
Abstract
Introduction
The frequency of total joint arthroplasty (TJA), including total hip arthroplasty (THA) and total knee arthroplasty (TKA), is expected to increase as the global population is ageing. 1 Venous thromboembolism (VTE), a collective term for deep vein thrombosis (DVT) and pulmonary embolism (PE), is one of the most common complications after TJA and it increases perioperative morbidity and mortality. 2 The incidence of preoperative DVT in TJA patients is as high as 17.9% 3 and that in THA patients is up to 29.4%. 4 VTE is considered a common serious complication after TJA and an important cause of morbidity and mortality, especially in hospitalized patients. After TJA, DVT incidence may reach 40% to 60% without prophylaxis and PE may occur in 0.5% to 2% of the patients.5,6 Therefore, identifying the high-risk factors for preoperative DVT is important for managing perioperative thrombosis in TJA patients.
Albumin inhibits platelet function indirectly and exerts an antithrombotic effect. 7 Low albumin concentration is considered an integrative index for inflammation, hypercoagulability, or disease states that predispose patients to thrombosis.8,9 Low albumin has been found to be independently associated with an increased risk for pulmonary complications, blood transfusions, reoperation, and readmission in patients undergoing total shoulder arthroplasty. 10 Zhu et al 11 found albumin < 35 g/L to be an independent risk factor for preoperative DVT in lower limb fractures. Tan et al 12 demonstrated that albumin < 35 g/L was a risk factor for DVT in closed patella fracture. Song et al 13 reported low albumin levels to be an independent risk factor for preoperative DVT in patients with intertrochanteric fractures.
Most prior studies have focused on the association between low albumin and preoperative DVT in bone fracture patients, as well as the effects of low albumin on postoperative complications in TJA patients. In contrast, we hypothesized that low albumin and preoperative DVT formation were associated in osteoarthritis (OA) patients.
Materials and Methods
Inclusion and Exclusion Criteria
Data Collection
We accessed the electronic medical records and surgical anesthesia information systems and collected patients’ clinical data. Patients’ general information and medical records included: height, weight, body mass index, age, gender, preoperative hypertension, diabetes, coronary heart disease (CHD), chronic obstructive pulmonary disease, chronic bronchitis, OA, cerebral infarction, cancer (Cancer refers to patients who have previously suffered from malignant tumors, including breast cancer, early lung cancer, nasopharyngeal cancer, throat cancer, etc, but have now been clinically cured.), renal failure, use of corticosteroids, smoking, alcohol consumption, major surgery (major surgery requiring anesthesia [general, orthopedic, neurologic, or gynecologic surgery] 14 in the previous 12 months; laboratory examinations: blood type, albumin [in bromocresol green [BCG] method] in our laboratory, and the normal reference range 40–55 g/L), the result of preoperative low extremity vein ultrasound and perioperative blood transfusions (all of our transfusions refer only to transfusions during TJA procedures and were performed in strict accordance with the transfusion guidelines 15 ). After admission, our TJA patient underwent liver function tests followed by lower extremity venous Doppler ultrasound. Liver function tests were performed 6 to 48 h prior to lower extremity Doppler examinations.
Preoperative DVT was defined as DVT detection by Doppler ultrasound between admission and surgery. All patients were examined by Philips IE33 GE Vivid 9, C5-1, and 5 to 10 Hz pulsed Doppler ultrasound. The results were co-diagnosed by two experienced sonographers. The positive criteria for DVT by ultrasound included venous incompressibility, intravascular filling defect, and Doppler signal absence. The location of DVT was classified as follows: distal thrombosis (a previous thrombus at or below the popliteal vein), proximal thrombosis (thrombus above the popliteal vein), and mixed thrombosis (both proximal and distal). This study has been approved by Medical Research and Ethics Review (No. 184, 2022) and registered in the WHO International Clinical Trials Registration (ChiCRT2100054844).
Statistical Analysis
SPSS 26.0 was used for statistical analyses. Specifically, we created the receiver operator characteristic (ROC) curve to determine the cut-off values for preoperative albumin and age and DVT in TJA patients. The cut-off value and the area under the curve (AUC) were calculated. And then, we divided the patients into 2 groups: one above and the other below the cut-off value and risk factors were subsequently analyzed. For enumeration data, the chi-square test or Fisher's exact test was used. The results were represented in percentage (%) and DVT-related variates were analyzed. The variates that were statistically significant in the univariate analysis were included in the multivariate analysis. The adjusted odds ratio (OR) and 95% confidence interval (95% CI) were calculated, to evaluate the preoperative association of low albumin with preoperative DVT in TJA patients.
Results
General Information of Participants
We excluded 3 patients with a history of VTE and genetic thrombophilia; 9 patients who had received anticoagulants at some earlier time before operation; 343 patients with fractures; 25 cases of joint tumors; 19 cases of joint tuberculosis or infection; 194 cases did not have ultrasonic or albumin records before surgery. Finally, 593 patients were excluded and 2133 patients were included.
The mean age was 63.2 ± 12.1 years among all the 2133 TJA patients, 71.5 ± 8.9 years in the DVT group, and 62.7 ± 12.1 years in the non-DVT group (Table 1). The mean height was 156.58 ± 6.4 cm in the DVT group and 158.08 ± 8.33 cm in the non-DVT group. And 1001 cases underwent TKA and 1128 underwent THA. Among them, 794 (38.56%) were men and 1265 (61.44%) were women. Preoperative comorbidities were hypertension (611 cases), diabetes (206 cases), and CHD (112 cases) (Table 2).
Summary of Patient Characteristics.

Abbreviations: BMI, body mass index; DVT, deep vein thrombosis.
Univariate Analysis of Preoperative DVT Risk in Patients Undergoing TJA.

Abbreviations: CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; TJA, total joint arthroplasty.
Characteristics of Patients With a Previous DVT
One hundred and ten cases (5.16%) with DVT before TJA included 81 distal thrombus cases (74%), 13 proximal thrombus cases (14.55%), and 16 mixed thrombus cases (11.82%). Low molecular weight heparin was used for the thrombus. Once proximal DVT formation (acute or nonacute DVT) was detected by preoperative lower extremity Doppler ultrasonography in patients, the inferior vena cava filter was placed before TJA. None of our TJA patients had PE during the perioperative period.
Analysis of Factors Associated With a High Risk of Preoperative DVT
The albumin was 36.8 ± 3.9 g/L in the DVT group and 38.3 ± 3.9 g/L in the non-DVT group,

Diagnostic performances of albumin for predicting DVT in patients undergoing TJA. Albumin was measured by the bromocresol green method in our laboratory, and the normal reference range was 40 to 55 g/L.
Degree of Albumin and the Incidence of Preoperative DVT and Blood Transfusion in Patients Undergoing TJA.

Abbreviations: DVT, deep vein thrombosis; TJA, total joint arthroplasty.
Analysis of High-Risk Factors of Preoperative DVT
Univariate logistic regression analysis revealed that the risk for DVT before TJA in patients with albumin <37.2 g/L was increased by 2.26 times (

Univariate logistic regression analysis of preoperative risk factors for DVT in patients undergoing TJA.
Multivariate logistic regression analysis revealed that the risk for DVT before TJA in patients with albumin < 37.2 g/L was increased by 1.99 times (
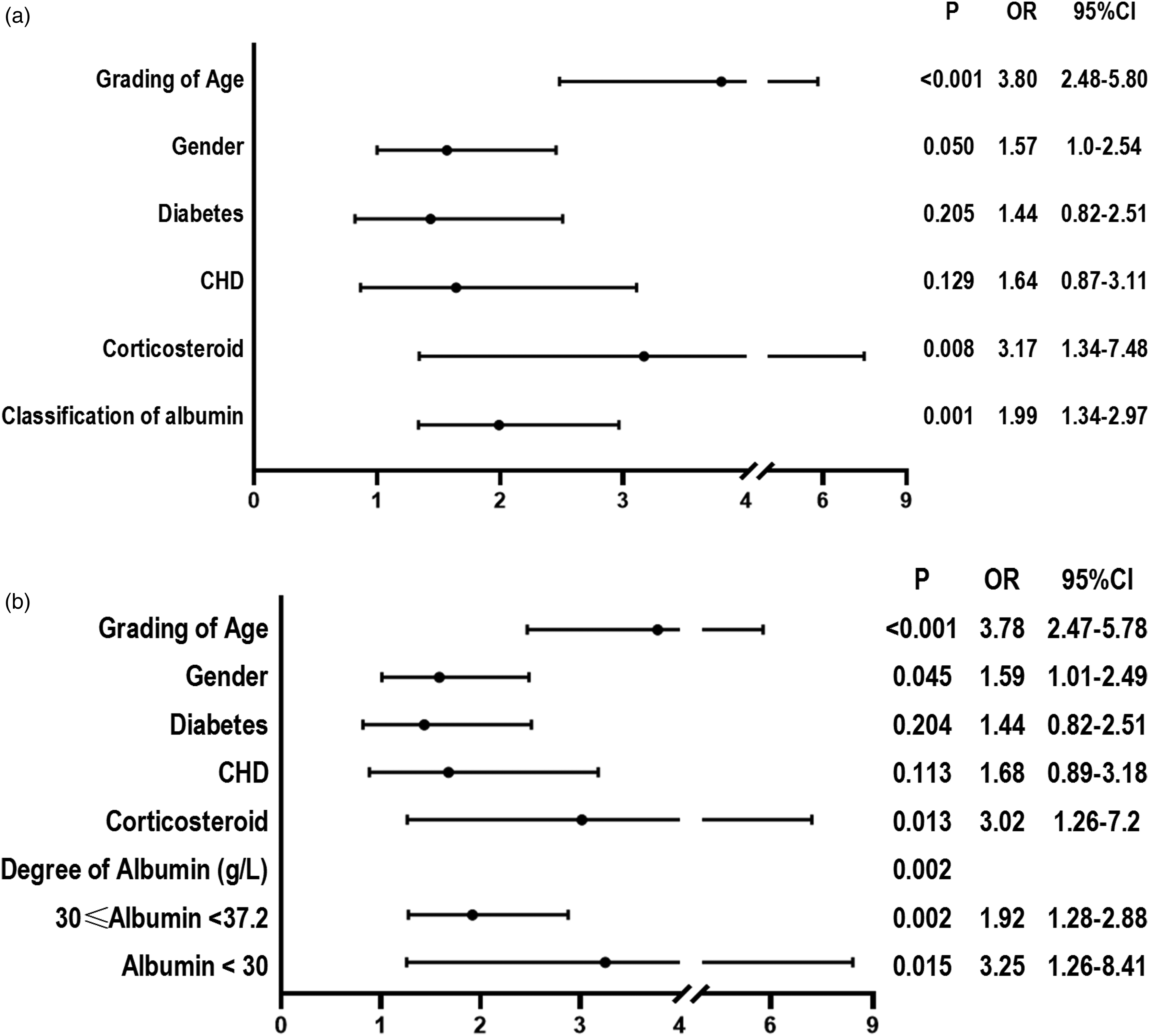
Multivariate logistic regression analysis of preoperative risk factors for DVT in patients undergoing TJA. (a) Multivariate logistic regression analysis of albumin and preoperative DVT in patients undergoing TJA. (b) Multivariate logistic regression analysis of degree of albumin and preoperative DVT in patients undergoing TJA.
Discussion
In our study, 74% of clots were distal in TJA patients who had a previous DVT detected. In our series, all symptomatic DVT was essentially proximal thrombus and mixed thrombus, and the patients with distal thrombus had essentially no obvious clinical symptoms. Song et al 4 demonstrated that 66.7% of the THA patients who were diagnosed with preoperative VTE had another thrombosis at the same sites following the THA. Small-sized thrombosis may lead to PE, hence Smith et al 17 urged attention to medium and small-sized peripheral DVT in patients undergoing THA. If the patient with thrombosis underwent surgery, immobilization and other procedures, DVT may develop, extend or even detach, causing PE, severe disability, or even death. 18 Therefore, we considered it important to identify any occurrence of distal DVT in clinical work.
To our knowledge, the present study is the first to demonstrate an association between albumin levels and preoperative DVT in TJA patients with OA, as well as the first study that has found that the lower the preoperative albumin value, the greater the odds of preoperative DVT being detected in TJA patients, and a higher likelihood for perioperative transfusion. As albumin is measured in the liver function tests, no extra financial burden is imposed on patients. Therefore, compared to other inflammatory cytokines, they are more clinically accessible and more advantageous in predicting DVT formation before TJA. Our findings indicate that patients who are to undergo TJA and have an albumin <37.2 (BCG albumin assay, but lower if the BCP albumin assay is used) should be aware of the potential for a previous DVT to be present. The albumin results measured by BCP and BCG methods are different. In renal failure the BCG methods are preferred. 19 However, in other conditions, the BCG method produces a higher reference range. 19 Coley-Grant et al 16 found that constant bias of approximately + 6 g/L occurred with the BCG method compared to the BCP method. The BCG method reported by Garcia Moreina et al 20 is falsely elevated in patients with low serum albumin and an inflammatory condition due to raised alpha-1 and alpha-2 globulins. However, we did not find an increase in alpha-1 and alpha-2 globulins in patients with OA. Therefore, it is feasible to measure the albumin level by BCG method in TJA patients. Enoxaparin was the most commonly used low molecular weight heparin in our TJA patients. For patients who had a previous DVT, 1 mg/kg once daily, the dose of thromboprophylaxis in patients who had no previous DVT was 30 mg once daily. Enoxaparin was discontinued 12 h before surgery. 21
Association Between Low Albumin, Age, and DVT
Albumin is the most prevalent serum protein and is a commonly used marker of nutritional status.
22
It has been found that up to 50% of orthopedic patients may suffer from protein malnutrition before surgery.
23
And 27% of THA and TKA had varying degrees of low albumin, and the degree was positively correlated with age (> 60 years old).24,25 The incidence of albumin < 37.2 g/L in our TJA patients was 37.4%. And 717 cases were older than 69.5 years old, with an incidence of 33.6%; 316 cases complicated with low albumin, accounting for 44.07% of patients older than 69.5 years. Our study found that patients older than 69.5 years had a 3.8-fold increased risk of preoperative DVT (
Olson et al
30
reported that for every standard deviation drop in serum albumin, there was a 25% increase in the risk of VTE. Chi et al
8
found that albumin < 35 g/L had 2-fold greater odds for developing VTE compared with those with albumin ≥ 42 g/L. Moghadamyeghaneh et al
31
found that serum albumin < 35 g/L significantly increased the risk of developing postoperative DVT and PE. Zhao et al
32
found that albumin < 35 g/L was significantly associated with preoperative DVT in 1515 elderly patients with intertrochanteric fracture (OR = 1.516,
Furthermore, Chi et al
8
reported that the risk of DVT increased approximately 1.4 times for each 5.24 g/L decrease in albumin. Acutely ill hospitalized patients with low serum albumin had an increased VTE risk over 77 days.
8
In nephrotic syndrome, Gyamlani et al
33
found that compared with patients with serum albumin ≥ 40 g/L, those with albumin levels of 30 to 39.9 g/L had a 1.5-fold risk of VTE, whereas those with serum albumin 25 to 29.9 g/L had a 2-fold higher and those with serum albumin < 25 g/L had an almost 3-fold risk of VTE. Lionaki et al
34
reported low albumin to be the dominant independent risk factor for VTE in patients with membranous nephropathy. In their study, 28 g/L was the threshold below which the risk of VTE increased 3.9-fold, and when the albumin level declined further to < 22 g/L, the risk of VTE increased 5.8-fold.
34
These studies reported that low albumin level was associated with a high risk of VTE, which is similar to the present study. Our study found that the lower the preoperative albumin level, the higher the risk of preoperative DVT. Compared to the albumin ≥ 37.2 g/L group, the risk for preoperative DVT in the albumin of 30 to 37.2 g/L group and the albumin < 30 g/L group increased by 1.92 times (
Mechanism of Low Albumin Action on Preoperative DVT in TJA Patients
Low albumin concentration is considered an integrative index for inflammation, hypercoagulability, or disease states that predispose patients to thrombosis. 8 The mechanism for the association between low albumin and preoperative DVT in TJA patients may be 2-fold. First, low albumin may be a marker of inflammation, and inflammation can cause a hypercoagulable state in patients. 35 Several cytokines and chemokines have been detected in joint tissues of OA, such as IL-1, IL-6, and TNF-α. 29 The patients enrolled in our study had a long course of disease, varying from years to decades. Therefore, patients with OA are regarded as having a chronic and long-term inflammatory condition. Second, low albumin can lead to a hypercoagulable state in the blood. Albumin has been found to have anticoagulant properties by inhibiting fibrin polymerization and platelet aggregation. 9 Moreover, albumin appears to enhance the effect of antithrombin III, thus exerting a heparin-like action. 36 Lower serum albumin may also indicate a hypercoagulable state because of its association with higher fibrinogen and factor VIII levels and a shorter activated partial thromboplastin time. 37 Low albumin leads to increased bioavailability of arachidonic acid and increased thromboxane A2, thereby favoring platelet aggregation and hyperactivity. 9 This is consistent with the mechanism underlying the promoting effect of low albumin on recurrent thrombosis.
Association Between Low Albumin and Perioperative Transfusion
Total shoulder arthroplasty patients with a low albumin level during and after surgery had an increased incidence of blood transfusion. Low albumin was independently associated with an increased risk of blood transfusion.
10
In hip fractures, albumin < 35 g/L indicates increased allogenic blood transfusion.
38
Zhu et al found that preoperatively low albumin patients had a 2.26-fold higher risk of perioperative transfusion in 414 elderly patients with femoral neck fractures who underwent hemiarthroplasty. Low albumin was an independent risk factor for blood transfusion in patients undergoing hemiarthroplasty.
39
In our study, when the albumin was <30 g/L, the incidence of perioperative transfusion increased to 57.7%. Our study found that preoperative albumin < 37.2 g/L was a risk factor for perioperative transfusion in TJA patients. We also found that compared to the albumin ≥ 37.2 g/L group, the likelihood for perioperative transfusion in the groups with albumin of 30 to 37.2 g/L or <30 g/L increased by 1.6 times (
Moreover, we also found corticosteroid use was an independent risk factor for preoperative DVT in TJA patients. Lieber et al
40
found that corticosteroids were associated with a 1.47-fold (95% CI 1.13-1.90) increase in the risk of PE and a 1.55-fold (95% CI 1.28-1.87) increase in the risk of DVT within 30 days after surgery. Corticosteroids may disrupt the balance between procoagulant factors and antithrombotic mechanisms
41
and can increase prothrombin plasma concentrations.
42
Corticosteroid has been found to increase the levels of factors VII, VIII, XI, and fibrinogen, which may contribute to increased risk of VTE in patients with chronic corticosteroid use.
43
We found that corticosteroid use had a three times higher risk of preoperative DVT (
However, our study has certain limitations. Some data are incomplete because the study was retrospective. The AUC for albumin was 0.611, indicating a moderate risk of identifying at-risk patients. The association between albumin and preoperative DVT in TJA patients should be further verified in future studies with larger sample sizes and more data.
Conclusion
To our knowledge, this is the first study that has demonstrated the association between low albumin and preoperative DVT in TJA patients. We found that albumin < 37.2 g/L, patients older than 69.5 years, and corticosteroid use were independent risk factors for preoperative DVT in TJA patients. Additionally, the lower the preoperative albumin value, the greater the odds of preoperative DVT being detected by Doppler ultrasound in TJA patients, and the higher the risk of perioperative transfusion.