
Abstract
Keywords
Maternal mortality is a pressing “social tragedy” (Souza et al., 2024) where women and childbearing people lose their lives. Maternal mortality, also called maternal death, relates to the tragic deaths of women due to complications from pregnancy or childbirth (United Nations Children’s Fund, 2023). Currently, the global maternal mortality ratio is 223 deaths per 100,000 live births (Khalil et al., 2023). Haiti is a relevant context to better understand maternal mortality. Haiti’s maternal mortality ratio is 480 maternal deaths for every 100,000 live births—more than double the global ratio (United Nations Development Programme, 2024). Access to comprehensive emergency obstetric and newborn care, and birth in health facilities, or with skilled birth attendance, is an ongoing serious challenge in Haiti. According to Haitian data sources, in 2018, 42% of births were attended by skilled birth personnel and 39% of births were attended at health facilities (Institut Haïtien de l’Enfance [IHE/Haiti], 2018; Pan American Health Organization, 2023). Women may choose not to attend a health facility or have many challenges accessing a health facility and receiving adequate care there (Raymondville et al., 2020). Haiti’s unacceptably high maternal mortality ratio has only worsened in the wake of the current political and economic crisis (UNICEF, 2022). During this crisis, there are an estimated 315,000 pregnant women and adolescent girls in need of emergency primary healthcare (UNICEF, 2022).
Maternal death is only the “tip of the iceberg” because it has been suggested that for every maternal death, there are between 20 and 30 women who suffer from morbidity and disability after childbirth (World Health Organization, 2024). When women suffer from maternal morbidity, their lives are not lost but their health and well-being are seriously impacted (WHO, 2024). Another important indicator is maternal near-misses, defined by the World Health Organization as when a person narrowly survives a grave obstetric complication during pregnancy, birth, or up until 42 days after birth (WHO, 2011). Maternal near-misses likely occur 5–10 times more frequently than maternal deaths (Juma et al., 2021). Moreover, maternal near-misses often require intensive care and resources which can lead to catastrophic expenditures for near-miss survivors (Juma et al., 2021). This is especially significant in low-resource settings where the prevalence of the maternal near-miss ratio is considerable (Abdollahpour et al., 2019). In Haiti, many women with maternal complications never reach health facilities which likely contributes to underreporting of maternal deaths and adverse outcomes (Bridwell et al., 2019), including maternal near-misses.
Youth make up 21% of Haiti’s population (IndexMundi, 2019) of 11.6 million (World Bank, 2023). Adolescents and youth (by United Nations, 2019, definition: adolescents: age 10–19 and youth: age 15–24) in Haiti face poor health outcomes, especially young women who make up approximately half of the youth population (IndexMundi, 2020). One of the four leading causes of death for those 20–24 years old is pregnancy- or childbirth-related (PAHO, 2017). In Haiti, maternal health and well-being of young women are especially tenuous. Systematic tracking of quantitative maternal youth indicators has begun, but an important gap remains in existing knowledge that links youth perspectives and lived experiences of maternal health and well-being within their communities (UNICEF, 2016). Youth perspectives are important to include in the development of a response aimed at helping to curb maternal deaths and maternal near-misses among young women within settings of constrained services and low resources. This is because engaged youth have an important part to play in initiatives with real-world implications, especially those that concern their sexual and reproductive health and well-being (Wood & Hendricks, 2017).
This study aims to help fill a gap in understanding maternal near-miss experiences from the perspective of youth aged 15–24 years. Our research questions aimed to explore the experiences and attitudes of a group of young women living in La Pointe, Haiti, and its surrounding rural communities, who had survived maternal near-misses. We were guided by the following research questions: What are the lived experiences of this group of young people who had survived maternal near-misses in northwest Haiti? What key challenges do they experience regarding their maternal near-misses? What possibilities do they see for change for maternal health in Haiti?
Background
The historical and contextual background within which this study took place is highly relevant to the research. Haiti’s colonial history, its current health system, and religious affiliations are related in the following paragraphs.
Colonization
In the 17th century, France colonized and exploited the western third of the Island of Hispaniola, that is, Haiti, becoming one of the wealthiest colonies in the Caribbean on the backs of the forced labor of African slaves (Central Intelligence Agency, 2025). Haiti’s enslaved peoples revolted and brought an end to colonial rule in 1804, establishing the world’s first independent nation led by former slaves (Central Intelligence Agency, 2025). France forced upon Haiti an indemnity (equivalent to $22 billion USD in 2023) as an independence debt (Oosterlinck, 2022; Central Intelligence Agency, 2025). This “debt of dishonor” has contributed to institutional and policy failures, resulting in Haiti’s development being stunted even into current times (Oosterlinck, 2022).
Health System
The health system in Haiti includes both public and private sectors. The current general government health expenditure is 3.48% of the Gross Domestic Product which represents a decrease since 2020, in a population whose growth is increasing at a rate of 1.2% (WHO, 2025). Haiti’s political, economic, social, environmental, and health context continues to be very precarious (PAHO, 2024), negatively impacting the health and well-being of Haitians at large. The health system is challenged to provide comprehensive health services (Fene et al., 2020); and currently 43% of healthcare is being paid as “out-of-pocket” by Haitians (PAHO, 2025). Where maternal health is concerned, the healthcare system is more fragile than ever—the MMR remains at a very high level and shows an upward trend in maternal deaths (PAHO, 2024) within a context of unmet needs for contraception (PAHO, 2025) and framed within circumstances of acute food insecurity and increasing gender-based violence especially against women and girls (UN, 2024).
Religious Affiliations
Colonization also influenced religious affiliations in Haiti which are predominantly to Christian faiths, with 55% of the population as Catholic, 29% Protestant, and the remaining affiliations being 2.1% Voudou, 4.6% Other, and 10% None (Central Intelligence Agency, 2025). Notably, in Haitian culture and society, 50%–80% of Haitians incorporate some aspects of Voudou religious practices in addition to another religion or faith (Central Intelligence Agency, 2025). Where maternal health and well-being is concerned, birthing people served by traditional birth attendants (TBAs) receive physical and emotional support, as well as spiritual support (e.g., prayers and use of religious rites) which is profoundly connected to cultural traditions around birth (Raymondville et al., 2020). It is also not uncommon for pregnant, birthing, and postpartum folk to seek guidance and care from local healers and Voudou doctors (MacDonald et al., 2018).
Author Voice
The authors represent a diverse set of intersecting identities and lived experiences which have influenced our perspectives, approaches to this inquiry, and the voice we use. Seven of the twelve authors are Black Caribbean or African, and the remaining identify as white. We are women and men. We have ties to different nations (i.e., Haiti, Canada, and Cameroon), languages (e.g., Creole, French, and English), and cultures. Our research and work span global health, midwifery, obstetrics, nursing, epidemiology, social work, and mental health. Health equity is at the root of all of our work. We aim to redress historical and social exclusion of those most impacted by health and social issues, through a lens that examines the intersection of gender, race, and the impacts of colonization. We are united by a shared desire to build relationships of trust within our work and research, to engage with and commit to communities in authentic and sustainable ways, and to advance social change through our own work and by impacting the work of other researchers and individuals working for health and well-being.
Methods
The Photovoice design of our study is detailed in the published protocol (MacDonald et al., 2024) and described below in brief. In this study, the term “women” embraces an inclusive approach to all women and gender-expansive individuals across a diversity of experiences, and acknowledges the impacts of gender on lived experiences (Tannenbaum et al., 2016).
Study Objectives
The overarching objective of this study was to understand and amplify the voices of Haitian youth who had experienced maternal near-misses. There were three primary objectives. The first was to identify, explain, and characterize factors in the social environment that created barriers to youth maternal health and well-being, and increase or influence their risk of maternal near-misses as youth. The second was to support youth leadership and empower youth to share their experiences and observations regarding maternal health and well-being in their community. The third was to mobilize findings to meaningful partners and interested collaborators to advocate for improved maternal health and well-being among young people.
Our Community-Based Research Approach
The philosophical foundations of this study are rooted in a transformative worldview and community-based participatory research (CBPR), through a lens of health equity, social justice, and sustainable community development (Creswell & Plano Clark, 2018). Reflecting these values, our community research team is a partnership between “on the ground” Haitian community members (obstetrician-gynecologist, nurse, Community Health Lead affiliated with Centre Médical Béraca (CMB), and two youth engaged in community health and wellness) and team members in Canada (Canadian midwife and PhD student, and Haitian Canadian nurse-midwife). This core research team is made up of members with affiliations to CMB (Centre Médical Béraca, 2019) and the communities it serves, working to better health and well-being for the communities’ women, especially young women. Members have strong ties by way of currently working, living, and being active members of these communities, or through previous work, long-term volunteer, research, and living experiences in this community and in other parts of Haiti facing similar maternal health challenges. Our team strived to approach our work from feminist and anticolonial perspectives, and to center the knowledge and expertise of local Haitian community members and young women with lived experiences.
A critical feminist and anticolonial theoretical framework was adopted that attempted to make visible the historical and present day social and political conditions in Haiti, where maternal death and near-misses continue to occur at an alarming rate and with substantive impact on women, their families, and the community at large. In theory, critical feminism makes efforts to address oppression in various forms such as between race, class, and gender, with goals of liberation, emancipation, and empowerment of marginalized social groups and the oppressed (Katsiampoura, 2024). Principles of decolonized research challenge Western research foundations, critique existing power structures, and center and engage the communities they work in through their research (Stevens-Uninsky et al., 2024). Postcolonial feminist theory recognizes women’s oppression through colonialism, nationalism, fundamentalism, patriarchies, and global economic structures (Deepak, 2012). This theory draws attention to the complexities of power relations within and between macro systems (e.g., large systemic issues, such as those in healthcare), meso systems (e.g., medium systems of communities and neighborhoods), and micro systems (e.g., contained systems of individuals and their relationships), focuses on concepts of self-determination and social justice, and affirms women’s agency, power, and resistance (Deepak, 2012). Within our work, this lens of overlapping perspectives supports consideration of gendered, racist, and colonial histories and how these histories are embedded in current maternal health practices and policies. This theoretical framing informed our CBPR approach involving Haitian young women and employing Photovoice with youth in their community.
Recruitment
Information was distributed through community-based networks, aided by community health workers and local TBAs, called “matwon” in Haitian Creole. Recruitment involved two groups of participants: those whose maternal near-miss occurred in a health facility (Group A) and those whose maternal near-miss occurred “at home” (Group B). Participants without access to a cell phone with built-in camera were provided one for project use. Study participants were 17 women-identified individuals whose age ranged from 18 to 24 years (mean = 21.4). Participants experienced their maternal near-miss between the ages of 16–23 years (mean = 18.5). Ten (59%) participants had a maternal near-miss in a health facility. Seven (41%) experienced their maternal near-miss at home and did not attend a health facility. Participant demographics are summarized in Table 1 (online supplemental material).
Data Collection
Data were collected between July and October 2023, in the Northwest department of Haiti. This region is served by two public government-run hospitals, and by CMB, the only private, health facility in this part of Haiti that operates 24/7 and that has comprehensive emergency obstetric and newborn care services (CMB, 2019). CMB serves a population of over 700,000 and is in La Pointe, Haiti (CMB, 2019). Most in-person activities were held on the CMB campus while some interviews were conducted at a nearby location.
Participants filled out a questionnaire, before and after participating in the Photovoice project. The purpose of the questionnaire was to collect participant demographics, participant questions about the project, and participants’ rating of their Photovoice experience. The focus of this paper is the data that were generated through the Photovoice activities.
Methodology: Photovoice
Photovoice is an arts-based visual research methodology, developed by Wang and Burris, that has the potential to foster social change and achieve empowerment of individuals and communities so their voices can be heard (Budig et al., 2018; Wang & Burris, 1997). Reflecting our CBPR approach, our Photovoice process leaned on feminist principles of fostering empowerment and liberation (Wang & Burris, 1994) in that our study was exclusively facilitated by women team members inclusive of women youth. The Photovoice process (Wang & Burris, 1997) and activities were adapted to the local context and participant circumstances. This included holding a project information session prior to study recruitment and supporting a flexible project timeline to accommodate participants’ multiple priorities. Our Photovoice activities occurred over a 13-week period where participants engaged in photo taking, sharing of photos, and photo elicitation during individual interviews and in a group setting. The process culminated in a participatory analysis activity and group planning for a photo exhibit. The process is outlined in Table 2 (online supplemental material).
Photovoice Process
Our Photovoice process consisted of individual interviews with all participants and two focus group discussions (FGDs) based on participant location of their maternal near-miss event. During these activities, to simulate reflection we asked questions such as “What does this photo mean to you?” (Aboulkacem et al., 2021, p. 879). Our FGD guide incorporated Wallerstein and Bernstein’s (1988) “SHOWED” method. The FGDs allowed for collective interpretation of their photos, shared interpretation of their personal lived experiences, and co-construction of the meaning of these (Liebenberg, 2018). We asked these guiding questions for the explication of each shared photo: What do you See here? What is really Happening here? How does this relate to Our lives? Why does this situation, concern, or strength exist? How can we become Empowered through our new understanding? What can we Do about it? (Wang et al., 1998)
Interviews occurred in weeks 3–7, with the average time of the 17 interviews lasting 10.5 minutes. FGDs occurred in weeks 9–11, and lasted 67 minutes for Group A and 78 minutes for Group B. All sessions took place in Creole, were recorded, and transcribed verbatim. Each participant took 1–8 photos, for a total of 55 photos; participants shared 50 of their photos for public display. Findings of photographic data are summarized in Table 3 (online supplemental material).
Data Analysis
Our community research team participated in a process of data analysis which included iterative discussions following interviews and focus groups; analysis sessions using Creole audios and transcripts, and photos, then English translated transcripts; computer-assisted analysis of English transcripts using NVivoTM, group interpretation sessions, and a mapping process of major themes; and finally, a discussion and review of themes. Findings were viewed by keeping in mind a maternal mortality framework of determinants, contributors, and causes of maternal death (Souza et al., 2024).
We adopted Braun and Clarke’s reflexive thematic analysis (Braun & Clarke, 2019) as our method of data analysis to include the following steps: Data familiarization and writing familiarization notes, coding data systematically, generating initial themes from coded and collated data, developing and reviewing themes, refining, defining, and naming them, and writing the report (Braun & Clarke, 2021).
A critical component of reflexive thematic analysis is ensuring that
Ethical Considerations and Participant Protections
All study procedures were reviewed and approved before the study began. The community research team reiterated concepts of informed consent, study withdrawal, and confidentiality with participants. Only participants who provided their informed written or marked and ongoing consent to participate were included in the study. Study activities took place at an appropriate time, in a safe location, with the provision of food and drink, and availability of childcare. We addressed ethical issues raised by the use of Photovoice and ensured we exceeded Wang and Redwood-Jones’ minimum best practices of Photovoice ethics (Wang & Redwood-Jones, 2001). Participants submitted a media public release form providing permission for public display of their photographs. Participants collected a signed or marked public release from community individuals who were featured in photographs. Reported findings and photos for public display will use participant numbers or pseudonyms (as used throughout this paper). We compensated participants $10 USD per participant for each study activity, and paid transportation costs to activities. At the project’s end, each participant received a certificate of appreciation, copies of their photos, and a gift of healthcare supplies.
Given the sensitive and traumatic nature of the research topic, it was our responsibility to ensure optimal ethical care and concern for participants (and for research team members) for which several measures were put in place. First, we addressed any ethical concerns and attempted to mitigate them through open and ongoing communication, with direction from those engaged within the project (especially local team members and participants themselves), community players, and partner organizations. For example, we sought specific ways to protect the privacy and security of participants (e.g., by location of interviews and optimal daylight time for activities). Second, team members facilitating participant interviews and group discussions undertook additional training around the ethical and empathetic care of the young women participants. These women team members included a local, experienced maternal healthcare nurse with skills in interviewing and provision of empathetic care, and two youth research coordinators with community involvement among youth and children but no formal skills in healthcare provision or research. Their training integrated WHO-recommended guidelines for the ethical and safe conduct of intervention research on domestic violence against women (WHO, 2016) and used a trauma- and violence-informed approach, emphasizing ethical attention around participant safety (Nonomura et al., 2020). During training sessions, we brainstormed about different ethical concerns, and potential scenarios and narratives that could arise during interactions with participants, and how these could be broached; we collaborated on how to navigate our roles and responsibilities as researchers, especially when discussing sensitive topics among marginalized groups. Third, for participants, we ensured access to appropriate medical and mental health referral through resources at the local healthcare facility and with other available community supports. Our efforts were focused on ensuring the physical, social, and psychological well-being of our youth participants was not adversely affected by their participation, and promoting participants’ agency, well-being, equity, and dignity (Nonomura et al., 2020). Finally, we checkedin regularly and supported team members, particularly the youth research coordinators, in their roles while being immersed in participants’ narratives.
Global Research Ethics and Inclusion
This work adheres to the TRUST Code, a global code of conduct for equitable research partnerships (TRUST, 2018). Our research has local relevance, was designed and conducted in partnership with local communities, received local ethics approval, took measures to ensure participant safety and well-being, tailored activities, documents, etc., to local requirements, and upheld the highest possible ethical standards.
Findings
We present five themes resulting from our reflexive thematic analysis of participant photos and narratives. These findings emerged from both the participants’ group analysis and the team’s analysis of these data. Each of the authors immersed in this project (through workshops, interviews, and discussion groups with participants, during community research team meetings, and while pouring over the transcripts, etc.) were deeply touched and profoundly impacted by the young women participants themselves and the experiences they shared.
Theme 1: “Starting From the Margins”
Youth participants described living in rural, low-income, resource-constrained communities and the implications of poverty that permeated all aspects of their lives. The social context of pregnancy, childbirth, and parenthood represented further challenges for young women, an already marginalized group. Challenges related to the importance of attending antenatal care visits, “taking care of themselves” including their mental health, receiving medical care, preparing for parenthood, and eating nutritious food during pregnancy, for example. Using humor, Sasifi, a 24-year-old, referred to the importance of a healthy diet. Sasifi stated: Like … I wish for them [youth], to give them a little advice: when they are pregnant, not to eat “weak” food, not use poor food, it won’t give you much, right. It’s eating strong things, that we should use, so we can build our body, like water in a pot; when they tell you [to put] water in a pot, it’s not just water in the pot!!! To the little bit of water in the pot, you need to add something [nutritionally] strong to give you strength to help your baby. It will be good for us, it can help us … (Sasifi, FGD-A)
Social and financial precarity for these youth necessitated important ties to their parents. Regardless of whether they had a partner, many participants described how they needed to rely on their parents for shelter, food, and funds for transportation and basic healthcare needs. Fany, a 24-year-old, explained that having children too early (i.e., as youth) led to reliance, particularly on their parents. Referring to youth as “children,” Fany felt as though “children shouldn’t have children early” because they lack financial means to be parents. She further elaborated: The person you’re having a baby with doesn’t have the means, you also can’t afford it, you’re under the roof of adults, they are the ones who will help you. (Fany, FGD-B)
Participants also reflected on sociocultural values and stigma related to pregnant youth and schooling. One participant, 22-year-old Sara, equated adolescent pregnancy to lack of education saying “… because we don’t go to school, we have children too early” (Sara, FGD-A). Other youth shared that pregnancy often signaled an end to their education. In some communities, for example, adolescent pregnancy is perceived as shameful, and pregnant students are not accepted at school. A pregnant youth can be rejected by peers, abandoned by faith members, and isolated from the community. A culture of exiting school upon pregnancy was identified by the youth as a barrier to gaining future work, earning power, and financial independence. Some participants suggested the need for a cultural or policy shift. Dylane, a 19-year-old, for example, recommended that youth should return to school “to learn a trade,” to be able to earn money and establish themselves independently.
Finally, young women described their circumstances of having low education, lacking maternal health knowledge, suffering from existing health conditions, living in poverty, and confronting multiple barriers to care access. For example, while participants supported the idea of giving birth in a health facility, the reality was that many participants birthed at home because of distance to a health facility, transportation and socioeconomic issues, and preference for a matwon as birth attendant. The matwon in this Haitian context is an individual with a close relationship with their community, is recognized for their indigenous knowledge and skills in caring for women and their babies, and provides culturally acceptable services to pregnant folks and their families in communities which often lack access to medical care and are resource-limited (Jean-Baptiste et al., 2023). Youth shared many photographs of everyday items (e.g., bed and inverted bucket with a blanket) used to cope during childbirth at home. For instance, Sasifi, a youth from a remote community, photographed a “biyòt,” Creole for a kind of birthing stool (Figure 1). Sasifi described the object in detail: shaped from a chunk of wood, brought by the matwon or handed down in families, and used to help reduce labor pain. Eva, a 23-year-old participant from an urban area, recognized the biyòt as a necessity in remote communities, where it is difficult for women to get to a hospital, and its use helped them in some way. Photo by Sasifi: “Biyòt” (birthing stool).
Overall, the disadvantaged positions of youth at the margins contextualized the difficult choices youth needed to make, and shed light on how their choices further affected them throughout their maternal trajectories.
Theme 2: “Negotiating Hostile Terrain”
Participants described how structural, systemic, and political forces were dangerous roadblocks that influenced their pregnancy journey and beyond. Youth spoke at length about the lack of road infrastructure particularly to remote communities. The problem of inadequate roads was captured by Melanie, an 18-year-old participant, in a photo showing the community road used to reach hospital (Figure 2). Photo by Melanie.
Youth described the impact of Haiti’s political unrest (i.e., their “state” or nation’s lack of an organized, functioning, and effective government) on availability of gasoline and access to transportation. The complexity of issues presented barriers to getting to a health facility and to be followed by a doctor if there even was a health facility in their area. Sonia, 24 years old, described her efforts to advocate for change: I am asking the authorities to put hospitals in the remote areas … if there were no hospitals in the area, to put an ambulance, so that when the person is in pain, so that they can reach [a hospital], because the moto is not too good for the person, because if the baby’s head comes out, it can cause problems for the baby. (Sonia, FGD-A)
Contextual realities created further adverse and unjust conditions for their journey when danger signs signaled the important need for youth to leave home and seek medical care. First, in situations where there may be a health facility in one’s area, the youth stated that paying for transportation or healthcare was not possible since as young people they “don’t have work” and could not save money for their current needs or those as future parents. Second, for youth who were able to find the means to give birth in a health facility, they faced challenges all along their way, including impassable roads, long journeys on foot, by donkey (Figure 3), or carried on a door (Figure 4), delayed travel during darkness, inherent risks of motorcycle transportation because of a reckless disregard of moto drivers for their passengers, and motorcycle mechanical breakdowns that added time and urgency in reaching their destination. “This donkey represents for me … when I was giving birth, it was the one who carried me when I was in pain, when things were hurting me, I couldn't find anything else so I could go [to hospital].” (Melanie, Interview) Photo by Dada: “Lè m te ansent” (When I was pregnant).

Irene, for instance, shared a photo of her brother’s mobilette and explained what it meant to her (Figure 5). For Irene, the memory of being transported on the same mobilette while unconscious and having eclamptic seizures evoked sadness and pain. Irene related: If the country had a state, it was not the motorcycle that was supposed to take me, because of the way I was, that was supposed to take me to the hospital. I think it was in the ambulance that I would have gone to the hospital. (Irene, FGD-B) “When I was... when I was going to have the baby, I was... I had eclampsia (seizure attack). That‘s the motorcycle... when I... when I was at home, I was at home, and I was inside, something came over me and they called the motorcycle to come and take me to the hospital.” (Irene, FGD-B)
Having finally reached a health facility, youth faced additional structural barriers—a hospital without access to emergency obstetric care, or worse, without medical personnel. This context is described by Adelrose, a 21-year-old youth, whose experience included a series of roadblocks during her labor, first with no available matwon in her remote community and then with “no means of transportation,” being carried on a door, before finally reaching a health facility. As Adelrose explained: When I was going to the hospital, it was a Sunday and there was no nurse. There was not one nurse in the hospital, so it was time to call them and they called them [at] home, they came, when they came to see me … they finished writing a file about me, then they made me walk, they made me walk, they made me walk for a long time and then they admitted me. (Adelrose, interview)
Similar systemic challenges persisted into the postpartum period, negatively influencing health seeking behavior and overall maternal and neonatal health and well-being. Several young women shared stories of their survival during birth that were juxtaposed with the losses of their infants born still or dying at a few months of age. Participants were empathetic of their peers and voiced concerns about lack of care. For example, Sara noted the injustices of the structural context and their impact on Fany, now 24 years old, whose circumstances prevented her from receiving specialized care and led to grave consequences. Sara explained: What happened is that each child she [Fany] had, all three of them died. It is because our country does not have a state [it is ungoverned]. If our country had a state, every child that’s born, you’re not supposed to have to bury them at your place. She is supposed to bury them in the cemetery. Also, if every child she delivers dies, she is supposed to go to a big hospital. (Sara, FGD-B)
Youth who survived their maternal trajectories were survivors of complex and pervasive structural, systemic, and political forces. These forces, beyond their control, had a profound and negative influence on their individual outcomes.
Theme 3: “Pathways of Pain and Suffering”
Youth were keenly aware of the impact that their circumstances could have on their health during their maternal journey. Participants shared disturbing, brutal, and traumatic experiences of pain and suffering because their experiences of poverty prevented them from being able to eat well, gain maternal health knowledge, receive effective treatment of health conditions, and seek care in a timely manner or at all. Melanie experienced grave complications during her pregnancy. Melanie shared an all-black photo to represent her difficult journey to reach help, losing consciousness along the way (Figure 6). Unaware of what was happening to her, she explained “… when things were hurting me, I didn’t know anything else, I saw darkness.” Interestingly, another participant, Monette, felt that the context of the photo was representative of more broad challenges faced by youth. Monette explained: Sometimes when a young girl is pregnant, she has difficulties, everything is against her. Like she can’t go the hospital, she doesn’t have a family that is there with her, this means that she sees everything black for herself. It is one of the reasons that [people] are always opposed when a young woman is pregnant … people may not stand up for her, but she would prefer that someone stands with her to give her good advice, so she doesn’t just do “whatever” with this baby in her belly. (Monette, FGD-A) Photo by Melanie: “Peryòd lavi m te nwa” (Dark period of my life).
Youth described their experiences of pain and suffering at a health facility in ways different to care provided at home. Particularly within the context of medical interventions, several participants described being uninformed by hospital personnel. Youth echoed “not knowing anything” about their care and not being told about the immediate well-being of their baby, for example. Young women also related to the lack of dignity they experienced when being physically examined, especially by male doctors. Eva provided cultural context for youth’s preference for home birth yet also gave a rationale for the importance of skilled birth attendance. She articulated that young women don’t like to go to the hospital to give birth, explaining: … so the doctor doesn’t see their private parts. Some girls say that they don’t want to open the feet [part their legs] in this way, they don’t want to. But for this problem, we want it to improve, for the youth to think differently. Because giving birth in a hospital is the best way, you will also get better care, and for the baby to be healthy. (Eva, FGD-A)
Most participants described recovering from their painful experiences of pregnancy and childbirth. However, for some young women, pain, suffering, and loss continued and became embodied within the postpartum period. For example, 19-year-old Marianne was abandoned by her partner and living in extreme poverty. Among all study participants, only Marianne described the unassisted birth of her child at home, save for the help of two family members. She also share an all-black photo. Marianne explained how the photo symbolized her experience when she could cope no longer, lost consciousness, and unaware delivered her baby in her yard. Marianne could not “… place him in his bed” but rather he was buried in the yard on the day of his birth. Next, in the postpartum period, Marianne was plagued by dizziness, “zombies dancing” in her head, and an (untreated) uncharacteristic sense of loss of self-control. Marianne’s narrative and photo led to discussion among participants and another interpretation of the photo’s symbolism. One participant felt the photo represented “Darkness … like someone died somehow …” as if the photo was an expression of Marianne’s emotional pain and trauma turned to mental anguish and suffering.
Finally, Fany described already suffering the immeasurable pain of losing her first two babies, and then shared the experience of her last birth: The third baby, I delivered him, despite me having a lot of suffering, I delivered him. … After that, he was living, despite the difficulties, every time he was sick, I went to the hospital with him, until when he was six months old, he died. (Fany, FGD-B)
Fany shared a photo of a machete (Figure 7) as a symbol of her loss and anguish, describing it in this way: That machete, it’s the same one every time I have children, it’s the same one I take to dig a hole to put the children. (Fany, interview) “The machete is a symbol … [of] each time I had pain, I had given birth to babies, despite going through a lot of misery, I didn't succeed. It's this machete, that … it was this machete that was there for me, to dig holes to bury the babies.” (Fany, FGD-B).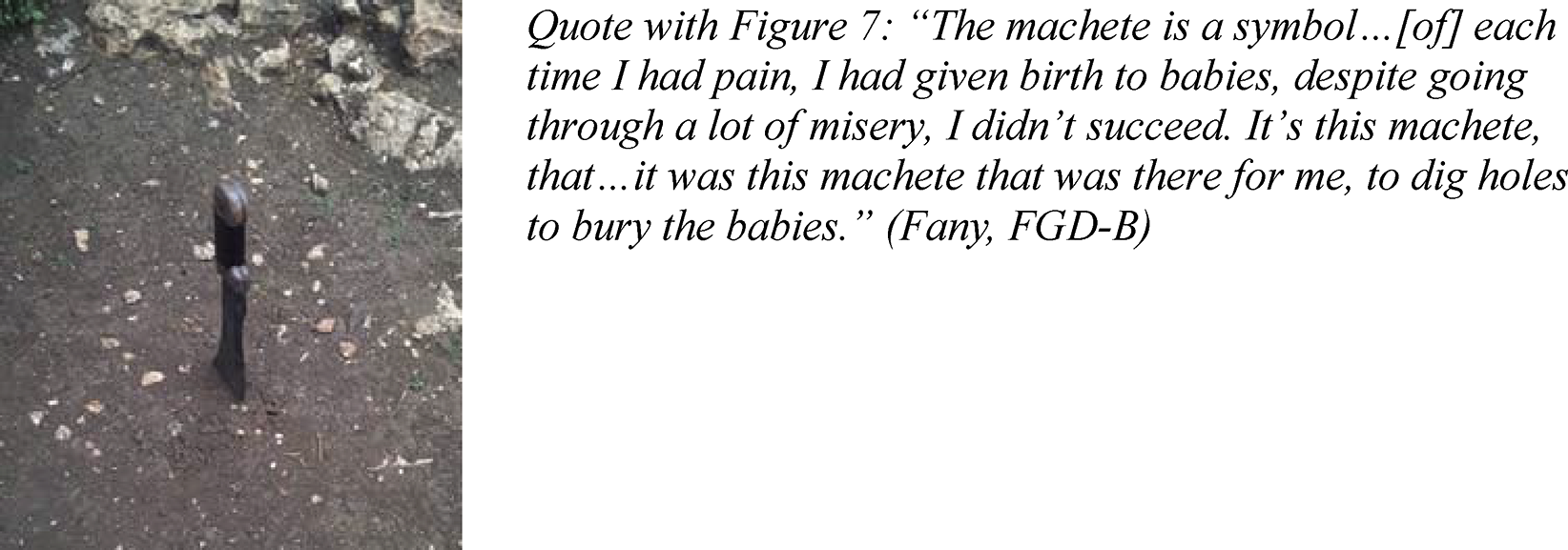
Youth suffered greatly in ways physical, emotional, mental, and spiritual during their maternal journeys.
Theme 4: “Searching for Support”
Young women sought support to combat their sense of isolation and confront pervasive obstacles faced along their entire maternal journey. Youth described positive maternal experiences of being offered money, food, and drink, being carried by community members to hospital, receiving therapeutic touch and kind words from a birth attendant, feeling cared for with dignity and respect, and being surrounded by supportive family and friends.
Marianne recounted the importance of family support when describing the precarity of her first pregnancy as a 16-year-old. Already living in poverty, in a remote community with barriers to care, her situation was exacerbated when she was “kicked out” and abandoned by her partner and came to rely solely upon her father and sister. With no financial support from her former partner, she was unable to buy adequate or nutritious food during pregnancy. She was only able to attend one antenatal care visit and could not afford the additional costs of completing pregnancy investigations ordered by the doctor.
However, while participants described family was a potential source of support, living “under the roof of adults” also had implications for youth with respect to their agency and autonomy since parents held the balance of power. Eva described family dynamics and treatment of pregnant teenagers. She explained that parents will often “kick out” their pregnant youth from the family home. If the young person remains at home, parents “will pressure her” and speak to the youth in a negative way, “increasing stress” such that the young person “will become malnourished.” Eva had clear advice for parents to support pregnant youth: The advice I’m giving is not for the young, I’m giving it to the parents [of pregnant youth] … I hope that parents modernize about things, so that they don’t tell young people some things that will traumatize them during their pregnancy. (Eva, FGD-A)
Participants talked extensively about the importance of having supportive people “at their side” especially during childbirth. Yola, a 23-year-old, highlighted emotional and physical support first, from her partner, and later a friend by her side to bear the weight of her pain. Yola stated, “She was the one who took the most pain with me.” Youth also related to the important presence of their matwon to help them. They shared how their trusted matwon attended to them, offered hands-on care, and provided spiritual support. Dylane described her matwon-attended birth: When I couldn’t take it any longer, my mother went to call a matwon. When the matwon came, she checked me … Every time she made me push, I became unable to push, I lost strength. Now, they went to buy a juice for me which I drank, after she checked me again, she said I was almost delivered … [but] I didn’t have room to delivery him … she checked me, she was also a Christian, she prayed for me and then my passage opened, I gave birth. (Dylane, FGD-B)
Their matwon advised on labor progress and helped them through their pain. As an 18-year-old, Sara gave birth in her remote community. Sara shared a photo of her matwon and explained: … when I was giving birth to the baby, she was the one who gave me strength. I couldn’t have the baby, I couldn’t push him, she was the one who gave me the strength that made me have the baby with God’s grace. (Sara, interview)
Youth described the use of ritually important natural remedies throughout their maternal trajectories. Matwon, especially, shared indigenous knowledge of plant remedies used for different functions (e.g., to control bleeding). Lourdie, a 23-year-old, described a plant used to help give birth and stimulate placental delivery, and captured its image (Figure 8). “… I felt belly pain, after that ... the matron came to wash me, after I came and gave birth to the baby. Unfortunately, I could take 15 minutes, after, which I could not deliver [the placenta]. After that, they made ... boiled a leaf for me that they called “mother wasp”, I drank it but it was not this alone that made me give birth to the baby, no. After that, I came… the placenta came out, I came to deliver it, after that I didn't feel any problem anymore.” (Lourdie, FGD-B)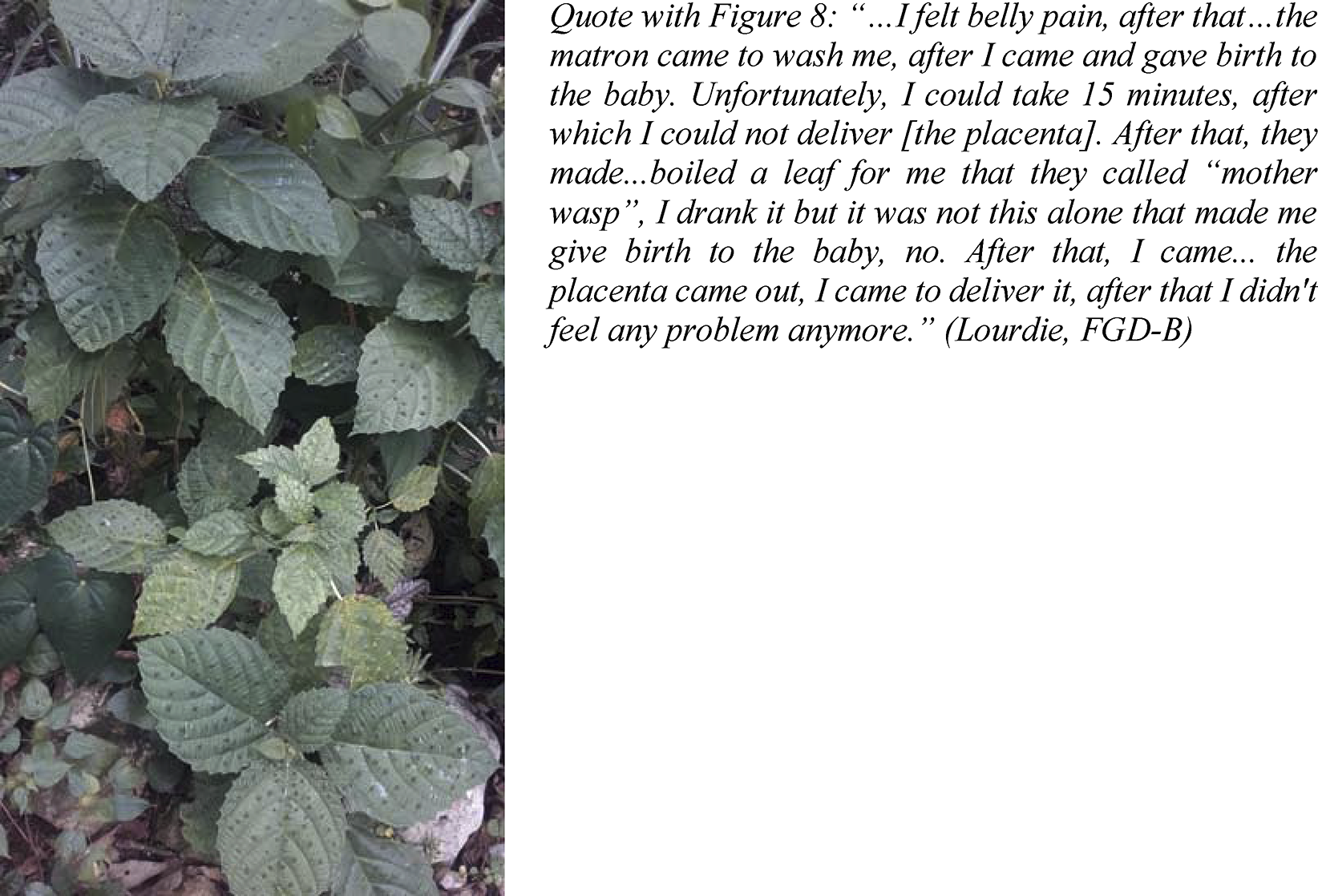
Sara also shared about her matwon’s use of an herb to facilitate birth by rubbing a gumbo (okra) leaf over Sara’s face. Sara stated: When the matwon came, after passing a small gumbo leaf, she said that I did not have space for the baby to come out, [but] she used the gumbo leaf. After that the baby was born. (Sara, FGD-B)
Finally, the safety of herbal remedies was questioned by a proportion of youth who raised concerns about maternal–fetal risks with their use. Fany saw grave risks and stated, “It shouldn’t be that you must drink boiled mother wasp leaves and give it to the woman when she’s giving birth, because it can create a problem in the baby, the baby can even die.”
Overall, supportive family, friends, and community members including TBAs and healthcare providers gave vulnerable youth the potential to combat their sense of isolation and confront pervasive obstacles they faced along their entire maternal trajectory.
Theme 5: “Reimagining Future Possibilities”
Participants imagined how things could be different. The young women made assertions of how they might reclaim power in spite of the many obstacles in their way. They suggested solutions for improved maternal health and well-being which are presented at the macro-, meso-, and micro-levels, respectively, as
Macro-Level Solutions: Demanding Change
One youth voiced her concerns and emphasized the importance of youth by stating: I would like to tell them like this, I would not want … I would not want … I would not want women to die during childbirth. Because we … for them to do everything possible, because we are the future of the country. (Dada, FGD-B)
Photovoice participants were keenly aware of Haiti’s current geopolitical crisis when they suggested solutions in the study. They described their country as having “no gasoline, no means, no development, no state, and no security.” Despite the study taking place at a critical point of uncertainty in Haiti, youth participants still demanded change for Haiti, and in ways very practical, pragmatic, and vital. Youth want to see structural and systemic change that will positively impact Haitian society at the grassroots level. For example, participants talked about the importance of and need for gasoline. This is especially relevant for rural areas without roads and where isolated communities are greatly dependent on motorcycle transportation. This was stated by Monette as: … because there is no gas in our country, because there are many … many pregnant women who die along with all their babies. Uhh, we are asking them to be able to help us with the issue of gasoline. (Monette, FGD-A)
Young women talked extensively and pragmatically about road infrastructure. They suggested that passable roads (and an ambulance service) would reduce the delay to reach a health facility and improve maternal and newborn outcomes, including reducing maternal and newborn deaths, for example. Youth articulated the vital need for easy access to health facilities to prevent individuals from having to travel by donkey, motorcycle, and car to get to a health center during a time of pain, stress, and urgency. They emphasized the urgency for government decision-makers to “take the lead” and “to find a way” to invest in health facilities in areas where there is no access to health services. Dada, an 18-year-old, felt that Haitians are not working together for a common cause to prevent problems of maternal health and well-being. Dada pleaded for “… Haitians to raise their voices, so that the Haitian state can give us strength and courage too.”
Meso-Level Solutions: Working Within Precarity and Uncertainty
In our study, youth were not voiceless. Youth participants were critically conscious and made connections between youth struggles and the sociopolitical forces affecting them and their community (Aboulkacem et al., 2021). Youth were acutely aware of their circumstances as precarious and uncertain in many ways (Figure 9). In spite of this, they gave solutions for improving maternal health and well-being in their communities. “This house is where I had all my children. Despite the rain, the wind blowing in, the dampness inside, the house leaked, but I had to stay there anyway, I looked for the old things I had left so that I could sleep there with the children.” (Fany, Interview)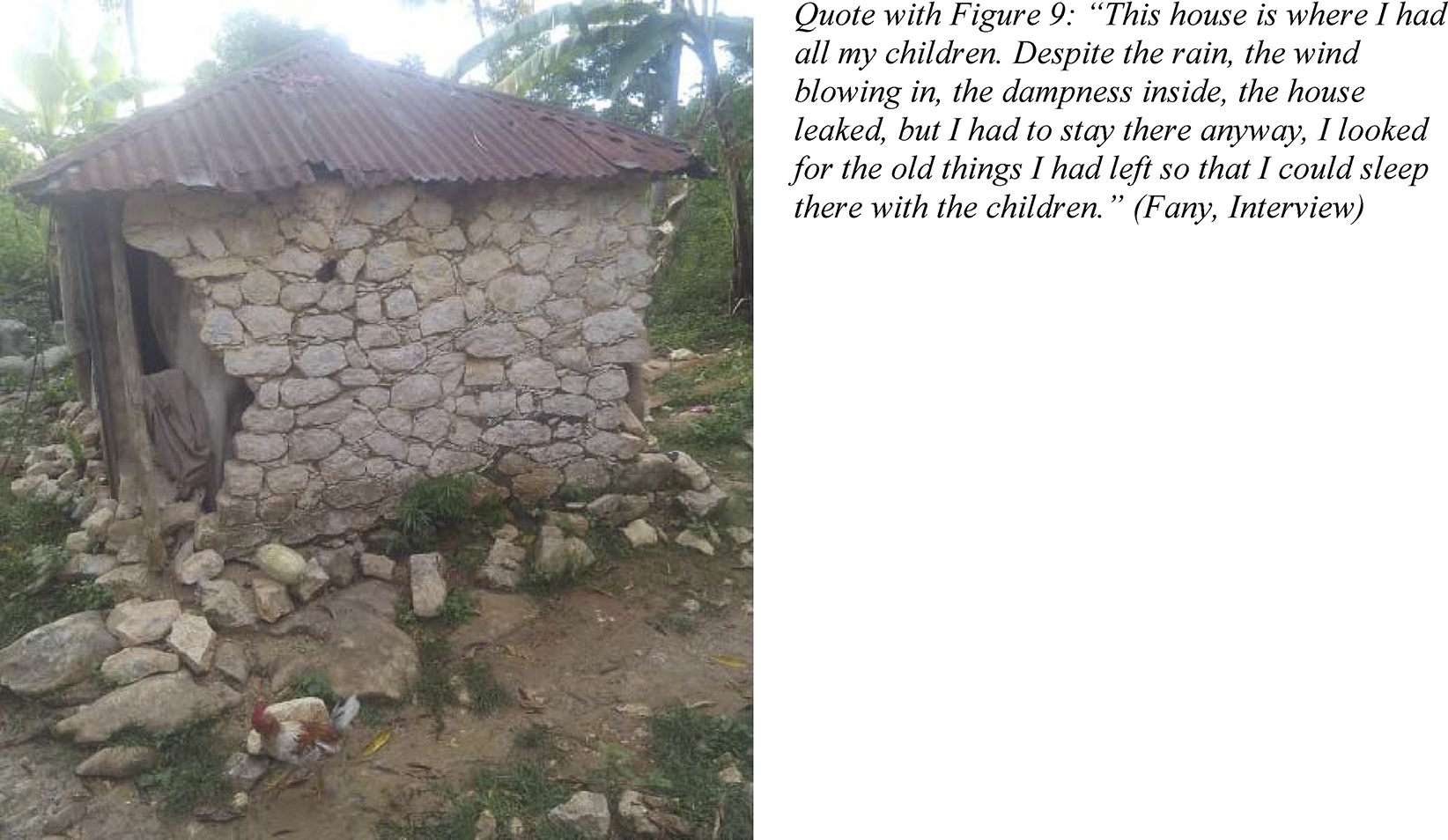
In one discussion group, youth talked about people banding together to buy a stretcher for emergency transport instead of someone “being forced” to be carried on a bed or a door. They suggested that community members could work together to build a road from their remote community. Youth also asked for more information and education to be given to young people to help with the prevention of unintended pregnancies. Dylane recommended that young people form a “girl’s group” where TBAs could teach young women about expectations for giving birth, for example.
Participants echoed a recommendation that health facilities should send trained medical personnel to provide care in isolated communities. This was seemingly in contradiction of their recognizing the value of community matwon in their communities. However, while participants at some level may have valued trained professionals whose recommendations for necessary medications and interventions were unavailable through TBAs, there were aspects of care provision in health facilities that participants did not appreciate and suffered as a result of. For example, youth focused on the gynecological bed and spoke at length about the misery it caused them. Along this discourse, several youth asked that doctors “improve the way they do deliveries.” This recommendation was made in response to the use of the gynecological bed, its contribution to labor pain in a lying position for hours on a cold, flat, and hard surface, and its causing young women to have “bad experiences in childbirth.” The young women valued the respect of their matwon and put trust in their traditional ways (e.g., use of birthing stool and delivering in an upright position). This allowed them choice of laboring position and free movement during labor and birth.
Micro-Level Solutions: Taking Things Into Our Own Hands
… the moment they [young people] find work they will become independent, then they will be able to find a means of transportation, they will be able to get a good salary to buy a vehicle, then they will be able to reach the hospital comfortably. (Eva, FGD-A)
Youth participants were able to see that in some small way “uncertainty opens space for change” (UNDP, 2022). These young women saw opportunities for change where they could actually “take things into their own hands,” as Sonia stated. Practically speaking, they emphasized that at the root of their independence is their finding paid work. Dylane explained that taking responsibility means gathering a little money, in anticipation of complications that might necessitate going to a health facility for care. Fany suggested that, as youth, they could benefit from the formation of a women’s group as a support that would “… be there with us, to be able to help us … when we have a problem, to stand with us.”
One participant, Yola, shared clear advice about pregnancy planning for youth saying that they should “… protect themselves when they are having sex, protect themselves when they are having children … don’t have children right away, use contraception.” Several participants had concerns about youth living at a distance from a hospital. They proposed that youth themselves should “raise their voices” concerning the need for more healthcare centers. They also advised that pregnant youth approaching their due date should leave home and travel closer to the hospital before labor, staying with family or friends to be nearby the health facility. Many participants explained the importance of being followed by a doctor and giving birth in a hospital and “having a good outcome.”
Youth shared a litany of other recommendations for young people. They should practice total abstinence, be careful who they choose as a partner, eat a healthy diet in pregnancy, take care of themselves physically and mentally, attend antenatal care visits, prepare for parenthood, and avoid riding motorcycles in pregnancy, to name a few. They also articulated the importance of being supported by family and friends during their maternal journey. Eva highlighted the importance of support for youth especially, and asserted: It’s best to know which people we should count on. Fight too so that we always have someone by our side who can support us in any situation. And no matter what the situation, to have someone to always talk to, to always explain what we are experiencing and what we are dealing with … (Eva, FGD-A)
These young women participants had solid knowledge of the state of maternal health as individuals, in their community, and at the level of their nation. In addition, they offered many solutions for improved maternal health and well-being relevant to their context.
Discussion
Our study captures rich visual and textual narratives of youth and illustrates in-depth insights into the complexity of their lived experiences. Together with our young women participants, we explored the phenomenon of maternal near-misses. We used a research approach aimed at redressing power imbalances by building strong community partnerships, using community-adapted research tools for data collection, and engaging community research team members as cultural navigators for this research (Stevens-Uninsky et al., 2024). However, this exploration came with certain ethical challenges, exacerbated by an unstable political context in Haiti. For example, facilitating consistent engagement of participants as co-researchers throughout the life of the project was not possible; and the shared benefits of this research among participants, community members, and researchers alike are yet to be fully realized. These examples bring into question how our study measures up to anticolonial research and how effectively we have focused on cultural relevancy and in making efforts to dismantle residual colonial power structures inherent to Western research (Stevens-Uninsky et al., 2024). Overall, our findings overlap and create a multifaceted web of interconnected and inter-related nodes (Souza et al., 2024) in the messiness and perilous journey of maternal health and well-being for these Haitian youth. We found that youth survivors of maternal near-misses living in rural northwest Haiti faced substantial challenges during their maternal trajectory. Women shared about the contexts they are embedded within, their experiences of pain and suffering, and an embodiment of the challenges of their maternal journeys.
First, we found several factors in the social environment that created barriers to youth maternal health and well-being, and influenced their risk of maternal near-misses as youth. A key finding was that accessible, affordable, and safe transportation proved difficult for both youth living semi-rurally and those living in rural and remote areas. Youth had indigenous knowledge of Thaddeus and Maine’s Three Delays Model of the three critical delays when obstetric complications can have direct consequences on maternal survival (Thaddeus & Maine, 1991). In practical terms, participants were keenly aware that a delay in the decision to seek emergency obstetric care (first delay); a delay in reaching a health facility for care (second delay); and a delay in receiving appropriate treatment at the facility (third delay) (Raymondville et al., 2020; Thaddeus & Maine, 1991) all contributed to the risk of maternal death or experiencing a maternal near-miss when there were complications of their pregnancy or birth. Youth acknowledged the importance of seeking medical care but recognized poor access to health services and its contribution to maternal death in their communities. Youth recognized the potential benefits of maternal care in health facilities but pointed out that young women avoid hospital birth for numerous reasons: cost for care, limited space (i.e., for support people), scarce resources, labor expectations that prevent ambulation, and lack of dignity during care provision. All participants shared vivid stories of pain and suffering, endured and embodied. These findings are all highly consistent with those of other recent studies in Haiti concerning perceptions of facility births (Dev et al., 2019), barriers and facilitators influencing facility births in rural Haiti (Raymondville et al., 2020), and referrals to health facilities by TBAs (Jean-Baptiste et al., 2023).
Participants in our study also made light of the value of TBAs, the community matwon. They described TBAs’ many skills and expertise and saw them as a bridge between their communities and health facilities. Yet, participants also saw a need for training and support of matwon. Both findings align with other study findings on matwon in rural Haiti (Dev et al., 2019; Jean-Baptiste et al., 2023). Next, the work of Juma et al. (2021) highlights the financial costs of maternal near-misses in under-resourced settings and demonstrates financial burden for survivors and their families. This finding has some resonance with our study. As such, for some participants, first, the cost of treating a near-miss was a barrier to seeking care. Second, youth experienced financial difficulties related to the costs of transportation, medical or traditional healer care, and treatments.
Our study also had unique findings. We found that youth were highly perceptive of the impact of maternal near-miss survival on their physical, emotional, mental, and spiritual health and well-being. Youth were reflexive about their lived experiences and related easily and with empathy to the circumstances of their peers. They depicted their experiences as painful, filled with misery and suffering, and even traumatic. Their pain and suffering was brutal, pervasive, overlooked, and to a degree accepted, probably due to the context of their circumstances and lives. Trauma was equated to the embodiment of a compilation of grave difficulties in their maternal trajectories. The actions of unsupportive individuals contributed to their trauma and created another barrier to youth health and well-being. In sharp contrast, the youth expressed gratitude for the supportive care (physical, emotional, spiritual, even financial) from their parents, partners, friends, and matwon. Supportive care seems to have been a protective factor for these youth.
Despite their circumstances, youth in this study could see ways to improve maternal outcomes. This aligned with our second study objective of supporting youth leadership and empowering youth to share their experiences and observations regarding maternal health and well-being in their community. Their shared lived experiences informed the ways they see for improving circumstances around young women’s health and well-being in Haitian society. Youth were pragmatic about the realities of pregnancy and childbirth in Haiti. Youth have called on the Republic of Haiti, decision-makers and leaders at the state and the community levels, and the people close to them to “put their heads together” to bring about real change for youth. Their recommendations range from systemic and structural changes that will take a significant amount of effort, finances and political will, to recommendations of practical and pragmatic grassroots interventions that are feasible, realistic, and imply elements of sustainability and responsibility, empowerment, and independence of youth themselves. Their solutions at the individual level relate to being employed, gaining independence, understanding more about their bodies including abnormal maternal conditions, being empowered, and having agency to make decisions about their health and well-being. In very direct and simple terms, youth voiced their own needs beyond surviving maternity within the grand scheme of their sexual and reproductive health and well-being. In many ways, their recommendations overlap with core principles of trauma-informed care that include safety, trustworthiness and transparency, peer support, and empowerment (Center for Health Care Strategies, 2024).
In this study, we supported youth and considered them co-researchers in this work. The youth participants made suggestions to change the direction of the research methodology and methods, were intimately involved in data analysis during FGDs, and helped plan for a community Photovoice exhibit (pending community security). These participants shared more of their experiences during our end-of-project celebration and felt recognized for their contributions in this project. Regretfully, constraints of security, transportation, communication, timelines, and finances have prevented a more profound implication of youth participants as project co-researchers. Our study also supported youth leadership through a very active engagement of the two young women as research coordinators on the research team, empowering their peers to share their experiences and observations regarding maternal health and well-being in their community. The youth research coordinators have continued the conversation about youth health through their involvement with girls and young women’s groups, on a radio show, and through their experiences at university in medical school.
Our third study objective concerned knowledge mobilization efforts. To date, sharing of our findings and advocacy for improved maternal health and well-being for all women have taken place among the participants themselves, within the CMB community, through the work of a non-governmental midwifery organization working in Haiti (that supported our project), and at an international global health conference in Canada. Plans to present a community exhibit among other mobilization efforts have been delayed due to geopolitical instability and insecurity in Haiti.
Finally, youth managed to survive grave maternal experiences, but we are left with questions such as “at what cost, and with what impact on their future lives?” and “how have their experiences been embodied and to what affect?” Through the individual and collective narratives of these youth, we are drawn to further consider concepts of agency and autonomy for them as young women, as they relate to their maternal health and more broadly, their sexual and reproductive health and well-being. This includes stigma surrounding young people’s sexual and reproductive health which was also reflected in our findings (Hall et al., 2018; Nyblade et al., 2017). Evidently, we are reminded that maternal health and well-being is a messy, complex social concept. This is eloquently stated by Souza et al.: “Maternal health is a social issue: maternal ill-health and disability are not just medical problems, but outcomes of a complex interplay of eco-social forces, lifestyles and exposures, and individual-level factors” (Souza et al., 2024, p. e307).
Implications and Future Directions
This study provides important foundational data about the value of engaging and elevating the voice of youth, and a participatory approach to advance system change that is relevant and responsive to their needs. Future directions in research should consider participatory methods to involve youth in other sexual and reproductive health research approaches, including research partnerships with community-based youth-serving agencies that value youth participation and engage youth in all stages of community research. This should consider a more in-depth exploration of how gender constructs such as gender roles, gender identity, and institutionalized gender can help us understand near-misses, for example, and their intersection with issues of maternal morbidity and mortality.
Short-term adaptations that may lead to reduced morbidity and mortality of young women in Haiti should be considered. Given the context of a failing nation experiencing a humanitarian crisis, these could include identification of a community champion youth leader in more remote communities, and their being partnered with a health leader at the local hospital. Communication, collaboration, and capacity-building could help bridge the sharing of information, education, and health planning for community youth and others. The local hospital could bring youth leaders, parents, community matwon and other leaders, and healthcare personnel together to brainstorm other ways to promote community health and well-being. Practice could be changed by supporting TBA-training that uses a collaborative and interactive approach, instituting birthing plans that address transportation barriers, and creating a more supportive person-centered culture of maternal healthcare to address the specific needs of young women. Policy objectives can be strengthened by having youth advisory committees that support youth leadership and help inform policy-makers about youth health and well-being, from upstream policies and services to prevent unintended pregnancies among youth to improving access to and quality of healthcare services for youth.
Strengths and Limitations
We formed a research team that understood community context and the needs of youth. The team included two young women members who were central to all interactions with youth participants. The use of photos allowed participants to be co-creators of knowledge through their photos and to tell their stories. Photovoice captured an insider’s view into what otherwise might have been inaccessible. We empowered Haitian youth community research team members and study participants to be engaged in CBPR, and youth raised their voices. Recruitment of a wider breadth of participants may have been deterred by study eligibility where participants required a camera-capable cell phone to be included in the study. It is possible that other survivors of maternal near-misses from the same community or other rural Haitian communities would share different, unique lived experiences. The study was conducted in a unique temporal and political context within Haiti and therefore may be different in other settings.
Conclusions
Prominent in this study is the need to draw greater attention to the health and well-being of young women. The findings illuminate a pressing demand to address multiple, intersecting issues of maternal health and well-being for all women but by also providing a particular focus on the needs of young women. Where young women are concerned, the positive involvement of families and friends, community leaders, and decision-makers invested in youth is especially critical. The importance of youth raising their voices and being genuinely heard cannot be understated. Interventions must recognize the contexts, causes, determinants, and contributors to their lived experiences in order to make real and sustainable improvements to the health and well-being of young people who are the future of Haiti.
Supplemental Material
Supplemental Material - Navigating the Perils of Pregnancy and Childbirth Among Youth in La Pointe, Haiti: Insights Captured Through Community Photovoice Research
Supplemental Material for Navigating the Perils of Pregnancy and Childbirth Among Youth in La Pointe, Haiti: Insights Captured Through Community Photovoice Research by Tonya A. MacDonald, Marie-Carmèle Charles, Olès Dorcely, Françoise D. Volcy Bonne Anney, Medge Dona Mular, Lovenska Sylvestre, Rose Andrele Bien Aimé, Elizabeth K. Darling, Saara Greene, Sandra Moll, Carmen Logie, and Lawrence Mbuagbaw in Qualitative Health Research
Footnotes
Acknowledgments
Author Contributions
Declaration of Conflicting Interests
Funding
Ethical Statement
ORCID iD
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.