
Abstract
Introduction
Motor neuron disease (MND) is a neurodegenerative disorder which leads to progressive muscle weakness and respiratory compromise due to loss of motor neurons in the brain, brainstem and spinal cord.1–3 The typical age of onset is in the mid-late 50s and there is a slight male predominance with males twice as likely to be affected. Survival is approximately 3–5 years after diagnosis with the most common cause of death being due to respiratory failure.1–4 The estimated incidence of MND in the United Kingdom is 2.76 per 100,000. 5 The only approved drug for MND is riluzole which works by slowing disease progression and has been demonstrated to prolong survival by 2–3 months. 6 The phenotypical subtypes of MND are based on the affected area of disease onset and include limb and bulbar onset.
Regardless of the site of onset however, respiratory muscle dysfunction is a key clinical aspect of MND and declines as the disease progresses. Many patients already show evidence of pulmonary function impairment at the time of diagnosis. 7 Symptoms due to respiratory muscle involvement include dyspnoea and nocturnal hypoventilation which can lead to morning headaches, orthopnoea, poor concentration, unrefreshing sleep, fatigue and daytime somnolence with a resulting negative impact on the patients’ quality of life.7–10 The introduction of non-invasive ventilation (NIV) may help alleviate these symptoms and has been shown to improve quality of life, survival and slow the rate of pulmonary functional decline in numerous studies.6,10,11–17 Non-invasive positive pressure ventilation is the most commonly used form of NIV in MND as it most closely replicates physiological conditions, reduces symptoms, improves sleep quality and gas exchange.18–20
There is a paucity of clear guidance outlining the optimal time-point in the course of the disease, at which to initiate NIV, but small studies suggest that the earlier NIV is initiated the better the outcome for the patient, in terms of survival and quality of life.6,11,21–23 Other important aspects to consider are tolerance and compliance with NIV once it has been established, with studies showing that the use of NIV for more than 4 hours a day has the greatest potential for long-term benefit.6,7,11,12,17 It has previously been shown that bulbar onset MND can lead to poorer compliance with NIV and therefore this cohort of patients do not get the same benefit in terms of survival and quality of life improvements. 7
In terms of markers of pulmonary function decline, sniff nasal inspiratory pressure (SNIP) has been found to correlate well with transdiaphragmatic pressures and has demonstrated an ability to predict respiratory muscle function as it linearly declines with disease progression.24–28 SNIP can be performed more easily than spirometry, in patients with advanced disease and is a reliable predictor of mortality and is a better indicator of early respiratory muscle dysfunction than forced vital capacity (FVC).24–28 Furthermore, its measurement does not require a tight mouth seal which may not be possible for many patients with bulbar onset MND. 25
In this study, we aimed to review data on MND patients who attended a multidisciplinary MND clinic between September 2014 and September 2019 at our institution; a tertiary-referral, academic, teaching hospital to determine whether the use of NIV had any survival advantage in this patient cohort.
Materials and methods
A retrospective chart analysis of all patients who attended a multidisciplinary MND clinic at our institution from September 2014 to September 2019 was performed. All charts of those attending this clinic were reviewed. Patients who did not have a definite or probable diagnosis of MND were excluded. Patients who had not yet been set up on NIV at the time of study commencement were also excluded, as were those who died or failed to attend clinic after their diagnosis to discuss the use of NIV. This resulted in the inclusion of
Data collected from the patient’s chart included basic patient demographics, the use of NIV, age at diagnosis and type of MND, that is, bulbar or limb onset MND. Data on compliance with NIV was obtained both from compliance records in the patient’s charts and through the ResMed online system who provided the majority of NIV machines to this cohort of patients. Optimal use of NIV was defined as use of the machine for greater than 4 hours per day and for greater than 70% of the days used. Increased patient reliance on NIV with disease progression is typical in MND. Therefore, it was felt that patients who demonstrated initial compliance within 3 months of commencing NIV would probably demonstrate good levels of compliance throughout the clinical course of their disease. Survival (in months) was defined as the time from MND diagnosis to patient death, or if patient was still alive then time from diagnosis to their last clinic attendance until a cut-off point of January 2020 when data collection was completed.
Pulmonary Function Test (PFT) results were also collected from the patient records. We aimed to collect FVC, peak cough flow (PCF) and SNIP results both at diagnosis and at time of commencing NIV. The use of riluzole and the use of a cough assist machine were also recorded as was the location of NIV set up.
All patients attending the clinic are offered NIV as soon as possible after diagnosis is confirmed either as an inpatient or at home. The preferred method at our institution is inpatient set up within the hospital. During this time, the patient is assessed by the multidisciplinary team, PFTs are performed and NIV is set up and trialled. The machine utilised for in-patient set up is the same machine the patient is discharged home with for their ongoing use.
Statistical analysis
Descriptive statistics were used to analyse patient characteristics. Normally distributed continuous data was described using means and standard deviations(SD). The categorical variables were reported in percentages of total subjects. Patient characteristics were compared using independent sample t tests for continuous variables and Pearson’s χ2 test for categorical variables. Kaplan–Meier method was used to plot survival distributions. We performed statistical analyses for the full study cohort (all phenotypes), followed by a subgroup analysis with patients grouped according to their clinical phenotype. A
Ethical approval for this study was granted by the Cork Research Ethics Committee, Cork Ireland.
Results
Demographics
Patient demographics. Column one shows cumulative data from all patients included in the study (

Abbreviations: MND, Motor neuron disease; NIV, non-invasive ventilation; PEG, percutaneous endoscopic gastrostomy: IPAP, inspiratory positive airway pressure: EPAP, expiratory positive airway pressure.
Non-invasive ventilation
In the total population, 80.2% of patients trialled NIV while 66.7% maintained use. 73.7% of the bulbar MND group continued using NIV and 61.8% in the limb onset MND group continued with NIV. Optimal use of NIV, defined as use for more than 70% of days and for greater than 4 hours per day was observed in 44.1% of the 66.7% of patients who continued using NIV. Those with bulbar onset MND were more compliant and had better usage when compared to those with limb onset MND (55.3% vs 36.4%,
Pulmonary function tests
PFTs at diagnosis were not available for all patients with only 78 patients having an FVC value recorded around the time of diagnosis. The mean FVC at diagnosis for the whole group was 78.7% predicted. Those with bulbar onset MND had an average FVC of 73.13% predicted while the FVC for the limb group at diagnosis at 82.64% predicted. However, there was a statistically significant difference between mean SNIP values at diagnosis for those with bulbar onset MND (35.85% predicted) compared with those with limb onset MND (52.98% predicted, Decline in SNIP and PCF values 3, 6, 9 and 12 months prior to death. This data was available on 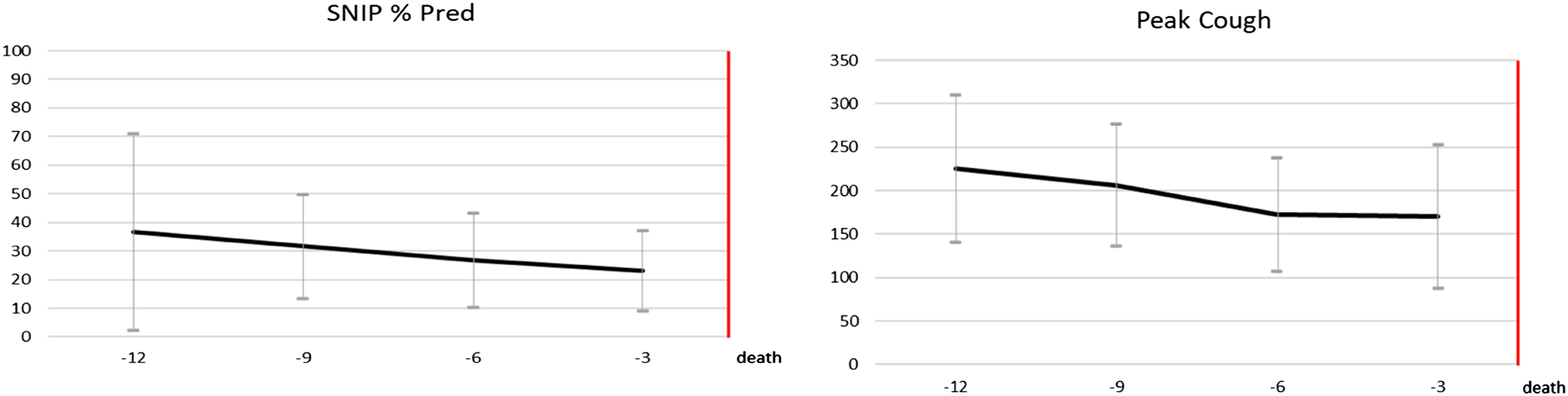
Survival
Overall survival was 26 months from the date of MND diagnosis. Survival was significantly longer in the limb MND group regardless as to whether patients used NIV or attained compliance when compared with those with bulbar MND (33 months vs 17 months, Survival curves. a - compares overall survival for those with limb onset disease versus those with bulbar onset disease with a statistically significant longer survival seen in those with limb onset MND, Comparison of data for those who were given NIV regardless of if they achieved compliance or not versus those who never used NIV. Those who used NIV had a statistically significant longer survival than those who never used NIV, Abbreviations: NIV, non-invasive ventilation; PEG, percutaneous endoscopic gastrostomy: ITT intention to treat. Those who used NIV optimally, as defined by use for more than 4 h per day and for more than 70% of the time were compared with those who did not use NIV. Particular attention should be paid to the survival data when these two groups are compared. Abbreviations: NIV, non-invasive ventilation.


NIV set up
Location of NIV set up, that is, home versus in hospital set up and associated compliance.

Discussion
This study of MND patients attending a multidisciplinary clinic found that 66.7% of the patient cohort were treated with NIV and of this 66.7%, 44.1% used NIV optimally. Optimal use of NIV was taken as use for >4 h/day for over 70% of the time used within 3 months of commencing use of the machine. It has been shown in previous studies that better compliance and longer use of the machine is associated with prolonged survival with Piepers et al. 2006 and Bourke et al. 2003, both showing that survival improved with better compliance compared to those who did not tolerate or did not use NIV, while Kleopa et al. 1999 showed that those who used NIV for four or more hours per day survived longer than those who did not use NIV.7,12,17 It was noted on observation that those who used the machine well initially continued to use the machine optimally as disease progressed. Only nine patients who initially were not compliance then later became more compliant on the machine. How improved compliance in this small group of patients affected survival was not further explored in this study. When those with bulbar onset MND were compared with those with limb onset MND, the bulbar MND group had better compliance and better machine usage. This may be due to poorer respiratory function and a greater need for NIV amongst the bulbar group. Review of the literature shows varying results regarding compliance and tolerance of NIV in those with bulbar MND with some finding that those with bulbar onset MND had a decreased benefit due to intolerance and that NIV was difficult to establish in bulbar MND.7,16 In contrast, other studies have found that the area of MND onset did not affect tolerance. 12 There was a low level of compliance among the study cohort. Factors which may contribute to this are that often only one compliance data set was available for a patient. However, as previously noted, we observed that in general if a patient was tolerant of the machine within 3 months of initiation, they remained compliant throughout the rest of the time using the machine.
In our population cohort, those with limb onset MND survived significantly longer than those with bulbar onset MND (33 months vs 17 months). This is not unexpected as bulbar onset MND is known to have a worse prognosis.
29
There was a statistically significant longer survival in those who used NIV compared to those who never used NIV (28 months vs 12 months). This is in keeping with multiple studies including the only randomised control trial on this topic by Bourke et al. 2006 7,12–17,21,30 Furthermore, there was significantly longer survival in those who used NIV optimally compared with those who never used NIV. This survival advantage has been previously demonstrated in several studies.7,15,31,32 Of additional interest, those who used NIV regardless of compliance and pattern of onset survived 2 months longer on average than those who optimally used NIV. This may be as a consequence of having smaller patient numbers in the optimal use NIV group (
This study also found that those with bulbar onset MND have more marked impairment in PFT measurements at diagnosis compared to those with limb onset MND, with SNIP and PCF values being statistically significant lower in those with bulbar onset MND. This highlights a worse overall prognosis of bulbar onset MND when compared with limb onset MND. It has long been established that the rate of decline of respiratory function is related to mortality. We have shown in this study that the SNIP and PCF values declined significantly between diagnosis and values recorded within 6 months of death. SNIP measurements can better predict respiratory muscle function as they linearly decline with disease progression, can better perform in advanced disease and are a reliable predictor of mortality and can better indicate earlier respiratory muscle dysfunction than FVC.24–28 Figure 2 highlights the gradual decline of SNIP and PCF in the year before death of all patients for which this data was available. It could be concluded from this that serial SNIP and PCF measurements, as is carried out in our centre, are an accurate measure of respiratory muscle decline and can help predict mortality.
There is a lack of data regarding the best location for NIV set up for MND patients. As mentioned, our institute aims to set up NIV while the patient is in hospital so that nursing and physiotherapy staff can help with mask adjustment and therefore improve compliance. Although 70% of the patients for which this data was available had their NIV set up while in hospital, compliance amongst this group was lower compared with those set up at home. There may be several reasons for this including that those who are able to be set up at home may have less severe phenotypes and/or may be more willing to embrace the intervention. More research is required in this area, but it is a unique data point to our current study.
Advantages and limitations
One of the limitations of this study was that it was a retrospective study performed over a 5-year period and therefore it was not possible to standardise data collection of each patient. Practise in the clinic changed significantly during this time which influenced the data available. As the clinic became established a physiotherapist, speech and language therapist, neurology consultant and respiratory consultant saw the patient on every visit. This meant that compliance data was analysed and recorded and that the physiotherapist preformed spirometry and recorded SNIP and PCF values at every visit. This was not always the case with earlier clinics which resulted is a lack of PFT data for certain patients. Secondly, in some cases there was missing data especially elements of PFTs. This was due to a combination of factors including lack of availability in the PFT lab, patient difficulty travelling to appointments and patient difficulty carrying out the test. This affected our ability to accurately measure FVC decline over time. A further limitation is that not every patient was set up in NIV in our institute. A subset of patients were set up at other institutes prior to assessment at our institution. This resulted in difficulties retrieving compliance data for some patients. This was particularly the case in earlier clinics, but this issue was subsequently resolved by standardising practice with one primary vendor within the region. Given its observational nature, our study while showing robust associations cannot establish causation, and a variety of factors may have contributed to the observed difference in survival.
One of the main advantages of this study includes the large sample size of 111 patients. This sample is representative of MND patients from all over the south of Ireland. Furthermore, we believe that this is the first study of its kind in an Irish MND population. Another advantage was that there was a high uptake of NIV among our patient cohort with two-thirds of patients who continued to use NIV using it optimally. Finally, we analysed home and inpatient set up in our patient cohort and looked at how this affected compliance which is a factor rarely mentioned in other studies.
Conclusion
This is a retrospective chart analysis of 111 patients who attended a multidisciplinary MND clinic at our institute over a 5-year period. We collected data on NIV usage and compliance as well as PFT results. It was found that there is a statistically significant advantage to using NIV optimally and this was also seen in those with bulbar onset MND who were compliant with NIV compared to those who did not use NIV.