
Abstract
In spite of considerable fall in MMR in India, maternal health status has not much improved if we consider the 2 important maternal healthcare indicators viz.; female anemia (hb < 12.0 g/dl) and Body Mass Index (BMI).
More than 50% women in their reproductive age are anemic and more than 15% are too thin for their height (BMI<18.5 kg/m2).
The prevalence of anemia and low BMI is more severe among the women belonging to SC and ST categories.
SC and ST women are more prone to anemia (more than 60%) than other (General) women and the rate of prevalence has increased from 2005-2006 to 2019-2021.
The maternal health status is mostly controlled by per capita health expenditure and health infrastructure variables like no. of hospitals and nurses, irrespective of social class.
Introduction
Maternal health is a major public health issue in the world as they play an important role in the development and wellbeing of the children. Maternal health is key to reduce child mortality and improve the nutritional level of children. 1 The United Nations has emphasized that “improving maternal health is key to saving the lives of half of a million women who die as a result of complications from pregnancy and childbirth each year (MDG 5)”2 (United Nations Development Programme (UNDP) 2015) and sets target to “reduce the global maternal mortal ratio to less than 70 per 100,000 live births by 2030 (SDG 3)” (United Nations Development Programme (UNDP) 2020). 3 Even then, WHO Reports on MMR (2023) reveals that about 287 000 women died during and following the pregnancy and child birth in 2020, among these maternal deaths 95% occurred in low and middle income countries (World Health Organization 2023). 4
India had initiated National Safe Motherhood Program in 1992 to 1993 to promote antenatal check-ups and institutional delivery. To achieve the goals set under SDGs, various programs like Janani Suraksh Yojana (2005), Surakshit Matritva Ashwasan, Pradhan Mantri Surakshit Matritva Abhiyan, etc. under National Health Mission(NHM) were launched with the objective of reducing maternal and child mortality by promoting institutional delivery of pregnant women. Unfortunately, in spite of these policies and programs, there is little evidence that maternity has become safer in India. However in the last 2 decades, there have been considerable improvements in the health indicators, including reduction in child and maternal mortality rates.5,6 MMR in India has come down to 103 per 100,000 live births (SRS, 2017-2019). But the factors affecting maternal health status such as female anemia and female Body Mass Index (BMI) has not improved much. The NFHS 5 report reveals that the percentage of all women aged 15 to 49 years who are anemic has risen from 54.1% in 2015-2016 to 59.1% in 2019-2020. Anemia can lead to adverse health outcomes such as low birth weight, neonatal mortality and premature births. 7 Women with BMI less than 18.5 kg/m2 has decreased from 22.9% to 18.7% during the same period, but it is also a matter of serious concern. These 2 factors are reflection of the nutritional level of women. 8
India in aggregate has poor nutritional level. It rather deteriorated as India ranked 101 out of 116 countries in 2021 (fall from 94 in 2020) in Global Hunger Index (2021). The situation of women’s health conditions were much more adverse due to existence of gender discrimination from birth and unequal distribution of health services.9,10 Studies have also shown that lower caste women (particularly SCs and STs) have worse nutritional level (with more anemic and lesser BMI) than other women because their accessibility to proper food, consumption, education and decision making is limited. It is observed that multiple socio-demographic factors ranging from poor economic and educational status, rural residence to higher childbearing of women are responsible for predicting anemia levels among social groups of women in India.5,11,12
The present study on maternal health status has mainly considered 2 factors viz. Female Anemia (hb < 12 g/dl among women within 15-49 years) and Body Mass Index (<18.5 kg/m2 in women), as proxy for maternal health status. It is believed that maternal health status largely depends on immediate health factors: Antenatal Care (ANC), Institutional Delivery and Postnatal Care (PNC). Improvements in maternal health can be achieved by increasing quality of antenatal and postnatal care. 13 Along with these maternal health also depends on other socio-economic factors like health insurance coverage, per capita health expenditure, number of hospitals, PHCs and nurses.
In India, social group is an essential traditional measure of social stratification, which is based on the self-identification as belonging to Scheduled Caste (SC), Scheduled Tribe (ST), Other Backward Classes (OBC) and other (who does not belong to any of these and for simplicity we call it GEN). The people belonging to SC, ST, OBC constitute more than 60% of the total population (Census, 2011) and are considered as disadvantaged groups. Mass poverty, poor diets, limited accessibility to education and health are evident leading to poor maternal health status among the women belonging to these groups. 12 Women from SC, ST and OBCs were less likely to have safe delivery and post natal care utilization. 14
The present study aims to examine the maternal health status in India and its trend among the socially disadvantaged groups (SC & ST) women and compare their status with other (GEN) category. It also attempts to identify the factors responsible for poor health status among SC and ST women.
Methods
The study employs the retrospective observational design, using secondary data to study the maternal health status among various social groups in the states of India and to analyze the factors affecting maternal health status. The study also utilizes the dimension index methodology to compute a composite indices for maternal health. These indices are used to study the maternal health status in the states of India. To find the association between maternal health and its predictor variables, panel regression method is used taking states as cross-section unit over 3 time points.
Panel regression involves estimating regression model that accounts for both individual specific effects and time-specific effects. There are 2 main types of panel regression models: fixed effects model (FE) and random effects model (RE). In FE model, individual specific effects are included in the regression equation as dummy variables. These fixed effects capture unobserved characteristics of individual units that remain constant over time. In a RE model, individual-specific effects are assumed to be random variables.15-17
Data
The data for analysis has been taken from aggregate reports of 3 rounds of National Family Health Survey (NFHS) conducted during 2005 to 2006 (NFHS 3), 18 2015 to 2016 (NFHS 4), 19 and 2019 to 2021 (NFHS 5), 20 conducted by International Institute for Population Sciences (IIPS), Mumbai, a nodal agency for the survey under the Ministry of Health and family Welfare, Government of India. The data on maternal health and other indicators are taken for all 28 states and 2 UTs (Delhi and Jammu & Kashmir) for all 3 surveys. Data on per capita health expenditure and health infrastructural variables were taken from Rural Health Surveys (2005, 2015, and 2019). Per capita net domestic product was taken from RBI data of concerned periods. As the data used in this study are secondary data that are freely available in the public domain, ethical clearance and consent to participation were not needed.
Maternal Health Status Index (MHSI)
The indices of Maternal Health Status and Maternal Healthcare Services are obtained by the Dimension Index (DIs) following Iyengar and Sudarshan method.21-23

For each indicator, DI is obtained using above formula for each state and the average of all DIs for each indicator has been taken to obtain Composite Index. The value ranges from 0 to 1, which implies larger the value better is the performance. For the indicators female anemia and BMI, higher value implies worse performance, the DI is modified as follows

Panel regression analysis
To understand the factors affecting maternal health status, panel regression was applied, taking state as cross section over 3 time points respective of 3 rounds of NFHS. The dependent variable is Maternal Health Status Index, composed of DIs of female anemia and BMI for social groups SCs, STs and GEN (other castes). Anemia is defined as the hb level < 12 g/dl and BMI is defined as below 18.5 kg/m2. The Predictor variables taken are Antenatal Care (ANC), Institutional Delivery, Postnatal Care (PNC) and Health Insurance Coverage (women) among different social groups. The other independent variables taken are per capita net state domestic product (PCNSDP), per capita health expenditure (PCHE), number of PHCs, hospitals and nurses.
The panel regression model is given as follows:

Where MHSIit is the index for ith state at time

The composite index viz. Maternal Health Status Index (MHSI) for each state for 3 rounds of NFHS was computed by taking average of DIs on female anemia and BMI. Similarly DIs for all independent variables were obtained for all states and UTs for 3 periods.
The Spearn’s Correlation coefficient between the MHSI and DIs of dependent variables was obtained to study the correlation between maternal health status and those indices. The determinants of maternal health status were obtained through a panel regression of MHSI on the DIs of several healthcare variables.
The Conceptual Framework for the study of Maternal Health Status is given below (in Figure 1):

Conceptual framework for the study of maternal health status.
Female anemia and body mass index (BMI) have been taken as proxy of Maternal Health Status. World Health Organization (WHO) defined anemia as a reduction in the proportion of red blood cells or decline in the concentration of hemoglobin (hb) level or insufficient oxygen caring capacity to fulfill the physiological demand. The NFHS has defined 3 levels of female anemia: mild (hb 10.0-11.9 g/dl, moderate (hb 7.0-9.9 g/dl) and severe (hb < 7.0 g/dl). Any anemia is defined as the hb < 12.0 g/dl. In our study, we have taken the percentage of women suffering from “any anemia.” The BMI is defined as a person’s weight in kilograms divided by the square of his height in meters (kg/m2). The BMI less than 18.5 kg/m2 is defined as “total thin” and percentage of total thin women is taken for our study.
Results and Discussion
Table 1 shows the composite scores of Maternal Health Status Index (MHSI), which is an average of dimension indices of female anemia and BMI. The MHSI for 3 categories (SC, ST, and GEN) were calculated for all 30 states for 3 rounds of NFHS (rounds 3 to 5). The value of MHSI varies from 0 to 1, higher the value better is performance in maternal healthcare. We have divided all the states on the basis of MHSI score into 3 categories: low performer (MHSI < 0.5), moderate performer (0.5 < MHSI < 0.7 and high performer (MHSI > 0.70) states. As it is clear from the table, the states of Andhra Pradesh, Assam, Bihar, Chhattisgarh, Gujarat, Jharkhand, Madhya Pradesh, Maharashtra, Odisha, Tamil Nadu, Telangana, and West Bengal are the low performer states for all the social groups for all 3 rounds of NFHS. Seven states are moderate performer. Only 6 states are having score more than 0.70.
Composite index for maternal health status and maternal health care services.

Source: Authors’ own calculation.
Inequity in the maternal health status could be seen as the performance of states is not equal for all the social groups. The performance of SC and ST mothers is worse than GEN mothers in the states of Andhra Pradesh, Chhattisgarh, Haryana, Jharkhand, Kerala, Madhya Pradesh, Odisha, Tamil Nadu, Uttar Pradesh, and West Bengal. The situation is worsening for maternal health among disadvantaged groups in few states.
The trends of the maternal health status index also reveals the performance of the states in 3 groups over the 3 rounds of NFHS (Figure 1). It is good to observe the increasing trend in the scores of index by majority of states for all 3 social groups. For SC category, the scores for Arunachal Pradesh, Sikkim, Uttar Pradesh and Uttarakhand have increased by more than 2 times during the period 2005-2006 to 2019-2021. The states like Chhattisgarh, Gujarat, Madhya Pradesh, Maharashtra, Nagaland, and Punjab has shown decreasing trend in MHSI scores during the same period, which is matter of concern. For ST category, MHSI score show the increasing trend except the states of Assam, Chhattisgarh, Gujarat, Meghalaya, Nagaland, and Tamil Nadu. For General category, the almost all the states have increasing scores. Goa, Gujarat, Maharashtra, Tamil Nadu, and Telangana states show the decreasing trend.
As the data are found not to be normally distributed (Shapiro-Wilk
Spearman’s correlation coefficient between Maternal Health Status Index (MHSI) and dimension indices.
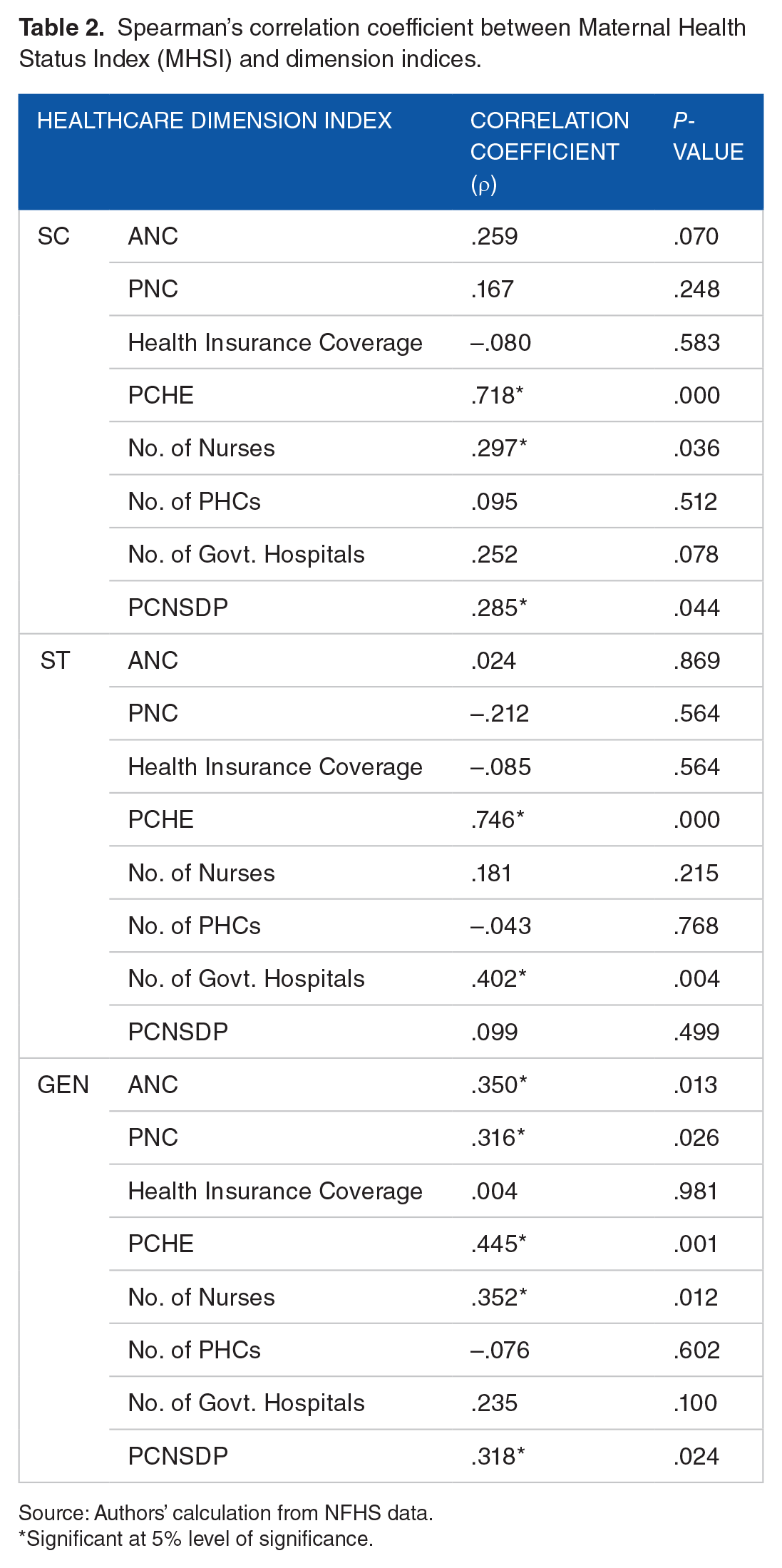
Source: Authors’ calculation from NFHS data.
Significant at 5% level of significance.
To examine the association between the maternal health status and maternal healthcare service variables, panel regression was used with healthcare service dimension indices to understand their effect on composite index of maternal health status. The regression was run for 3 social groups separately to understand the effects of maternal health service and other health related indices on respective MHSI. The result (in Table 2) clearly shows that all the healthcare variables have positive effect on MHSI, except of health insurance coverage for SC and ST and of PNC and PCNSDP for ST category.
For SC category, among 8 dependent variables included, only 3 (PCHE, the number of nurses, number of government hospitals) are significantly associated with the MHSI. Among the 3 significant variables, larger effect on MHSI was from PCHE (coefficient = .68,
Overall, the results show significant relationship between some healthcare variables and maternal health status across different social groups. For instance, PCHE and the number of nurses show significant positive relationship with MHSI in all social groups. However, the significance and magnitude of these relationships vary across different groups, as indicated by the coefficients and
Delimitation of the Study
We have limited our study to 2 health indicators viz. female anemia and BMI as proxy of maternal health. NFHS has defined various levels of anemia and BMI. We have taken anemia with hb level < 12 g/dl and BMI < 18.5 kg/m2 to construct maternal health service index. In our study, 1 of our aims is to find the effect of different socio economic and health infrastructural variables like PCNSDP, per capita health expenditure, and availability of health infrastructure on maternal health among mothers of SC and ST classes. The data on these variables were taken from other sources and are in aggregated form. Thus, we used aggregated data instead of unit level data. Also the study is limited to 28 states and 2 union territories of India due to small size of sample for other union territories.
Conclusion
The study was carried out to understand the situation and trend of maternal health status using an index viz. MHSI (composite index of DIs of female anemia and BMI) among SC, ST, and GEN category female and to examine the impact of various health services and health related variables on maternal health status on maternal health status.
The findings of the study shed light on the complex landscape of maternal health in India, particularly among social disadvantage groups such as scheduled caste (SC) and scheduled tribe (ST). Despite numerous initiatives and programs aimed at improving maternal health outcomes, challenges persist, as evidenced by the prevalence of maternal anemia and low body mass index (BMI) among women, which are key indicators of maternal health status.
The analysis of the MHSI reveals disparities in maternal health outcomes across states and social groups. States like Andhra Pradesh, Assam, Bihar, Chhattisgarh, Gujarat, Jharkhand, Madhya Pradesh, Maharashtra, Odisha, Tamil Nadu, Telangana, and West Bengal consistently perform poorly across all rounds of the NFHs. Moreover, the situation is particularly serious for SC and ST mothers in certain states, where their health outcomes lag behind those for women from other social groups.
Despite these challenges, there are positive trends observed in maternal health indicators overtime, with improvements noted in the majority of the states and social groups. However, there are also concerning trends, such as declining MHSI scores in some states, underscoring the need for continued effort to address maternal health disparities.
The correlation and panel regression analyses further highlight the importance of healthcare service provision in improving maternal health outcome. Factors such as per capita health expenditure (PCHE), number of nurses, and availability of government hospital emerge as significant predictor of MHSI, particularly for SC and ST communities.
After examining the overall findings of the study, it is observed that maternal health status in India is still low as the performance of most of the states remain low for all 3 social groups. There are several socio-economic and health related variables are responsible for this low performance. The variation of maternal health across social groups can be seen.
It is evident from the above discussion that the problem of low maternal health status remain a major problem in India. The government should adopt such policies which can increase the health infrastructure like no. of health centers, hospitals, nurses especially in the areas where disadvantage groups like SCs, STs, inhabit in a large proportion. The quality of ANC and PNC care should be improved by creating awareness by ASHAs and strengthening the Janai Surakshs Yojana (JSY) in the states. The per capita health expenditure by all the states should be increased through allocation of more fund to health sector in the budget so that higher expenses on health infrastructure can be ensured.
Overall, this study underlines the critical importance of targeted interventions and policies aimed at addressing the multifaceted determinants of maternal health, especially among socially disadvantageous groups. By focusing on improving access to quality healthcare services and addressing underlying socio-economic factors, India can make significant strides toward achieving the Sustainable development goals (SDGs) of reducing maternal mortality and improving maternal health by 2030.
Supplemental Material
sj-docx-1-his-10.1177_11786329241254206 – Supplemental material for Understanding of Maternal Health Status in Different Social Groups in India Using NFHS Data
Supplemental material, sj-docx-1-his-10.1177_11786329241254206 for Understanding of Maternal Health Status in Different Social Groups in India Using NFHS Data by Santosh Tamang and Uttam Kumar Sikder in Health Services Insights
Supplemental Material
sj-docx-2-his-10.1177_11786329241254206 – Supplemental material for Understanding of Maternal Health Status in Different Social Groups in India Using NFHS Data
Supplemental material, sj-docx-2-his-10.1177_11786329241254206 for Understanding of Maternal Health Status in Different Social Groups in India Using NFHS Data by Santosh Tamang and Uttam Kumar Sikder in Health Services Insights
Supplemental Material
sj-docx-3-his-10.1177_11786329241254206 – Supplemental material for Understanding of Maternal Health Status in Different Social Groups in India Using NFHS Data
Supplemental material, sj-docx-3-his-10.1177_11786329241254206 for Understanding of Maternal Health Status in Different Social Groups in India Using NFHS Data by Santosh Tamang and Uttam Kumar Sikder in Health Services Insights
Footnotes
Funding:
Declaration of conflicting interests:
Author Contributions
ORCID iD
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.