
Abstract
Keywords
Introduction
Recent studies revealed that the immune/inflammatory response may play an important role in the pathogenesis of vascular disease, since it is predisposed to platelet activation and neutrophil recruitment.1–3 Neutrophil-to-lymphocyte-ratio (NLR), platelet-to-lymphocyte-ratio (PLR) and systemic-immune-inflammation-index (SII) are novel, widely available biomarkers that provide information on immune/inflammatory status. These inexpensive tests have been proposed as useful indicators in a number of diseases in which inflammation plays a critical role, such as cancer, rheumatoid arthritis, chronic lung disease, acute coronary syndrome or COVID-19, among others.4–9
The blood cellular indices have been evaluated in various studies in the literature. In these studies, the blood cellular indices provided both clinical diagnostic and prognostic value for acute PE. However, these studies were not uniform, giving different results for different clinical conditions and different outcomes such as PE severity and mortality. 10 Some studies also reported conflicting results on their prognostic role in patients with venous thromboembolism (VTE). It is improtant to note that none of these studies evaluated the predictive value of blood cellular indices on VTE recurrence and bleeding complications. 10 Additionally, clearly defined cut-off points have not yet been established. Most of these recent studies were single-center investigations involving one or two indicators, with varying number of cases and study objectives, thereby making it difficult to reach to consensus conclusions with good clinical guidance.11–15
The RIETE (
Methods
Data Source
The rationale and methodology of the RIETE registry have been previously reported elsewhere. 16 The protocol for patient enrollment was approved by the ethics committees at the participating sites and all patients (or their healthcare proxies) provided informed consent. Consecutive patients with acute VTE confirmed by objective tests (compression ultrasonography for suspected DVT; helical computed tomography [CT]-scan, ventilation-perfusion lung scintigraphy or contrast angiography for suspected PE) were recruited. Patients were excluded if they were currently participating in a blinded therapeutic clinical trial. All patients (or their relatives) provided informed consent for participation in the registry, in accordance with the local ethics committee requirements.
Variables
The following parameters were recorded in RIETE: demographics; initial VTE presentation; clinical status including chronic heart or lung disease, recent major bleeding and other underlying conditions; risk factors for VTE; blood tests at baseline; the treatment received upon VTE diagnosis and the outcomes appearing during follow-up (at least the first 3 months). Immobilized patients were defined as non-surgical patients who had been immobilized (ie, total bed rest with or without bathroom privileges) for ≥4 days in the 2-month period prior to VTE diagnosis. Surgical patients were defined as those who had undergone an operation in the 2 months prior to VTE. Active cancer was defined as newly diagnosed cancer (less than 3 months before) or when receiving anti-neoplastic treatment of any type (ie, surgery, chemotherapy, radiotherapy, hormonal, immunotherapy, support therapy or combined therapies). Recent bleeding was defined as a major bleed less than 30 days prior to VTE. Anemia was defined as hemoglobin levels <13 g/dL for men and <12 g/dL for women. Creatinine clearance (CrCl) levels were measured according to the Cockcroft & Gault equation. Haemodynamic instability at diagnosis was defined as a systolic blood pressure (SBP) <90 mm Hg, and/or cardiac arrest. The NLR, PLR and SII were defined as neutrophil/lymphocyte, platelet/lymphocyte, and platelet x neutrophil/lymphocyte counts, respectively.
Study Design
Only patients with objectively confirmed VTE and available information on the cellular indices at baseline were considered for the current study. Neutrophil and lymphocyte counts were included into the RIETE database in January 2020. Thus, this study included patients with acute VTE recruited from January 2020 to April 2021. Major outcomes were symptomatic VTE recurrences, major bleeding and death appearing during the first 90 days of therapy. Recurrent DVT, in patients with clinical suspicion, was defined as a new non-compressible vein segment, or an increase of the vein diameter by at least 4 mm compared with the last available measurement on ultrasonography. Recurrent PE was defined as a new ventilation-perfusion mismatch on a lung scan or a new intraluminal filling defect on spiral CT of the chest. Bleeding events were classified as major if they were overt and required a transfusion of two units of blood or more, or were retroperitoneal, spinal, intracranial, or fatal.
Treatment and Follow-up
Patients were managed according to the clinical practice of each participating hospital (ie, there was no standardization of treatment). The type, dose and duration of anticoagulant therapy were recorded. After VTE diagnosis, all patients were followed up on for a minimum of 3 months, although a longer follow-up was advised whenever possible. During each visit, any sign or symptom suggesting VTE recurrences or bleeding complications were noted. Each episode of clinically suspected recurrent DVT or PE was investigated by repeat imaging studies, as appropriate. Most outcomes were classified as reported by the clinical centers. However, if staff at the coordinating center were uncertain how to classify a reported outcome, the event was reviewed by a central adjudicating committee (less than 10% of events).
Statistical Analysis
All of the calculations were performed with SPSS Statistics software (IBM). Continuous variables were compared using Student's t or Mann–Whitney U tests. Categorical variables were compared using the Chi-square and Fisher's exact tests (two-sided). In univariate analysis, relative risks and corresponding 95% confidence intervals (CI) were calculated for the major outcomes of VTE recurrences, major bleeding, and mortality. A receiver operating characteristic (ROC) curve analysis has been performed for each of the cellular indices and ratios to assess the predictive ability for the major outcomes. The optimal cutoff value of each cellular indices and ratios were assessed by calculating the corresponding area under the curves (AUC) and 95%CIs. Multivariate logistic regression analyses were performed to identify the independent predictors for each of the major outcomes. Hazard ratios (HR) and corresponding 95%CI's were calculated accordingly. The goodness-of-fit of the model was examined by the Hosmer–Leeshawn test. A p value of <0.05 was considered statistically significant.
Identification of Outliers
In both, the neutrophils and lymphocyte counts, the relative outliers are typically in the upper range. In the neutrophils we found 214 outliers, no outliers were found in the lower range, the same trend was noted in lymphocyte counts with 212 outliers in the upper range. Sixty of these patients showed concomitant outlier values in both lymphocyte and neutrophils counts. Interestingly, utilizing this analysis the outliers in the platelets were also mostly in the upper range, but were proportionally higher than the one noted in the neutrophils and lymphocytes, only two patients were found to be in the lower range. The selected outliers were further checked by the RIETE Quality control committee; however, they are not considered as the true outliers.
Results
From January 2020 to April 2021, 4487 patients with acute VTE were recruited. Of these, 2115 (47%) were women, 1956 (43%) were aged >70 years, and 715 (16%) had active cancer. Overall, 2683 patients (60%) initially presented with acute symptomatic PE (with or without concomitant DVT), 283 (6.3%) had incidental PE, 1129 (25%) had lower-limb DVT, 219 (4.9%) had upper-limb DVT, 69 (1.5%) had splanchnic vein thrombosis, 142 (3.2%) had superficial vein thrombosis and 20 (0.4%) had retinal vein thrombosis. Mean values (± standard deviation) of the cellular indices were: NLR 5.9 ± 7.1, PLR 190 ± 158 and SII 1459 ± 2028 (Table 1).
Mean Values At Baseline Of The 3 Cellular Indices, According To The Clinical Characteristics Of The Patients.

Cellular counts are expressed as values × 1000/mm3
Comparisons between patients with- versus without the variable: *p < 0.05; †p < 0.01; ‡p < 0.001.
Abbreviations: VTE, venous thromboembolism; CrCl, creatinine clearance; NLR, neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; SII, systemic immune inflammation index (neutrophils x platelets/ lymphocytes).
Baseline Characteristics
Mean NLR values were higher in men, in patients aged >70 years or weighing <70 kg, and in those with active cancer, recent immobility, chronic lung disease, diabetes, hypertension, anemia or renal insufficiency, but were lower in patients using estrogens, with unprovoked VTE, prior VTE, leg varicosities, or current smokers (Table 1). Mean PLR values were higher in patients weighing <70 kg, and in those with cancer, recent surgery, immobility, or anemia, but were lower in patients using estrogens, with unprovoked VTE, prior VTE, leg varicosities or actively smoking. Mean SII values were higher in patients weighing <70 kg, with cancer, recent surgery, immobility, anemia, or renal insufficiency, but were lower in patients using estrogens, with unprovoked VTE, prior VTE or leg varicosities.
Initial VTE Presentation
Mean NLR values were highest in patients initially presenting with PE (either symptomatic or incidental), particularly in those with tachycardia or hypoxemia, and were lowest in those with superficial vein thrombosis or retinal vein thrombosis (Table 2). Mean PLR values were also highest in patients initially presenting with PE, and lowest in patients with lower-limb DVT, superficial vein thrombosis or retinal vein thrombosis. Mean SII values were highest in patients with symptomatic PE (particularly in those with tachycardia) and lowest in patients with superficial vein thrombosis or retinal vein thrombosis.
Mean Values At Baseline Of The 3 Cellular Indices, According To The Initial Vte Presentation.

Cellular counts are expressed as values × 1000/mm3
Comparisons between patients with- versus without the variable: *p < 0.05; †p < 0.01; ‡p < 0.001.
Abbreviations: VTE, venous thromboembolism; PE, pulmonary embolism; SBP, systolic blood pressure; bpm, beats per minute; DVT, deep vein thrombosis; NLR, neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; SII, systemic immune inflammation index (neutrophils x platelets/ lymphocytes).
90-day Outcomes
During the 90-day study period, 38 patients (0.8%) developed recurrent DVT, 45 (1.0%) had recurrent PE, 152 (3.4%) suffered major bleeding and 484 (11%) died [26 confirmed fatal PE (5.4%), 26 confirmed fatal bleeding (5.4%) rest includes various factors, such as cancer, renal insufficiency, heart failure, infection, cerebral ischemia, multiorgan failure]. Mean NLR, PLR and SII values were higher in patients who bled than in those who did not, and in patients who died rather than in those who did not die during the first 90 days (Table 3). There was no difference in NLR, PLR and SII values between patients developing DVT or PE recurrences and those who did not.
Mean Values At Baseline Of The 3 Cellular Indices, According To The 90-Day Outcomes.
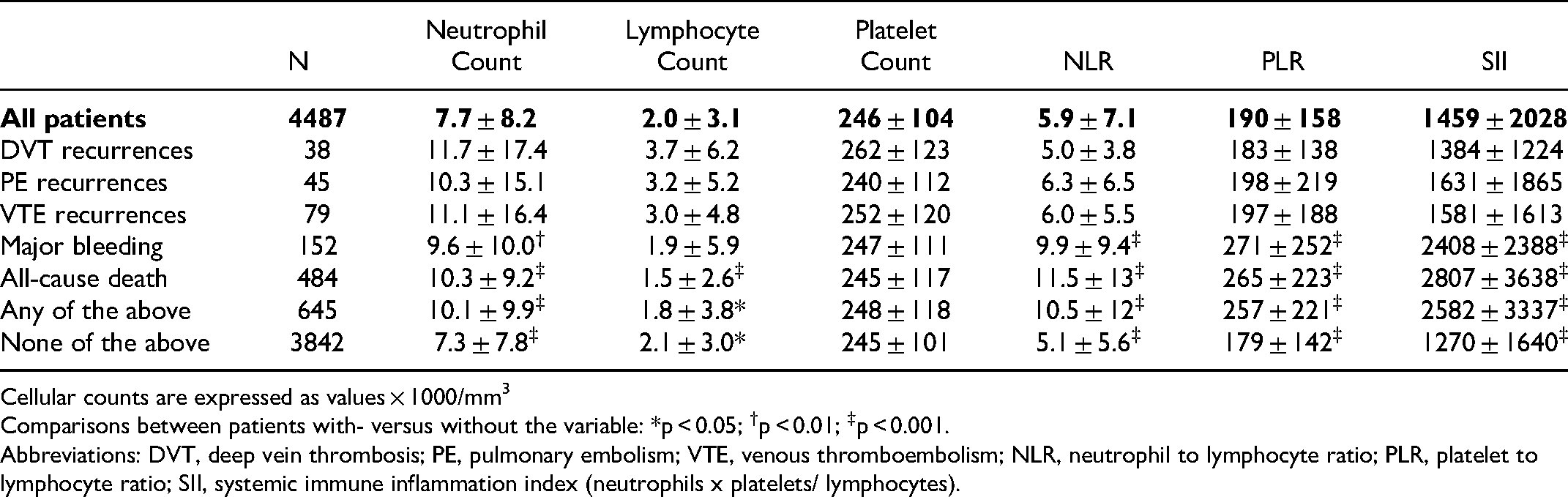
Cellular counts are expressed as values × 1000/mm3
Comparisons between patients with- versus without the variable: *p < 0.05; †p < 0.01; ‡p < 0.001.
Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism; NLR, neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; SII, systemic immune inflammation index (neutrophils x platelets/ lymphocytes).
The area under ROC curves for each of the cellular indices and their association with the risk for VTE recurrences, major bleeding or death are depicted in Figures 1–3. The optimal cutoff values of each ratio were: NLR >4.41 for major bleeding and >4.96 for mortality, PLR >166.47 for major bleeding and >167.96 for mortality, and SII >1154.81 for major bleeding and >1134.50 for mortality. No cellular indices were relevant to predict VTE recurrences (Figure 1). The overall accuracy of NLR, PLR and SII for major bleeding events by 90 days were: 0.669 (95%CI: 0.623-0.715), 0.624 (95%CI: 0.577-0.671), and 0.659 (95%CI: 0.612-0.705), respectively (Figure 2). The overall accuracy of NLR, PLR and SII for mortality events by 90 days were 0.730 (95% CI: 0.706-0.755), 0.632 (95% CI: 0.604-0.660), and 0.696 (95% CI: 0.670-0.772), respectively (Figure 3).

ROC curves of VTE recurrences for cellular indices.

ROC curve of major bleeding for cellular indices.

ROC curve of mortality for cellular indices.
Multivariable Analysis
On multivariable analysis, patients with NLR >4.41 and >4.96 were at increased risk for major bleeding (adjusted odds ratio [aOR]: 1.73; 95%CI: 1.05-2.86) and for death (aOR: 2.50; 95%CI: 1.83-3.42), but not for VTE recurrences (Table 4). Patients with PLR >167.96 and >166.47 were not at increased risk for major bleeding and mortality. Patients with SII >1134.5 were at increased risk for death (aOR: 1.52; 95%CI: 1.08-2.14) but not for VTE recurrences or major bleeding. These results are different from the univariate analysis where all three indices demonstrated an association with major bleeding in contrast to the multivariate analysis, where only NLR exhibited this trend.
Univariate- And Multivariate Analyses For Vte Recurrences, Major Bleeding And Death Within The First 3 Months. Results Are Expressed As Odds Ratio And 95% Confidence Limits.

Abbreviations: NLR, neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; SII, systemic immune inflammation index (neutrophils x platelets/ lymphocytes); VTE, venous thromboembolism; CrCl, creatinine clearance; PE, pulmonary embolism; DVT, deep vein thrombosis; NS, non-significant.
Discussion
The blood cellular indices have been evaluated in various studies in the literature. These studies have shown that the blood cellular indices may provide both diagnostic and prognostic information in acute VTE. NLR, PLR and SII are the most studied blood cellular indices in acute VTE. Ates et al have identified NLR as an independent predictor of massive PE in 639 patients comprised of acute PE. 17 In this study, NLR found to have a good diagnostic accuracy with an AUC of 0.893 for this outcome. Kasapoglu et al also reported that NLR levels were significantly higher in patients who died within 30 days in 550 patients comprised of acute PE. 18 Interestingly, NLR was not an independent predictor of death for overall patients in this study. But in subgroup analysis in patients without comorbidities showed that NLR was an independent predictor of mortality. Duman et al have shown that an NLR was predictive for 30-day, 6-month and 1-year mortality in a cohort of 828 PE patients. 19
Several studies also evaluated the PLR as a diagnostic and prognostic tool for acute VTE. The study of Ates et al identified PLR as an independent predictor of massive acute PE in 639 patients. 17 In this study, PLR found to have a good diagnostic accuracy with an AUC of 0.877 for this outcome. Kasapoğlu et al reported higher levels of PLR in 550 acute PE patients who have deceased within 30-days of acute VTE. 18 However, PLR was not an independent risk factor in multivariable analysis in this study. Duman et al, have reported that there was no significant difference in PLR levels between deceased and surviving subgroups in 828 PE patients. 19 Additionally, PLR was also not an independent risk factor for death in this study. Kundi et al have found that higher levels of PLR in patients with high sPESI scores was independently associated with in-hospital mortality among 646 patients with acute PE. 20 However, Ghaffari et al did not find a difference in PLR between patients with and without major cardiopulmonary adverse events in 492 acute PE patients. 21 But PLR was associated with in-hospital mortality with an AUC of 0.610 in this study.
In the recent literature, PLR were also considered as a predictor of the VTE occurrence in cancer patients and after surgery. Grilz et al identified a significant association between PLR and the occurrence of VTE in 1469 cancer patients. 22 Yao et al identified a higher preoperative PLR than postoperative PLR in 733 patients after total joint replacement. 23 In this study, the postoperative PLR was independently associated with the occurrence of DVT with an AUC of 0.513 and 0.561 for preoperative PLR and postoperative PLR respectively. Furthermore, Kurtipek et al, have reported higher PLR values in 71 patients with acute PE compared to healthy controls, suggesting that PLR may be associated with pulmonary artery endothelial cell dysfunction. 24
The predictive value of SII was also tested in several previous studies. These studies have shown that it can also be a useful tool for both the diagnosis and prognosis of mortality in VTE. Gok et al reported elevated SII levels in 442 patients with acute PE. SII was also higher in patients who had in-hospital mortality. 25 SII was an independent predictor of massive APE with an AUC of 0.957. Peng et al reported an increased SII in patients with VTE compared to those without VTE. In this study, SII was an independent predictor of VTE after hip fracture of elderly patients. 26
Reported data, obtained from a large series of consecutive patients with acute VTE, reveal that the cellular indices may help to predict adverse outcomes at 90 days, thus supporting the role of the immune/inflammatory response in the pathogenesis of VTE. In this cohort, none of the three cellular indices predicted the risk for VTE recurrences within the first 90 days, but patients with NLR >4.41, >4.96 were at increased risk for major bleeding (68.4% sensitivity and 68.0% specificity) or death (66.9% sensitivity and 66.8% specificity), and those with SII >1134.5 were at an increased risk of death (64.9% sensitivity and 64.9% specificity). One in every 30 patients (3.4%) suffered major bleeding within the first 90 days, and one in every four such patients died of bleeding. Thus, the clinical relevance of these indices at baseline should not be underestimated. On univariate analysis, all 3 cellular indices were associated to a higher risk for major bleeding, as were older age, cancer, recent immobility, hypertension, recent major bleeding, anemia, renal insufficiency or initial VTE presentation as PE. Most of these clinical variables have been identified and validated in the literatuire as independent risk factors for bleeding in patients with VTE.27–29 Interestingly however, only NLR, anemia and renal insufficiency independently predicted the risk for major bleeding. Moreover, both NLR and SII independently predicted the risk of death.
A meta-analysis including 2323 patients from 7 retrospective studies found the NLR and the PLR to independently predict the risk of death (in the short- and in the long term) in patients with acute PE. 15 The prognostic role of the SII (including neutrophils, lymphocytes and platelets) is currently less known, although a retrospective report involving 442 patients with PE suggested its association with worse outcomes, including hemodynamic compromise and in-hospital mortality. 25
In another study on patients with acute PE, NLR and PLR correlated with the severity of PE evaluated by the PESI or simplified PESI scores. 30 In contrast, high NLR values were not associated with more severe risk profiles in a more recent small cohort of less than 100 patients with PE. 31 This study reports t PE patients with tachycardia or hypoxemia to have high NLR and SII values. Thus, the prognostic role of these cellular indices in patients with acute PE needs to be further investigated.
In this study, the value of cellular indices in predicting outcome in patients with acute VTE has been addressed as novel biomarkers based on the utilization of blood counts. The molecular basis of these relationships requires detailed molecular and cellular investigations. Thrombo-inflammatory biomarkers have been extensively investigated and reported previously from a previous study, from our group. 32 A clear relationship between upregulation of inflammatory cytokines has been demonstrated in this comprehensive study. This study also provides an opportunity to demonstrate that, the variations in thrombo-inflammatory biomarkers may be relevant to the changes in the cellular indices, such as NLR, PLR and SII. The RIETE Registry, cohort did not address thrombo-inflammatory biomarkers except for the d-dimer, however the cellular indices were easily retrievable. Such a relationship between the cellular indices and the thrombo-inflammatory biomarkers will provide interesting insight in the understanding of the pathogenesis of VTE. In another study, Darwish et al, have also reported on the dysregulation of hemostatic and inflammatory biomarkers with reference to adhesion molecules TNF-a, and PAI-1. 33 Ongoing studies on the cellular indices in this group and their correlation with the biomarkers investigated is being addressed. In a lymphoma cohort, some of the cellular indices and thrombo-inflammatory biomarkers have been simultaneously measured. Such measurements have provided useful data in stratifying risk and outcomes in cancer patients. 34 Future studies, to complement cellular indices data, with such biomarkers as inflammatory cytokines, tissue factor, and microparticles will provide additional information on the pathogenesis of VTE.
The role of microparticles in the understanding of the pathogenesis of VTE is well known. 35 Microparticles are drive mainly from platelets, white cells, and endothelial lining. These microparticles are pro-coagulant in nature, and profiling of these microparticles has been addressed in several studies. In the current study, the main focus is on demonstrating value of cellular indices in conjunction with a large registry. This registry, thus also offer an opportunity to quantify microparticles, however the current study is mainly focused on cellular indices and correlations with cellular microparticles can be subject of future studies.
The role on inflammation in inducing hemorrhage in thrombocytopenia has been reported previously. Platelets play an important role in inflammatory responses. Inflammatory processes may result in hemorrhagic response to multiple pathways, where the cytokines play a role including the integrins. 36 In this study, recent bleeding was defined as a major bleed less than 30 days prior to VTE. In-terms of the association of cellular indices with bleeding risk, the NLR showed an association with bleeding risk in the multivariate analysis, where as the PLR and SII did not reveal any relevance. Additional data, on a larger cohort will provide furthur insights. Therefore the RIETE Registry provides a unique opportunity to validate the diagnostic and prognostic significance of these indices.
This study has several limitations to consider. First of all, reported findings should be treated with caution considering the limitations of observational studies to infer causality. This study did not include a control group. This study did not address the prognostic relevance of repeated measurements of cellular indices, which may have a higher accuracy than a single one. Reported study only represents the outcomes appearing during the first 90 days. Additionally, this study did not completely consider the clinical characteristics of the patients while including in this study. Increased levels of blood cellular indices is detected in several other illnesses (particularly in cancer patients) other than VTE. Moreover, reported study did not compare other inflammatory biomarkers (such as CRP, d-dimer) with the selected variables. Finally, although clinicians might not perceive that this is readily available, and easily calculated indicators with blood cell counts.
The current analysis also has some strengths. To the best of our knowledge, this is the largest cohort study evaluating the prognostic value of three cellular indices simultaneously in patients with acute VTE. Prior publications concerning the prognostic role of these immune/inflammatory indicators were single-center studies. Our data provides a multicenter perspective, which increases the generalizability of the results. In the current literature, there is no specific cut-off values of NLR, PLR or SII for mortality. This study have obtained different optimal cut-off points of the cellular indices for major bleeding outcomes. Thus, reported study offers a new perspective of the problem, and notable data.
In conclusion, the cellular indices represent a consistent and powerful predictor of major bleeding or death within the first 90 days in patients with acute VTE. This should lead to increased awareness about these indicators, particularly NLR. Nonetheless, the prognostic role of these tests in patients with different risk profiles (ie, active cancer, normotensive acute PE, etc) is still underexplored and warrants further investigations.