
Abstract
Keywords
Introduction
Delaying progression of disability is a key therapeutic goal of disease-modifying therapy (DMT) in patients with multiple sclerosis (MS).1,2 Multiple outcome measures have been developed to assess disease progression or patient function in clinical studies of patients with MS. The Expanded Disability Status Scale (EDSS) is the most established outcome measure in MS clinical trials.3,4 The EDSS has notable limitations, particularly with regard to insensitivity in upper extremity function and non-motor functions once ambulation is severely restricted.2,5–7 Additionally, it does not provide an adequate assessment of cognitive impairment related to MS. 6
The Multiple Sclerosis Functional Composite (MSFC), developed to overcome some of the limitations of the EDSS, comprises three components that evaluate different patient functional outcomes: the Timed 25-Foot Walk (T25FW) for ambulation, the 9-Hole Peg Test (9HPT) for hand/arm dexterity, and the 3-Second Paced Auditory Serial Addition Test (PASAT-3) for cognition.
7
Because clinical interpretation of the composite
DECIDE (NCT01064401) was a phase 3 study that evaluated the efficacy and safety of treatment with daclizumab beta 150 mg subcutaneous once every 4 weeks versus interferon (IFN) beta-1a 30 mcg intramuscular (IM) once weekly in patients with relapsing-remitting MS (RRMS).
13
Daclizumab beta (formerly known as daclizumab high-yield process) was approved as ZINBRYTA®, which has a different form and structure than an earlier form of daclizumab. In the overall study population, daclizumab beta demonstrated greater benefit compared with IM IFN beta-1a on several outcome measures of disability. While 12-week confirmed disability progression (CDP) as assessed by EDSS did not differ significantly between the two treatment groups, 24-week CDP, a more robust outcome than 12-week CDP, was reduced by 27% in patients treated with daclizumab beta versus IM IFN beta-1a (
In addition to demonstrating efficacy of an MS therapy in the overall study population, subgroup analyses may inform on treatment effects across different demographic and clinical characteristics.15,16 This post hoc analysis examined treatment effects of daclizumab beta compared with IM IFN beta-1a on measures of patient disability or impairment across patient subgroups according to baseline demographic and disease characteristics in DECIDE. The measures included a modified MSFC, in which the PASAT-3 was replaced with the SDMT.
Methods
Full details of DECIDE have been reported. 13 Briefly, patients of age 18–55 years with a confirmed diagnosis of RRMS were randomized (1:1) to daclizumab beta 150 mg subcutaneous every 4 weeks and IM placebo once weekly or IFN beta-1a 30 mcg IM once weekly and subcutaneous placebo every 4 weeks for a minimum of 96 weeks and up to 144 weeks. Magnetic resonance imaging (MRI) consistent with MS, baseline EDSS score of 0–5.0, and two or more relapses within the previous 3 years (one or more in year before study) or one or more relapse(s) and one or more new MRI lesion(s) within 2 years (one or more event(s) in year before study) constituted additional inclusion criteria. All patients provided written informed consent. Central and local ethics committee approvals were obtained, and the study was performed in accordance with the Declaration of Helsinki and the International Conference on Harmonisation Guidelines for Good Clinical Practice. 17
Assessments
Three outcome measures of patient disability/function were examined for the overall study population and by subgroup. These included 24-week CDP as measured by EDSS 18 (tertiary endpoint in DECIDE), 24-week sustained worsening on the MSFCS (analysis performed post hoc), and the proportion of patients experiencing a clinically meaningful worsening in MSIS-29 PHYS score at week 96 (secondary endpoint in DECIDE). Twenty-four-week CDP was defined as an increase in the EDSS score of ⩾1.0 point(s) from a baseline score of ⩾1.0 or ⩾1.5 points from a baseline score of 0 confirmed after 24 weeks. 13 Twenty-four-week sustained worsening on the MSFCS, based in part on an analysis by Rudick et al., 8 was defined as ⩾20% worsening in T25FW score, ⩾20% worsening in 9HPT score (mean of both hands), or a decrease of ⩾4 points in SDMT score (clinically meaningful change) 19 sustained for 24 weeks. Additional analyses were run using alternative methods for evaluating 9HPT. These included examining a 20% worsening in 9HPT score for the dominant hand only or for either the dominant hand or the non-dominant hand. Finally, in order to capture clinically meaningful changes due to MS from the patents’ perspective, worsening from baseline in MSIS-29 PHYS score was analyzed at week 96. An increase from baseline on the MSIS-29 of ⩾7.5 points has been shown to indicate clinically meaningful worsening in a large clinical study population. 20
EDSS, T25FW, and 9HPT scores were assessed at baseline and every 12 weeks until week 144 (or end of study). SDMT (oral response format) and MSIS-29 (version 1) scores were assessed at baseline and every 24 weeks until week 144 or end of study.
Subgroups based on baseline demographics were age (⩽35, >35 years) and sex (female, male). Subgroups based on baseline disease characteristics were disability as defined by EDSS score (<3.5, ⩾3.5), relapses in previous 12 months (one or less, two or more), disease duration (<3, ⩾3 to <10, or ⩾10 years), gadolinium-enhancing (Gd+) lesions (absent, present), T2 hyperintense lesion volume (<, ⩾ median), disease activity (highly active, less active; highly active was defined as two or more relapses in the year before randomization and one or more Gd+ lesion(s) on baseline MRI, less active otherwise), prior DMT use (yes, no; excluding steroids but including any prior disease-modifying or immunomodulatory therapy for MS, such as alemtuzumab, azathioprine, cladribine, cyclophosphamide, fingolimod, fumaric acid, glatiramer acetate, immune globulin, IFN beta-1a, IFN beta-1b, laquinimod, methotrexate, mitoxantrone, mycophenolic acid, natalizumab, teriflunomide, or temsirolimus), and prior IFN beta use (yes, no; including IFN beta, IFN beta-1a, and IFN beta-1b).
Statistical analyses
All analyses were performed on the intention-to-treat population (randomized patients who received one or more dose(s) of study drug) with non-missing baseline assessments.
13
MSFCS progression was analyzed by Cox proportional hazards model adjusted for prior IFN beta use (yes, no) and baseline age (⩽35, >35 years), excluding covariates defining the subgroup. Patients with a tentative progression at the end of treatment period visit and no confirmation assessment were censored at their last assessment. Data were re-censored at 2 years, that is, 96 weeks. Missing T25FW and 9HPT data were imputed using the method described in the supplemental material of Kappos et al. 13 Missing SDMT values in post-baseline visits were imputed using last observation carried forward. For patients with missing SDMT values, the other endpoints were used to derive time to first sustained progression.
Analyses of patients with a clinically meaningful worsening in MSIS-29 PHYS score were based on logistic regression models, adjusted for baseline MSIS-29 PHYS score, baseline Beck Depression Inventory-II score, prior IFN beta use, and baseline age (⩽35, >35 years), but excluded covariates defining the subgroup. If a patient was missing data for <10 of the 20 items that make up the PHYS score, then the mean of the non-missing items was used for the missing items. If the patient was missing ⩾10 of the 20 items that make up the PHYS score, or missing the questionnaire entirely, or if the questionnaire was completed after the patient switched to alternative MS medication, a random effects model was used to estimate MSIS-29 PHYS score.
Results
The intention-to-treat population of DECIDE included 1841 patients; 922 were randomized to IM IFN beta-1a and 919 were randomized to daclizumab beta. 13 Details of the demographics and baseline characteristics of the DECIDE study population are published. 13 Relevant demographics and baseline characteristics are shown in Table 1.
Patient demographics and baseline disease characteristics in DECIDE.

IM: intramuscular; IFN: interferon; SD: standard deviation; MS: multiple sclerosis; EDSS: Expanded Disability Status Scale; SDMT: Symbol Digit Modalities Test; MSIS-29: 29-Item Multiple Sclerosis Impact Scale; PHYS: physical impact subscale; PSYCH: psychological impact subscale; MSFC: multiple sclerosis functional composite; T25FW: Timed 25-Foot Walk; 9HPT: 9-Hole Peg Test; PASAT-3: 3-Second Paced Auditory Serial Addition Test.
Daclizumab beta, n = 918.
IM IFN beta-1a, n = 880; daclizumab beta, n = 884.
IM IFN beta-1a, n = 912; daclizumab beta, n = 906.
IM IFN beta-1a, n = 912; daclizumab beta, n = 904.
IM IFN beta-1a, n = 920; daclizumab beta, n = 916.
Twenty-four-week CDP
Across all subgroups, point estimates of the risk of 24-week CDP showed consistent trends favoring daclizumab beta over IM IFN beta-1a (Figure 1) and supported the results observed for 24-week CDP in the overall study population. 13 For this outcome measure, minor variations in treatment effect estimates were observed and there was no convincing evidence of effect modification. HRs ranged from 0.46 to 0.87, where the greatest risk reduction was observed in patients ⩽35 years of age.
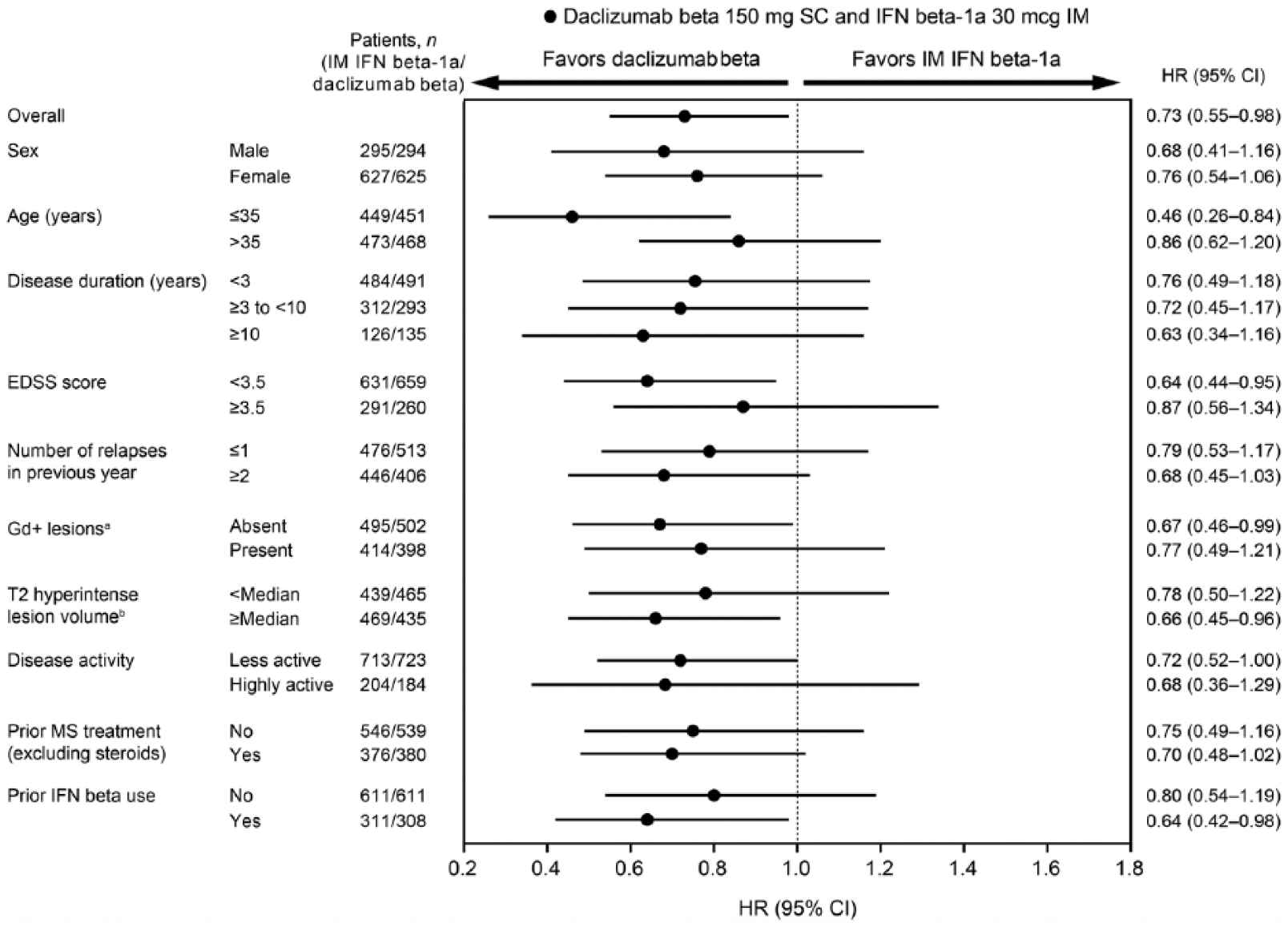
Forest plot for 24-week confirmed disability progression for daclizumab beta versus IM IFN beta-1a by baseline demographics and disease characteristics.
Twenty-four-week sustained MSFCS progression
Fewer daclizumab beta (24% (224/919)) versus IM IFN beta-1a patients (28% (259/922)) met the criteria for 24-week sustained MSFCS progression at week 96. Of patients who progressed, MSFCS progression was most commonly driven by SDMT (IM IFN beta-1a, 56% (146/259); daclizumab beta, 55% (124/224)), followed by T25FW (IM IFN beta-1a, 34% (89/259); daclizumab beta, 33% (75/224)) and 9HPT scores (IM IFN beta-1a, 6% (16/259); daclizumab beta, 8% (17/224)). The rest of the patients progressed on two or more components at the same time. In the overall study population, treatment with daclizumab beta resulted in a 20% reduction (HR, 0.80; 95% CI, 0.67–0.95;

Forest plot for 24-week sustained modified Multiple Sclerosis Functional Composite progression for daclizumab beta versus IM IFN beta-1a by baseline demographics and disease characteristics.
Clinically meaningful worsening in MSIS-29 PHYS score
Treatment with daclizumab beta resulted in a 24% reduction in the odds of a clinically meaningful worsening in MSIS-29 PHYS score at week 96 versus IM IFN beta-1a (OR, 0.76; 95% CI, 0.60–0.95;

Forest plot for proportion of patients with clinically meaningful worsening in 29-Item Multiple Sclerosis Impact Scale physical impact subscale score at week 96 for daclizumab beta versus IM IFN beta-1a by baseline demographics and disease characteristics.
Discussion
In the overall study population of DECIDE, treatment with daclizumab beta resulted in significant reductions in risk of 24-week CDP as measured using the EDSS, and risk of 24-week sustained progression on the MSFCS, a version of the MSFC replacing the PASAT-3 with the SDMT. Additionally, patients receiving daclizumab beta had reduced risk of experiencing a clinically meaningful worsening in MSIS-29 PHYS score compared with IM IFN beta-1a. Daclizumab beta treatment also showed consistent benefit versus IM IFN beta-1a across multiple patient subgroups, thus supporting the treatment effect seen in the overall population for each of the outcome measures examined independent of baseline characteristics. Treatment effect did not reach statistical significance for all subgroups for any of the three outcome measures, however, age ⩽ 35 years and baseline T2 hyperintense lesion volume ⩾median reached nominal significance for all three measures.
In this study, daclizumab beta demonstrated greater efficacy versus IM IFN beta-1a on two distinct measures of disability progression, 24-week CDP as measured by EDSS and the MSFCS. Despite its wide use, the EDSS has been criticized for a lack of sensitivity to change and inadequate assessment of cognition.5,22 The MSFC was developed to address these limitations and provide information supplemental to that provided by the EDSS. 7 Both a 15% and a 20% worsening from baseline in at least one MSFC component (sustained for 3 months) were found to be sensitive measures of disability progression. 8
This study examined MSFCS progression sustained for 6 months, which is considered more robust than the 3-month interval and is recommended by the European Medicines Agency when examining CDP.2,23 This study also explored three methodologies for the 9HPT component of the MSFCS: mean of both hands, dominant hand only, and either the dominant or non-dominant hand. The results of this MSFCS analysis did not appear to be impacted by choice of methodology.
Rudick et al. reported that, of patients who progressed on the MSFCS using a 20% worsening, the majority of patients progressed first on the T25FW (51% of placebo and 54% of natalizumab), while few patients progressed first on the PASAT-3 (5% of placebo and 6% of natalizumab). 8 In contrast, the present analysis found that the majority of the patients with MSFCS progression worsened first on the SDMT, suggesting that the SDMT has potentially greater sensitivity compared with the PASAT-3 in detecting cognitive decline.
In contrast to the EDSS and MSFC, which are clinical assessment measures administered by physicians or trained professionals, the patient-reported MSIS-29 was developed as a disease-specific tool meant to capture the impact of MS from the perspective of the patient. 24 Point estimates from the subgroup analyses of the proportion of patients with clinically meaningful worsening in the MSIS-29 PHYS consistently favored daclizumab beta versus IM IFN beta-1a.
These analyses should be interpreted as exploratory and hypothesis generating for future studies. Some subgroups had small sample sizes, which resulted in wider CIs for these subgroups. 15 Additionally, no adjustments were made for multiple testing. Inherent differences in the properties of the tools (e.g. clinician-administered vs patient-reported) and the different functions assessed by each also may contribute to the differences observed across them. 25
Overall, the results of these post hoc subgroup analyses of outcome measures assessing disability progression, as well as patient-reported function, indicate that the efficacy of daclizumab beta treatment compared with IM IFN beta-1a was superior and consistent across a range of baseline demographic and disease characteristics in patients with RRMS in DECIDE.
Footnotes
Declaration of Conflicting Interests
Funding
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.