
Abstract
Keywords
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is a very aggressive disease with poor prognosis and is expected to become the second leading cause of cancer-related mortality by 2030. 1 Currently, early diagnosis of pancreatic cancer is difficult, and no effective treatment options exist for advanced pancreatic cancer. Most patients with PDAC do not develop symptoms until the disease progresses, and when symptoms appear, they are usually vague and nonspecific.2,3 In addition, immunotherapy for PDAC has shown limited effectiveness. 4
A popular serum biomarker for PDAC is the tumor marker sialyl Lewis A blood group antigen (sLea) carbohydrate antigen 19-9 (CA 19-9) 5 which exhibits 80% to 90% sensitivity and specificity in symptomatic individuals.6,7 However, 10% of patients do not express sLea, 8 and thus, the CA 19-9 levels cannot be used for the diagnosis of this group of patients. In addition, biliary obstruction and benign pancreaticobiliary illness may also cause an increase in CA 19-9 levels.9-11
Therefore, to assess the extent of disease more accurately before treatment, new potential diagnostic markers for PDAC should be explored.
In the present study, we analyzed blood samples from patients with PDAC using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS).
12
We found that the plasma fibrinogen levels of patients with PDAC correlated with their overall survival (OS), and this correlation was statistically significant. In particular, the mean fibrinogen level was significantly higher in the PDAC group than in the control group (3.08 ± 0.565 vs 2.54 ± 0.249 log10 ng/mL,
Urine albumin excretion (UAE) is another potential PDAC biomarker. Abnormal UAE as an early marker of diabetic nephropathy is defined as a urinary albumin excretion rate (UAER) in the range of 20 to 200 μg/min (or 30-300 mg/24 h) or a urinary albumin/creatinine ratio (ACR) of 30 to 300 mg/g. 22 At this stage, the lesions remain reversible, and timely intervention can prevent progression to clinical proteinuria. 22 In the hyperglycemic state of diabetes, which is highly susceptible to diabetic nephropathy, the glomerular filtration membrane normally prevents the excretion of most albumin to the urine.23,24 In the early stages of diabetic nephropathy, the glomerular filtration membrane charge and molecular barriers are impaired, leading to increased albumin filtration and impaired tubular reabsorption, resulting in microalbuminuria. 25 New-onset diabetes and insulin abnormalities are risk factors for PDAC. 26 Approximately 25% of patients with PDAC have diabetes and 40% have prediabetes, which is predominant in patients with new-onset diabetes mellitus. 27 Hence, new-onset diabetes may be associated with early diagnosis of pancreatic cancer, and consequently, detecting UAE abnormalities may help identify this group of patients. A large number of studies have shown that an increase in UAE is closely related to the onset and progression of many diseases. Some studies have shown that the higher the UAE, the higher the risk of developing systemic cancer, lung cancer, and mortality. 28
Herein, we demonstrated the clinical utility of serum fibrinogen and urinary albumin excretion (UAE) as indicators of PDAC using Mendelian randomization (MR). The MR uses genetic variations (eg, single-nucleotide polymorphisms [SNPs]) to assess the causal effect of exposure (eg, fibrinogen levels, UAE) on a disease (eg, PDAC). 29 The proposed method has several advantages. First, MR enhances the reliability of causal inferences by reducing the influence of confounding factors through the random assignment of genetic variants. 30 Second, MR effectively avoids the problem of reverse causation because genetic variants are determined before an individual is born. 31 In addition, MR can reveal the directionality between exposure and outcome, providing evidence of true causality. As it is usually based on existing data from genome-wide association studies, MR is particularly suitable for factors that are difficult to study through randomized controlled trials. Based on the clinical information of patients with pancreatic cancer at the Peking Union Medical College Hospital from 2019 to 2024, we constructed a model for a more complete prediction of pancreatic cancer.
Methods
Mendelian randomization
Study design and source of data
A 2-sample MR study was conducted using data from a large-scale genome-wide association study (GWAS) of fibrinogen levels, UAE, and PDAC. The MR relies on 3 main assumptions 32 : (1) the association assumption: SNPs are strongly associated with exposure factors; (2) the independence assumption: SNPs are independent of the confounding variables; and (3) the exclusivity assumption: the SNP does not act on the outcome variable through pathways other than the exposure factor. The design is illustrated in Figure 1.

Mendelian randomization design for causal analysis of fibrinogen level, urinary albumin excretion (UAE), and pancreatic ductal adenocarcinoma (PDAC).
Data sources
Data on fibrinogen levels, UAE, and PDAC were obtained from the EMBL-EBI (https://www.ebi.ac.uk/) and FinnGen (https://www.finngen.fi/en) databases. As all data were obtained from freely accessible databases, no further ethical clearance was required. EMBL-EBI provided data on fibrinogen levels (data set GCST003194), which included information on 120 246 individuals of European ancestry. The UAE data were obtained from EMBL-EBI and included information on 382 500 individuals of European ancestry (data sets GCST006586, GCST002382, and GCST006463). EMBL-EBI also identified 20 SNPs that were strongly associated with fibrinogen levels and 74 SNPs that were strongly associated with UAE. Following the removal of confounding variables and linkage disequilibrium, 19 SNPs were associated with fibrinogen levels, whereas 26 were associated with UAE. In accordance with the Effect Allele Frequency (EAF) findings, duplications and mismatches were eliminated by coordinating the allelic orientation with respect to the exposure and outcome SNPs.FinnGen provided PDAC data, which included 314 193 individuals from Europe and 731 other cases (Data set No. finngen_R10_C3_PANCREAS_ADENO_DUCTAL_EXALLC).
Choosing genetic instrument variables
To verify Hypothesis 1, SNPs that were highly correlated with the exposure factors in the GWAS were first filtered using a cutoff value of

where R2 is the overall explained variation in a few selected exposure-related instrumental variables (IVs); MAF is the influence of small allele frequency; and β is the predicted effect value of SNP.
Data analysis
The present study adhered to the STROBE-MR guidelines. 33 Two-sample MR analysis was conducted using the “TwoSampleMR (0.6.6)” program package for R 4.4.0. The fundamental techniques used for determining causation are weighted median, MR-Egger, and inverse variance weighting (IVW). Among these approaches, the primary analytical technique for achieving unbiased causal estimation without horizontal pleiotropy is IVW. The weighted median and MR-Egger are complementary techniques for MR analysis. The latter is less susceptible to measurement errors and outliers, whereas the former occasionally provides reliable causal inference even in the presence of pleiotropy.
The MR-pleiotropy residual sums and outliers approach (MRPRESSO) was used to rectify and evaluate the MR analyses following the removal of outlier SNPs (
Summary of Mendelian randomization workflow
In this study, 2-sample MR analysis was performed. First, significant genome-wide SNPs associated with fibrinogen levels and UAE were identified from published GWAS data sets. Independent instruments were selected after linkage disequilibrium clumping and harmonization of alleles between the exposure and outcome datasets. Second, causal estimates of the effects of fibrinogen and UAE on PDAC risk were obtained using IVW MR as the primary method, complemented by MR-Egger and weighted median approaches. Third, sensitivity analyses were conducted, including heterogeneity tests, pleiotropy assessments, and leave-one-out analyses, to evaluate robustness. Finally, significant loci were annotated to candidate genes and subjected to functional enrichment analyses to explore their biological mechanisms.
Pancreatic cancer diagnosis and prognosis evaluation model
Pancreatic cancer samples
This study was conducted according to the 1975 Declaration of Helsinki (revised in 2024). 34 The clinical data of patients with pancreatic cancer at Peking Union Medical College Hospital from 2019 to 2024 were collected. In addition, the clinical data of 150 patients with benign pancreatic tumors were collected. A total of 169 patients with malignant pancreatic tumors were included in the study, including 114 patients with PDAC, as confirmed by pathological diagnosis. Patients who lacked complete clinical data and those who did not sign the informed consent form or whose legal representatives did not provide consent were excluded. The completeness of the clinical information (sex, age, pathological diagnosis, etc) of patients included in the study was ensured to be consistent with the description of the same data in different systems for patients included in the study; moreover, the values were within the range of clinical logic or practical needs. In this study, data on sex, age, tumor location, pathological diagnosis, as well as UAE, fibrinogen, and serum CA19-9 levels were collected. This study was approved by the Ethics Committee of the Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, under approval number I-24PJ1452. All participants or their legal representatives provided informed consent to participate in this study and agreed to its publication.
Statistical analysis
The statistical method of chi-square test was used for dichotomous variables (sex, UAE level), whereas the normality test, analysis of variance (ANOVA), independent samples Kruskal-Wallis test, and independent samples median test were performed for continuous variables (fibrinogen level, age). All tests were performed using the IBM SPSS Statistics version 27 (SPSS Inc, Chicago, Illinois). The accuracy, sensitivity, and specificity of UAE, fibrinogen, and CA19-9 levels in distinguishing patients with pancreatic cancer from those with benign tumors were evaluated using the receiver operating characteristic (ROC) curve analysis.
Gene Ontology and Kyoto Encyclopedia of Genes and Genomes pathway analysis, functional enrichment analysis, and protein-protein interaction
Protein-protein interactions were analyzed using STRING 12.0 (https://cn.string-db.org/), followed by the conduct of Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analyses with a screening condition of FDR ⩽ 0.05.
Results
We analyzed the causal effects between exposure factors (UAE and fibrinogen levels) and outcome variable (PDAC) using 2-sample MR. Forest plots of MR analyses are shown in Figure 2, whereas scatter plots of effect estimates for each SNP are shown in Supplemental Figure S1. For SNPs with significant effects, we revealed the potential mechanisms of fibrinogen levels and UAE as biomarkers of PDAC using GO and KEGG pathway analyses, functional enrichment analysis, and protein-protein interactions. We also proposed an assessment model for pancreatic cancer diagnosis and prediction based on MR analysis results using clinical samples.

MR analysis of the causal relationship between fibrinogen level, UAE, and PDAC. (A) Forest plot of the estimated effect value of the causal relationship between fibrinogen level and PDAC, the estimated effect value of rs12777 had a more significant effect on the total estimated effect value. (B) Forest plot of the estimated effect value of the causal relationship between UAE and PDAC, the estimated effect value of rs12727104 had a more significant effect on the total estimated effect value.
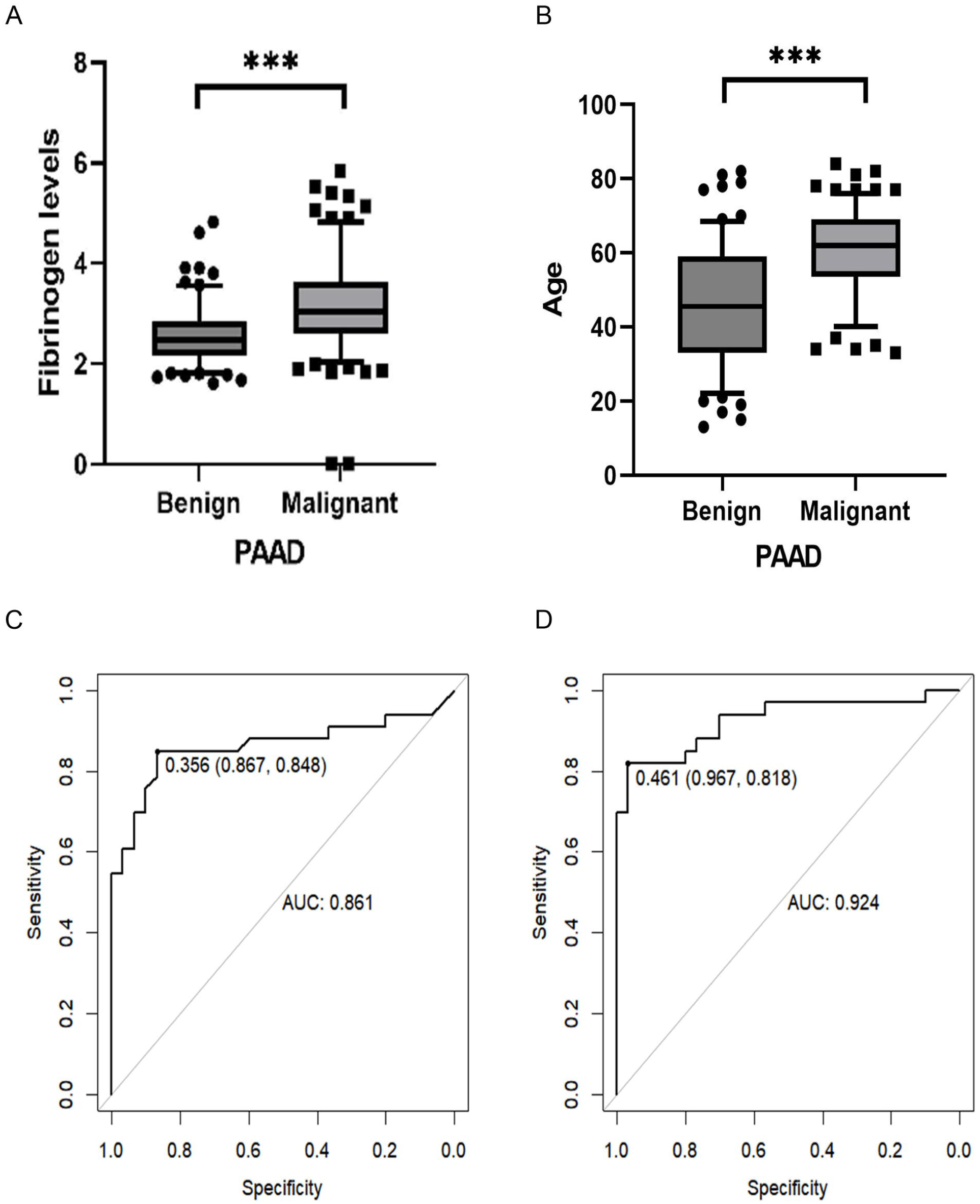
Statistical table of clinical data of patients with benign and malignant tumors of the pancreas and ROC curves of subjects with fibrinogen level, UAE, and CA19-9 in patients with benign and malignant tumors of the pancreas. (A) Point-box plot of fibrinogen levels in benign and malignant tumors of the pancreas. Fibrinogen levels in the group of malignant tumors of the pancreas were significantly higher than those in the group of benign tumors of the pancreas. (B) Dot-box plots of age statistics of patients with benign and malignant tumors of the pancreas. The pancreatic malignant tumors of the patients were significantly older than patients with benign tumors of the pancreas. (C) Working characteristic curve of subjects with CA19-9 in patients with benign and malignant tumors of the pancreas, with a specificity of 0.867, a sensitivity of 0.848, and an AUC of 0.861. (D) Working characteristic curves of subjects with CA19-9, UAE, and CA19-9 in patients with benign and malignant tumors of the pancreas. Working characterization curve with specificity of 0.967, sensitivity of 0.818, and AUC of 0.924.
Mendelian randomization
Mendelian randomization analysis results of fibrinogen levels and pancreatic ductal adenocarcinoma
In fibrinogen levels, all 3 analytical methods showed a positive correlation between fibrinogen levels and PDAC: IVW (95% confidence interval [CI]: 1.630 to 8.753;
Mendelian randomization analysis results of urinary albumin excretion and pancreatic ductal adenocarcinoma
In UAE rate, all 3 analytical methods showed a positive correlation between UAE and PDAC: IVW (odd ratio [OR] = 6.978; 95% CI: 0.055 to 3.831;
Gene Ontology and Kyoto Encyclopedia of Genes and Genomes pathway analysis, functional enrichment analysis, and protein-protein interaction
Effect of the SLC22A4 (rs12777) on pancreatic ductal adenocarcinoma
To explore the potential biological functions of SLC22A4, we performed GO, KEGG pathway, and functional enrichment analyses. The GO annotation consisted of 3 parts: biological processes, molecular functions, and cellular components (Figure 4). Biological process and molecular function analyses showed that SLC22A4 and related genes were enriched in biological processes related to drug transport, metabolic processes, and immune responses, and in molecular functions related to transporter activity, enzyme binding, and catalytic activity. In addition, SLC22A4 and related genes were closely associated with cellular components such as cell membranes, cytoplasm, and ribosomes (Figure 5). The KEGG pathway enrichment analyses indicated that SLC22A4 and related genes were involved in pathways critical to cancer biology. These pathways included ABC transporters, bile secretion, and antifolate resistance pathways (Figure 6B). SLC22A4 is associated with the ABC transporter, which contributes to chemoresistance in cancer cells. The involvement of the bile secretory pathway may reflect metabolic dysregulation in PDAC. The role of SLC22A4 in the antifolate resistance pathway highlights its potential role in the development of therapeutic resistance. Protein interaction network analysis revealed that SLC22A4 interacts with various transporters and immune-related proteins. Notably, SLC22A4 interacts with ABC transporters, such as ABCC1, ABCC3, and ABCC5, which have been implicated in drug resistance and metabolic processes. In addition, interactions with immune-related proteins such as RUNX1 and PTPN22 suggested that SLC22A4 plays a role in immune regulation of the tumor microenvironment (Figure 7B). Overall, SLC22A4 appears to play a multifaceted role in PDAC, participating in immune regulation, metabolic control, and drug resistance mechanisms. The interactions of SLC22A4 with key transporters and immune-associated proteins, as well as its involvement in key pathways, indicate SLC22A4 as a potential therapeutic target for PDAC. Further experimental validation is required to elucidate the exact mechanisms by which SLC22A4 affects tumor biology and therapeutic efficacy. In summary, our data support a plausible mechanism in which rs12777 alters SLC22A4 function or expression, leading to systemic inflammation and changes in immune cell behavior, which in turn increase fibrinogen levels and ultimately modify the PDAC microenvironment.

The bubble plots showing GO pathway enrichment data for FMO4 and related genes. (A) Molecular function (gene ontology) enrichment. (B) Biological process (gene ontology) enrichment. (C) Cellular component (gene ontology) enrichment.

The bubble plots showing GO pathway enrichment data for SLC22A4 and related genes. (A) Molecular function (gene ontology) enrichment. (B) Biological process (gene ontology) enrichment. (C) Cellular component (gene ontology) enrichment.

The bubble plots showing KEGG pathway enrichment data. (A) The bubble plots showing KEGG pathway enrichment data for FMO4 and related genes. (B) The bubble plots showing KEGG pathway enrichment data for SLC22A4 and related genes.

Protein-protein interaction network. (A) Protein-protein interaction network for FMO4. (B) Protein-protein interaction network for SLC22A4.
Effect of the FMO4 (rs12727104) on pancreatic ductal adenocarcinoma
Biological process and molecular function analyses revealed that FMO4 and its related genes were enriched in biological processes related to drug metabolism, detoxification, and oxidative stress and molecular functions related to oxidoreductase activity, flavin adenine dinucleotide (FAD) binding, and xenobiotic metabolism. In addition, FMO4 and related genes were closely associated with cellular components, such as the endoplasmic reticulum and cytoplasm (Figure 4). The KEGG pathway enrichment analysis revealed that FMO4 and its related genes were enriched in cytochrome P450, P450-to-xenobiotic metabolism, and chemocarcinogenesis (Figure 6A). The role of FMO4 in chemocarcinogenic pathways highlights its potential contribution to tumorigenesis. Protein interaction network analysis revealed that FMO4 interacts with various metabolic enzymes and transporters (Figure 7A). Notably, FMO4 interacts with cytochrome P450 enzymes (eg, CYP3A4, CYP2C9, and CYP2C19), which are implicated in drug metabolism and detoxification processes. In addition, interactions with transporters such as UGT1A1 and UGT1A6 suggested that FMO4 plays a role in metabolite conjugation and excretion. These results suggested that FMO4 plays a multifaceted role in PDAC by participating in metabolic detoxification, drug resistance, and the oxidative stress response. Its interactions with key metabolic enzymes and transporters as well as its involvement in key pathways indicate FMO4 as a potential therapeutic target for PDAC. However, further experimental validation is required to elucidate the exact mechanism by which FMO4 affects tumor biology and therapeutic efficacy. These findings suggested that rs1227104 may alter FMO4 activity or expression, leading to disturbed metabolic and oxidative homeostasis. This contributes to increased UAE and altered immune metabolism, thereby promoting changes in the PDAC microenvironment.
Pancreatic cancer diagnosis and prognosis evaluation model
Patient characteristics
Table 1 and Figure 3 present the demographic data of patients with benign and malignant pancreatic tumors. Patients with pancreatic malignant tumors were significantly older than those with benign pancreatic tumors (
Demographics and tumor status of patients with pancreatic cancer.

Statistical data and tumor status of patients with benign and malignant pancreatic tumors. Patients with pancreatic malignant tumors were significantly older than those with benign pancreatic tumors; the number of male patients with pancreatic malignant tumors was higher than that of female patients; fibrinogen levels in the pancreatic malignant tumor group (3.16 ± 0.90) were significantly higher than those in the pancreatic benign tumor group (2.56 ± 0.55); the urine protein positivity rate of patients with malignant pancreatic tumors was significantly greater than that of patients with benign pancreatic tumors. The age group “<53” means “9-52,” whereas the age group “⩾ 53 (53-87)” means “53-87.”
Fibrinogen levels and urinary protein excretion rate in benign and malignant pancreatic tumors
The fibrinogen level in the pancreatic malignant tumor group (3.16 ± 0.90) was significantly higher than that in the pancreatic benign tumor group (2.56 ± 0.55,
Receiver operating characteristic curve analyses in benign and malignant pancreatic tumors
The prediction model for pancreatic malignancy constructed from CA19-9 levels of patients with benign and malignant pancreatic cancer showed an area under the curve (AUC) of 0.861, specificity of 0.867, and sensitivity of 0.848, whereas the prediction model constructed from CA19-9-assisted fibrinogen levels and urinary protein excretion rate showed an AUC of 0.924, specificity of 0.967, and sensitivity of 0.818 (Figure 3C and D). The inclusion of both fibrinogen and UAE levels increased the prediction rate of pancreatic malignancy by 6.36%.
Discussion
Pancreatic cancer, especially PDAC, is a lethal malignant tumor of unknown etiology. 35 The worldwide PDAC incidence is predicted to reach 18.6 cases per 100 000 people by 2050, with a global average annual growth rate of 1.1%. Treating PDAC is a formidable challenge, with a mortality/morbidity rate of 98% and a 5-year OS of 2% to 9%. Cancer type, serum albumin level, tumor size, treatment choice, access to healthcare, and individual characteristics (eg, age, sex, health, and lifestyle) influence OS rates. 36 In conclusion, continued research on risk factors, early detection methods, and treatment strategies for PDAC is essential. Morbidity and mortality rates have remained relatively stable or have slightly increased. 37 In certain regions, PDAC may surpass breast cancer as the third most prevalent cause of death by 2025. 38 Therefore, conducting further studies on PDAC risk factors, early detection techniques, and treatment strategies is critical.
Elevated fibrinogen levels are an independent poor prognostic factor in various cancers, including lung, gastric, colorectal, liver, and breast cancers.39-42 Elevated fibrinogen levels are associated with a poor prognosis in a wide range of cancers, and the specific role and mechanism of action of fibrinogen in PDAC deserve in-depth investigation. Fibrinogen creates an immunosuppressive microenvironment by recruiting immunosuppressive cells (eg, M2-type tumor-associated macrophages, myeloid-derived suppressor cells) and suppressing T-cell activity. Its degradation products (eg, fibrinopeptides) can directly activate proinflammatory factors such as transforming growth factor-beta (TGF-β) and interleukin 6 (IL-6), promote Th17/Treg imbalance, and weaken the antitumor immune response.14,43,44
The MR analysis of fibrinogen levels in PDAC showed that the estimated effect size of SLC22A4 (rs12777) had a more significant effect on the overall combined effect size. Several SLCs have been shown to be involved in glucose uptake and lactate release, as well as promote the phagocytosis of apoptotic cells, and as cellular autophagy and apoptosis are critical processes in tumor immunotherapy responses, SLC-mediated metabolic regulation may influence therapeutic outcomes.
45
Moreover, the interaction of SLC22A4 with RUNX1 and PTPN22 suggests that SLC22A4 is involved in immune-related processes, potentially through regulating the tumor microenvironment. This regulation may affect immune cell infiltration and function, thereby influencing tumor monitoring and progression. The GO and KEGG analyses further confirmed the relevance of this gene in PDAC by linking it to hallmark pathways of cancer biology, such as cell proliferation, survival, and treatment tolerance pathways. By analyzing the GSE49641 data set, a previous study showed that the expression level of
Each UAE doubling was associated with a 7% higher risk of overall cancer (hazard ratio [HR] = 1.06) and a 15% higher risk of urological cancer (HR = 1.14).
28
Elevated UAE levels have been associated with poor prognosis in a variety of cancers51,52 including PDAC; however, the specific mechanisms deserve in-depth investigation. In the MR analysis examining the relationship between UAE and PDAC, the SNP rs12727104 (mapped to FMO4) showed a disproportionately large influence on the overall effect estimate. The FMO is a class of NADPH- and oxygen-dependent metabolizing enzymes, including 6 isoforms, FMO1-6, in humans, which are involved in the oxidative metabolism of drugs and toxicants.53-55 In recent years, FMO has been found to play key roles in tumorigenesis, metastasis, and immune microenvironment regulation.56,57 FMO4 promotes fatty acid oxidation (FAO) and induces M2 tumor-associated macrophage (TAM) polarization by activating the AMPK-ACC1 pathway in hepatocellular carcinoma.
58
By analyzing clinical samples from patients with hepatocellular carcinoma, Luo et al
58
found that high expression of FMO4 correlated with a decrease in CD8+ T-cell infiltration (
Taken together, our MR and annotation results suggested concrete mechanistic hypotheses linking genetic variation to PDAC risk via systemic biomarkers. Specifically, SLC22A4 variations may influence the cellular uptake of redox-active substrates and immune cell function, increasing systemic inflammation and fibrinogen production; FMO4 variation may perturb xenobiotic/lipid metabolism and oxidative stress responses, contributing to renal endothelial/tubular dysfunction (higher UAE) and immunometabolic shifts in the tumor microenvironment. Our MR analyses provided evidence for causal directionality between exposure (fibrinogen/UAE) and PDAC but did not demonstrate the molecular steps—functional follow-up (eQTL/resident-tissue expression, CRISPR perturbation, metabolomics, and immune profiling) that are required to confirm whether the implicated SNPs alter gene expression or protein function in relevant tissues (liver, kidney, pancreas, and immune cells).
Based on these findings, we evaluated the clinical data of patients with benign and malignant pancreatic tumors for fibrinogen levels and urinary protein excretion rate to determine whether these are biomarkers for the prediction and diagnosis of pancreatic cancer and PDAC. The statistical results showed that patients with malignant pancreatic tumors had significantly higher fibrinogen levels and urinary protein excretion rates than those with benign pancreatic tumors. In addition, patients with elevated fibrinogen levels, urinary protein excretion rate, and CA19-9 levels had a worse prognosis than other patients.
Currently, the most common biomarker for detecting pancreatic malignancy and PDAC is CA19-9, which has a sensitivity, specificity, and AUC of 72% (95% CI: 71% to 73%), 86% (95% CI: 85% to 86%), and 0.8474 (95% CI: 0.8227 to 0.8676), respectively, for differentiating between benign and malignant pancreatic disease. 59 When CA19-9 was combined with fibrinogen levels and UAE, the sensitivity, specificity, and AUC for distinguishing benign and malignant pancreatic tumors were 0.818, 0.967, and 0.924, respectively. This combination improved the prediction of pancreatic malignant tumors by 6.36% compared with using CA19-9 alone. Moreover, the positive predictive value of CA19-9 for pancreatic malignant tumors was extremely low (< 1%).60,61 Therefore, the development of novel biomarkers for pancreatic cancer or complementary biomarkers for CA19-9 is crucial. Our findings can assist in establishing evidence for the potential of fibrinogen levels and urinary protein excretion rates as diagnostic and prognostic biomarkers for pancreatic malignancy and PDAC, especially because these 2 metrics complement CA19-9 to greatly enhance the prediction of pancreatic malignancy.
Although this study validated the potential role of fibrinogen levels and UAE in pancreatic cancer through an MR analysis and clinical data, some limitations remain. First, the existing GWAS cohort for pancreatic cancer had a limited sample size, which might have affected the statistical power and reliability of the results. A population overlap may exist between exposure and outcome, leading to biased results. Second, horizontal pleiotropy was observed in MR analyses when using the validation data set. Despite the use of the MRPRESSO and MR-Egger methods to assess and correct horizontal pleiotropy, undetected horizontal pleiotropy may have still occurred. Third, MR analyses can only confirm the direction of the association and cannot provide quantitative causal effects. Additional quantitative studies are required to validate these associations. Fourth, the results were limited to a European population; therefore, the findings may not apply to other ethnic groups. Genetic backgrounds and environmental factors may lead to different results in different ethnic groups. Fifth, several statistical methods (eg, weighted median, MR-Egger, and IVW methods) were used, each with its own strengths and weaknesses, which may affect the interpretation of the results. Cochran’s Q test and MR-Egger intercept analysis were used to assess heterogeneity and horizontal multiplicity; however, the statistical power of the tests for these methods may be limited, especially in the case of small sample sizes. Sixth, clinical data were obtained from patients with pancreatic cancer at Peking Union Medical College Hospital from 2019 to 2024, which may introduce selection bias, and long-term follow-up data are lacking, which may affect the assessment of prognostic indicators. Seventh, the sample size was not calculated in accordance with the standards developed by Zhang and Hartmann, and the limited sample size may have affected the statistical significance of the results.
Beyond supporting a causal role in PDAC, our findings highlighted the potential translational applications of fibrinogen and UAE. Fibrinogen is routinely measured in clinical practice, and elevated levels may not only reflect systemic inflammation but also serve as a prognostic marker of tumor aggressiveness, response to therapy, and the risk of thromboembolic complications in patients with PDAC. The UAE, a marker of renal endothelial dysfunction and metabolic stress, could provide additional prognostic information by identifying subgroups of patients with higher systemic metabolic burden, and potentially worse outcomes. In combination with established markers such as CA19-9, both fibrinogen and UAE may contribute to a more refined risk stratification, early identification of high-risk individuals, and monitoring of treatment response. These findings suggest that integrating genetically informed biomarkers into clinical workflows could improve PDAC management and prognosis; however, further validation in prospective clinical cohorts is required.
Conclusion
This study demonstrated the potential of fibrinogen level and UAE as biomarkers of pancreatic malignancy through MR analysis and clinical data validation. These metrics significantly improved the prediction of pancreatic cancer when used in combination with CA19-9 levels. In addition, this study proposes a potential mechanism for fibrinogen levels and urinary protein excretion rate in PDAC involving SLC22A4 and FMO4.
Supplemental Material
sj-tif-1-onc-10.1177_11795549251392490 – Supplemental material for Proposing an Optimized Prediction Model for Pancreatic Cancer Based on Mendelian Randomization Analysis of Fibrinogen Levels and Urinary Protein Excretion Rate
Supplemental material, sj-tif-1-onc-10.1177_11795549251392490 for Proposing an Optimized Prediction Model for Pancreatic Cancer Based on Mendelian Randomization Analysis of Fibrinogen Levels and Urinary Protein Excretion Rate by Qian Wu, Mengqing Sun, Yan Lin, Shujin Lin, Ting Lin, Xiao Han and Xianlin Han in Clinical Medicine Insights: Oncology
Supplemental Material
sj-tif-2-onc-10.1177_11795549251392490 – Supplemental material for Proposing an Optimized Prediction Model for Pancreatic Cancer Based on Mendelian Randomization Analysis of Fibrinogen Levels and Urinary Protein Excretion Rate
Supplemental material, sj-tif-2-onc-10.1177_11795549251392490 for Proposing an Optimized Prediction Model for Pancreatic Cancer Based on Mendelian Randomization Analysis of Fibrinogen Levels and Urinary Protein Excretion Rate by Qian Wu, Mengqing Sun, Yan Lin, Shujin Lin, Ting Lin, Xiao Han and Xianlin Han in Clinical Medicine Insights: Oncology
Supplemental Material
sj-tif-3-onc-10.1177_11795549251392490 – Supplemental material for Proposing an Optimized Prediction Model for Pancreatic Cancer Based on Mendelian Randomization Analysis of Fibrinogen Levels and Urinary Protein Excretion Rate
Supplemental material, sj-tif-3-onc-10.1177_11795549251392490 for Proposing an Optimized Prediction Model for Pancreatic Cancer Based on Mendelian Randomization Analysis of Fibrinogen Levels and Urinary Protein Excretion Rate by Qian Wu, Mengqing Sun, Yan Lin, Shujin Lin, Ting Lin, Xiao Han and Xianlin Han in Clinical Medicine Insights: Oncology
Footnotes
Acknowledgements
N/A.

Ethical considerations
This study was approved by the Ethics Committee of Peking Union Medical College Hospital (PUMCH), Chinese Academy of Medical Sciences, under approval number I-24PJ1452 on July 12, 2024. The study included information on deceased participants, which was used with the explicit consent of legally authorized representatives (LARs). All participants (including LARs of the deceased participants) or their legal representatives provided written informed consent to participate in the study and agreed to its publication.
Author contributions
Qian Wu, Mengqing Sun, Xiao Han, PhD, and Xianlin Han, MD, conceived and designed the work on this topic and contributed substantially to the acquisition, analysis, and interpretation of the data. Qian Wu and Mengqing Sun drafted the article. Yan Lin, Shujin Lin, and Ting Lin performed the data analysis and experiments. All listed authors contributed to the conception, design, collection, analysis, or interpretation of the data and contributed to the writing and intellectual content of the article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by funds from the National High-Level Hospital Clinical Research Funding No. 2022-PUMCH-B-003; the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (CAMS) Initiative for Innovative Medicine Grant No. 2021-I2M-1-022; and the Natural Science Foundation of Fujian Province (2023J01411).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting this study are openly available from the EMBL-EBI (https://www.ebi.ac.uk/) and FinnGen databases (![]() ).
).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.