’s Fear via a “Behavioral Experiment”

Description of Key Features
Earlier in physical examination (prior to this sequence and not shown in this extract 5), the physiotherapist had solicited the patient’s concerns about bending, which he avoids as he is concerned “[That it’s] going to hurt my back.” Extract 5 starts with the physiotherapist returning to the patient’s concern by asking him to bend to the floor from the sitting position. The physiotherapist’s positive assessment of the patient’s movement, “It’s alright isn’t [it],” which is synchronized with a nonchalant shrug of the shoulders, appears to highlight disconfirming evidence to the patient about his worries that bending will “hurt.” In lines 08–09 the physiotherapist amplifies the patient’s concern by asking him to bend from a standing position, a position the patient had previously indicated (prior to this sequence and not shown in this data) as particularly worrying for him (“I think it’s the distance”). The patient cautiously performs the bend a couple of times, his anxiety audible with a large in-breath and embodied by a worried facial expression and nervously oscillating his hands. The physiotherapist’s evaluation of the movement, “That looks NI:CE,” is designed to reassure the patient. However, the physiotherapist detects that the patient is still worried, which prompts a concern-seeking question (lines 17–18 and 20) about the tightness the patient is experiencing: “have you got any worries about that?”. This gives the patient space to elaborate on his concerns fearing that his back might “[jus:: go],” an idiomatic expression for his back going into painful spasm. The physiotherapist’s supplementary and open question (lines 28–29) attempts to develop further the patient’s concerns and provides opportunity for the patient to reiterate that he is worried that his back “might just start to seize up.” Line 36 marks the start of a multi-turn reassurance sequence in which the physiotherapist begins to gradually expose the patient to his pain-related fear of bending. The initial position is side lying with the patient’s knees bent to his chest. The physiotherapist’s question: “Do you feel anything,” guides the patient toward an appreciation of his bodily responses. The patient’s response: “No it’s really actually very comfortable,” is the start of developing patient insight and allowing him to experience disconfirming evidence to challenge his expectation and concern of developing pain. The physiotherapist then emphasizes that in this position, the patient’s back is actually “fully flexed” (i.e., the position the patient fears), which implicitly challenges the basis of the patient’s concern. In lines 48–49, the physiotherapist proposes to the patient that the problem is not bending per se but how he bends: “it’s the process of how you get into these positions,” and that he is guarding his back due to a lack of confidence to move. In lines 55–56, the patient strongly affiliates to the physiotherapist’s representation of his back pain: “Yeah that’s that’s a lot of (0.2) lot of the problem I’ve had.” Over the next few turns, the physiotherapist progresses the start position to kneeling and attempts to modify the patient’s guarding responses by using breathing techniques and again guiding the patient to his bodily responses and to recognizing that the feared outcome has not occurred: “tell me what it feels like now” and “do you feel anything at all now here.” The patient responds with a positive assessment: “A lot better actually” and “it’s better than it was.” The physiotherapist’s follow-up Wh-Q: “Why is that?”, orients to the importance of developing the patient’s awareness and insights into his back pain. The patient’s developing understanding is clearly displayed in lines 99–100 where he recognizes his protective responses: “Yeah I suppose it’s the guard .. mechanisms.” This receives a strong agreement from the physiotherapist: “I totally agree with you,” who positively frames the patient’s “bending” as “a lovely (0.2) flexed position” without “any discomfort.” Having elicited the patient’s perspectives, the physiotherapist offers a more direct assertion, “I think that key is that your your back can [go into this position],” in lines 105–106. The patient responds with a simple acknowledgment and then reveals his insights by offering an account explaining that his back has tightened due to the length of time he has experienced back pain.
Extract 5 provides further illustration (similar to extract 4) of the importance of physiotherapists first eliciting the patient’s perspective and engaging in collaborative dialogue to establish what the patient is worried about before giving targeted reassurance. It also illustrates how some physiotherapists go beyond simply providing reassuring information and employ behavioral experiments in the physical examination as a reassurance strategy to test and disconfirm patients’ movement-related fears. We observed how the reassuring potential of these experiments was augmented by the physiotherapist’s simultaneous assessment commentary: “That looks NI:CE,” and a style of communication that encouraged patient reflection and insight into the disorder.
Discussion
Reassurance is considered patient supporting (Pinto et al., 2012) and in the context of LBP is perceived by patients to be an important part of a “good back consultation” (Holopainen et al., 2020; Laerum et al., 2006), which is reflected in recent Low Back Pain Clinical Care Standards (ACSQHC, 2022). Although patients value patient-focused communication where clinicians actively listen to their “thoughts, worries/feelings” (Laerum et al., 2006), these data suggest a need for physiotherapists to more adequately explore patients’ concerns and “actively” listen to patient responses before attempting to give reassurance.
Reassurance is recognized as a complex intervention (Giroldi et al., 2014), and simple “knee-jerk platitudes and messages of hope” (Traeger et al., 2017) are considered ineffective and risk increasing emotional distress. However, the best way to allay patients’ concerns and worries remains elusive (Karran et al., 2018). These data provide interesting insights into physiotherapists’ reassurance practices, which typically focused around educating patients and providing them with positive information about their scan findings, framing the findings as normal or minimal (see extracts 1–4). Biomedical beliefs are pervasive in western society (O’Sullivan, 2012), which are often influenced by unhelpful interpretations of normal age-related scan findings that are poorly associated with pain (Traeger et al., 2015). Providing explanations about normal image findings has clear reassuring potential (Karran et al., 2018) and aligns with guidelines for recommended practice (ACSQHC, 2022; NICE, 2016). However, evidence-based education individually tailored and relevant to patients’ concerns is likely to be more effective than generic educational messages (Cowell et al., 2019; Maguire & Pitceathly, 2002; Traeger et al., 2017). In these data, some physiotherapists assumed that
Research in other contexts has shown that a failure to fit advice to the advisee’s “problem” creates resistance (Heritage & Sefi, 1992; Park, 2014). Similarly, in these data, we observed how patients displayed their resistance explicitly when physiotherapists failed to tailor their reassurance to their concerns: “I’m not bothered about the [diagnosis] (0.2) it’s the mobility issue that [causes me] more of a concern” (see extract 2 lines 89–91). Their disaffiliative stance was also embodied “((looks to the floor))” (see extract 1, lines 15–16) and facially expressed “((despondent look)” (see extract 1, line 16).
We observed in these data how physiotherapists can invest considerable interactional effort and time, often over multiple turns of talk, delivering ineffective reassurance due to a failure to ascertain patients’ actual worries and fears (see extract 2). It has been recommended that the health care system must place greater value and investment on innovations that create the time required to deliver patient-centered approaches (Pieterse et al., 2019). However, it is also important for physiotherapists, with the acknowledged time constraints in primary care, to reflect on individual practice and to use the time they have more judiciously (Cowell et al., 2018), through a collaborative style of communication, where patients are encouraged to actively participate. Active patient participation contributes to improved health outcomes and quality of care, but is heavily dependent on the practitioners’ communicative style (Street et al., 2005).
We observed in these data a few examples of more patient-focused sequences where the physiotherapist’s reassurance was more targeted to the patient’s concerns. In these more collaborative exchanges, the physiotherapists actively engaged with the patient’s responses to their concern-seeking questions and typically employed secondary prompts/questions to build a better understanding of patients’ concerns. These concern-seeking sequences then provided the basis for more appropriately targeted reassurance (see extracts 4 and 5) with less interactional “trouble” in terms of patient resistance.
In these more targeted sequences (extract 5), the physiotherapist, when addressing the patient’s fear of movement, went beyond just providing reassuring information and employed behavioral testing in the physical examination to allay the patient’s concerns. In this more elaborate sequence, the physiotherapist gradually exposed the patient to the bending movement he feared while attempting to modify his protective responses. This use of guided behavioral experiments to disconfirm patients’ fear of movement has been advocated as an effective model of reassurance and may be more effective than simply providing information (Linton, 2005; Linton et al., 2008). Behavioral experiments are planned in the physical examination and attempt to achieve pain control through graded exposure to movements and activities that are nominated by the patient in the interview as painful, feared, or avoided (Kent et al., 2023; O’Sullivan et al., 2018). An interesting communication feature in this extract was the physiotherapist’s contemporaneous evaluation of the movement that appeared to have a reassuring function: “That looks NI:CE,” “a lovely (0.2) flexed position.” A similar type of communication approach designed to reassure patients, termed “online commentary,” has been observed in medical interaction, where physicians describe what they are seeing, feeling, or hearing during physical examination (Heritage & Stivers, 1999). The physiotherapist’s communicative practices employed in this sequence, including eliciting the patient’s perspective, reflective questioning, and guiding patients toward their bodily sensations, speak to the importance of developing patient’s understanding of their disorder. Rather than reassurance being imposed on the patient, as we observed in extracts 1–3, the reassurance we observed in extract 5 was grounded in a collaborative process in which the patient was helped to “play a part” in understanding why the feared outcome had not occurred. Extract 5 provided the strongest illustration of patient affiliation4 to reassurance, and it would appear that integrating behavioral testing to dethreaten pain experience may offer promise in reassuring and directing patients toward “active” behavior change.
Giving reassurance is common practice for physiotherapists when treating patients with LBP and is consistent with best practice for treating people with musculoskeletal pain (Lin et al., 2020). It is intuitive for clinicians to want to allay/reassure patients’ concerns (Kathol, 1997). However, providing patients with reassurance unrelated to their expressed concerns has been described as “worthless” (Balint, 2000). In these data, we have observed that despite physiotherapists’ eagerness to provide reassurance, it was not always effective or efficient. The interactional difficulties observed in these data (extracts 1–3) might point to physiotherapists feeling more comfortable with information giving and “reciting” evidence-based messages than engaging in the more skilled communication practice required to better understand patients’ concerns. Encouragingly, we also observed in extracts 4 and 5 how a more collaborative style of communication, where the physiotherapists encouraged patients to actively contribute to the interaction, allowed for a better understanding of their concerns and the delivery of more targeted reassurance.
Practice Implications
Delivering reassurance and addressing patients’ biomedical misconceptions about the cause of their back pain are clear evidence-based messages. Although we did not measure patient outcomes, our analysis suggests that for these key evidence-based messages to be effective and perceived as reassuring by patients, they need to be aligned to patients’ concerns. It is therefore important for physiotherapists not to make assumptions about concerns that patients might have and encourage a dialogue with patients, listen to their concerns, and take them into consideration before delivering their reassurance. Giving patients the opportunity to provide a full account of what concerns them is likely to contribute to patient satisfaction and enhance the therapeutic relationship. The use of behavioral experiments during the physical examination has been previously described as a central component of physiotherapy-led CFT (O’Sullivan et al., 2018) and may offer promise in providing active reassurance. Training physiotherapists to carefully explore patients’ concerns and adapt their communication to the individual needs of the patient, both within the interview and physical examination, is likely to be important.
Limitations
This relatively small corpus of interactions, undertaken in the United Kingdom in two settings in primary care only, does not claim to represent a comprehensive description of reassurance practice, and therefore there can be no claim to generalizability. However, these data do illustrate the
Conclusion
These data illustrate that giving reassurance in a physiotherapy context is common and typically involves some form of information giving. We observed how some physiotherapists give reassurance directed by what they considered to be important or what they assumed the patient was concerned about. This more physiotherapist-focused style of communication appeared ineffective and was often resisted by patients. We also observed examples where the physiotherapists more actively engaged with the patient’s responses to build collaboratively a better understanding of patients’ concerns, which provided the basis for more tailored and patient-focused reassurance with less interactional “trouble” and greater patient affiliation.