
Abstract
Keywords
Introduction
Erectile dysfunction (ED) is the inability to obtain or maintain sufficient penile rigidity to engage in effective sexual intercourse. It is a prominent cause of sexual dysfunction, impacting hundreds of millions of men worldwide (Ayta et al., 1999). ED is utilized as a potentially beneficial tool in assessing and preventing cardiovascular disease (CVD) (Orimoloye et al., 2019). The two diseases have similar risk factors and may be distinct manifestations of the same pathogenetic pathways of endothelial dysfunction and atherosclerosis (Miner et al., 2014). The research findings indicate that one of the most important factors leading to vascular endothelial dysfunction is systemic inflammatory, which eventually lead to the incidence of ED (Vlachopoulos et al., 2007). Hence, meticulous evaluation of inflammatory biomarkers is crucial in medical practice, providing quantitative measures of disease severity and progression for clinical decision-making. As research progresses, these biomarkers may become pivotal in intervention strategies and therapeutic targets, paving pathways for innovative therapies and treatment optimization.
So far, existing inflammatory biomarkers, including C-reactive protein (CRP), the CRP-to-high-density lipoprotein (HDL) ratio, and the neutrophil-to-lymphocyte ratio (NLR), have exhibited robust correlations with ED (Jamaluddin et al., 2019; C. Liu et al., 2023; Mei et al., 2024). The hemoglobin-to-red blood cell distribution width ratio (HRR), derived by dividing hemoglobin (Hb) concentration by the red blood cell distribution width (RDW), has been introduced as a novel inflammatory marker by Sun et al. (2016). Low HRR levels have been linked to a variety of negative outcomes, including stroke (Xiong et al., 2024), depression in older adults (Xi et al., 2024), cancer (Coradduzza et al., 2023), heart failure (Rahamim et al., 2022) and also frailty patients with coronary heart disease (CHD) (Qu et al., 2021), according to research.
Hemoglobin, one of the most critical indicators in red blood cells, reflects both oxygen-carrying capacity and the severity of anemia. RDW is a routine component of the complete blood count, specifically measuring the variation in size of peripheral red blood cells. As a nonspecific biomarker associated with various pathophysiological states, RDW serves as a prognostic indicator for adverse clinical outcomes (Salvagno et al., 2015). Although several well-established markers can directly detect inflammation, HRR integrates information on both anemia and erythrocyte heterogeneity. Anemia can elevate levels of inflammatory mediators, while an increased RDW reflects processes such as chronic inflammation and oxidative stress, which likewise impair endothelial function, lead to arterial dysfunction, compromise blood supply, and may thereby contribute to ED (Salvagno et al., 2015; Vlachopoulos et al., 2007). Inflammation ultimately affects blood flow and function by damaging vascular endothelium, elevating inflammatory cytokines, and increasing oxidative stress, culminating in ED (H. Liu et al., 2024). Both hemoglobin and RDW are widely used, cost-effective clinical markers readily obtained from a complete blood count, making HRR a novel and economical composite indicator of inflammation.
As a novel inflammatory marker, the relationship between HRR and ED remains unclear. Therefore, the purpose of our study was to look into the relationship between ED and HRR in the US population. We argue that this marker may have clinical utility in evaluating ED risk and directing early therapies meant to preserve men’s sexual health, based on our hypothesis that a higher HRR is inversely linked with the risk of ED.
Materials and Methods
Data Resource and Study Population
The National Health and Nutrition Examination Survey (NHANES) database provided the data for this cross-sectional investigation. A range of data modules, such as surveys, laboratory testing, examinations, dietary patterns, and demographics, make up the NHANES database. Furthermore, the studies involving human subjects were evaluated and authorized by the National Center for Health Statistics (NCHS) Research Ethics Review Committee. The public can see all of the NHANES research designs and data in detail at www.cdc.gov/nchs/nhanes/.
Exposure and Outcome Variables
HRR is a biomarker for inflammation that is calculated by dividing the Hb concentration by the RDW, which is expressed in g/dL. ED was the outcome variable. Participants were asked about their capacity to maintain an erection in the questionnaire data module. Following a response of “Sometimes able” or “Never able,” participants were placed in the ED group. Participants who were “Never able” to maintain an erection were selected to further define severe ED.
Covariates
Aside from the outcome and exposure factors, the other variables acted as covariates. Certain factors were considered as categorical variables. Age was divided into two subgroups: <60 years and 60 years and above. The body mass index (BMI) was divided into three subgroups: <25, 25–29.99, and ≥30 kg/m2. The education level was classified as high school or lower and university or higher. Race/ethnicity was classified as Mexican American, non-Hispanic White, non-Hispanic Black, Other Hispanic, and other races. Marital status is divided into two categories: married or living with a partner, and single, divorced, or widowed. Diabetes, hypertension, smoking status, alcohol consumption, and CVD histories were classified as yes or no based on questionnaire replies. The questionnaire divided physical activity into three categories: inactive, moderate, and vigorous. CVD was also diagnosed based on a history of congestive heart failure, CHD, angina, or a heart attack. Detailed measurement protocols for these variables are available at www.cdc.gov/nchs/nhanes/.
Statistical Analyses
Continuous data were reported as means ±
Results
Baseline Characteristics of Study Participants
In all, 2,197 people were chosen to take part in this study after the inclusion and exclusion criteria were applied to the participants from 2001 to 2004 (Figure 1). Of these, 725 said they had ED. Individuals with ED were more probable to be older, non-Hispanic White, and have an education level of high school or below, have lower PIR, be Never or Former drinkers, married/Living with a partner, have a BMI of 30 or above, be smokers, an elevated risk of diabetes, CVD and hypertension, and have lower HRR levels than those without ED. Additional baseline data is available in Table 1.
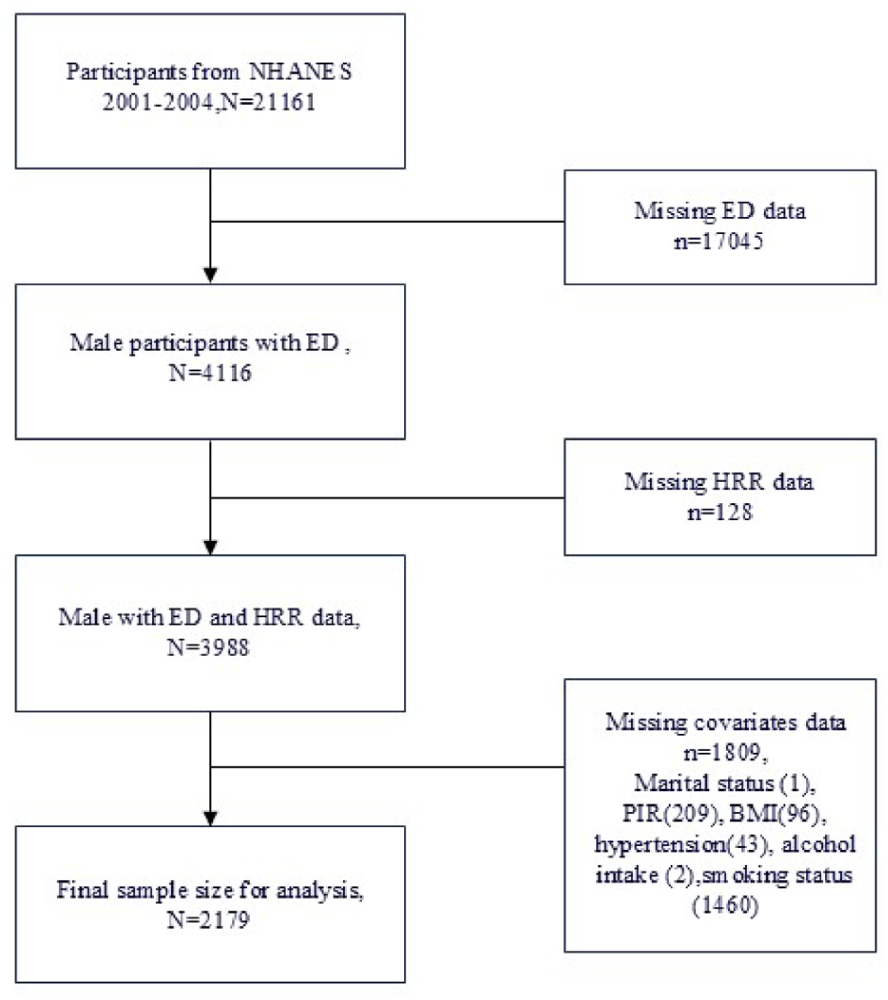
Flowchart of the Sample Selection From NHANES 2001–2004.
Baseline Characteristics of the Study Participants From NHANES 2001–2004, Weighted.

Continuous variables are expressed as weighted means ± standard errors and compared using weighted linear regression. Categorical variables are presented as weighted percentages and 95% confidence intervals, with group comparisons performed using weighted chi-square tests. All
Values with
The Association Between HRR and ED
Table 2 shows the connection between HRR and ED. The findings show a strong relationship between HRR and the occurrence of ED. (Model 1:
Multivariable Logistic Regression Analysis of the Association Between HRR and ED, Weighted.

Values with

Restricted Cubic Spline Fitting for the Association Between HRR and ED.
Analysis and Interaction of Subgroups
Subgroup analyses and interaction tests were used to look into any potential association between HRR and ED (Figure 3). It showed most subgroups had a significant decrease in the risk of ED. It is worth noting that the connection between HRR and ED was more pronounced in the subgroup of participants over the age of 60, no smoking, without diabetes and CVD, drank alcohol, were BMI <25 kg/m2, and had hypertension (all
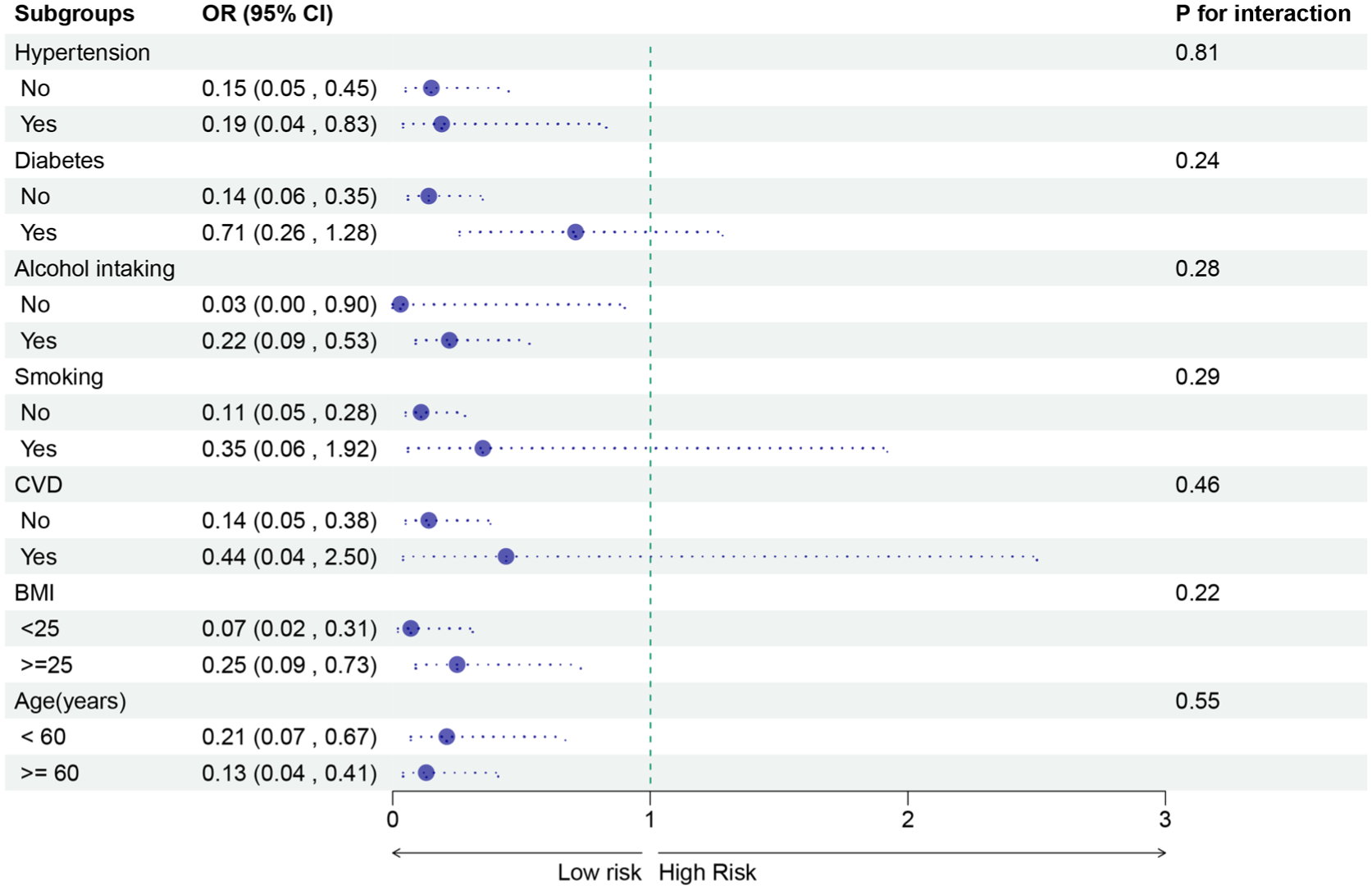
Subgroups Analysis for the Associations Between HHR and ED.
Mediation Analyses
To determine whether BRI mediates the link between HRR and ED, this study constructed a mediation analysis model. The independent variable in this mediation model was HRR, the dependent variable was ED, and the mediator was BRI. Figure 4 illustrates how BRI levels significantly mediated the relationship between HRR and ED, accounting for 6.53% of the total association, with an indirect effect (IE) of −0.031 (95% CI = [−0.049, −0.020]).
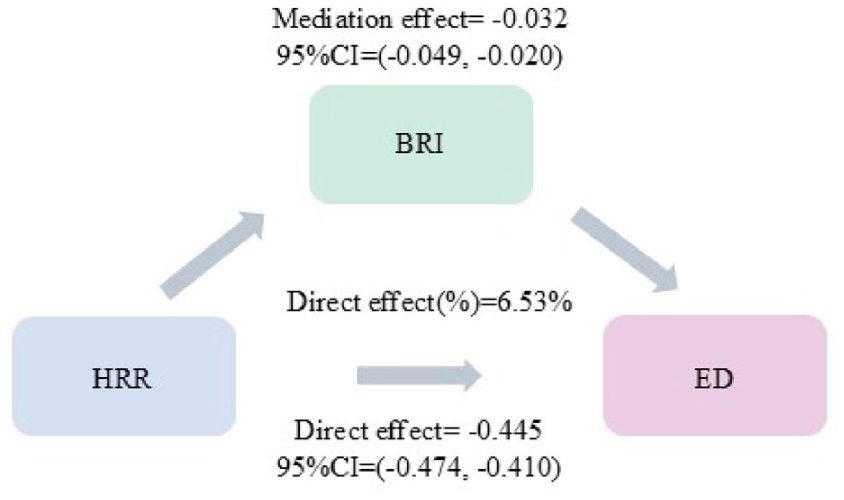
Path Diagram of the Mediation Analysis Models.
Sensitive Analysis
Severe ED was the outcome in the sensitivity study, and the earlier studies were conducted again. The regression findings are shown in Table 3, which demonstrates that in every model, there was a statistically significant correlation between HRR and severe ED. Participants in Q2 and Q3 showed considerably lower chances of severe ED when divided into terciles using Q1 as the reference, with
Multivariable Logistic Regression Analysis of the Association Between HRR and Severe ED, Weighted.

Values with
Discussion
In this extensive, nationally representative study of adult populations in the United States, we observed a statistically significant negative correlation between HRR and the incidence of ED. These results were further supported by sensitivity analyses, which suggested that HRR might be important biomarker for predicting ED risk and enabling prompt clinical interventions. Furthermore, our mediation analysis showed that BRI partially mediated this connection, offering profound insights into the potential underlying mechanisms linking inflammation with ED.
This study is the first analysis of the connection between HRR and ED that we are aware of. Red blood cells’ ability to carry oxygen is shown by their hemoglobin content, whereas the variability of the circulating erythrocyte volume is reflected by RDW (Ali et al., 2022; Salvagno et al., 2015). HRR may be a promising biomarker for a variety of diseases, according to accumulating data. Qu et al. demonstrated that a lower HRR constitutes an independent risk factor for frailty among elderly patients hospitalized with CHD. Furthermore, it emerged as a more potent prognostic indicator of frailty compared with Hb or RDW considered individually (Qu et al., 2021). In a meta-analysis, Chi et al. (2022) reported evidence of low HRR was associated with mortality and disease progression or relapse in patients with cancer. Furthermore, Yang and colleagues conducted a cross-sectional analysis encompassing 36,215 participants from the NHANES database, revealing a negative correlation HRR and the probability of stroke. Specifically, individuals with higher HRR levels exhibited a decreased risk of stroke (Xiong et al., 2024). The collective implications of these findings suggest a positive association between HRR and improved outcomes, aligning coherently with the results derived from our study.
Research within the field has increasingly acknowledged the significant role of inflammatory processes in the pathophysiology of ED (Das, 2007; Maiorino et al., 2018). Inflammation has emerged as a crucial factor that potentially increases an individual’s susceptibility to ED (D. Liu et al., 2024). Furthermore, we highlight HRR as an innovative inflammatory marker, underscoring its potential significance in monitoring inflammatory processes. The detection of these inflammatory markers not only facilitates early diagnosis of ED but also plays a pivotal role in preventing clinical deterioration and mitigating the risk of potential recurrences. Ongoing scholarly investigations have established that specific medications are efficacious in improving ED through their capacity to diminish inflammation, such as phosphodiesterase 5 inhibition (Paronetto & Crescioli, 2024). In addition to medications, pro-inflammatory diets have been implicated as a contributing factor to ED among male individuals in the United States (Ruan et al., 2022). Our findings indicate that HRR is a novel and readily accessible blood-based marker associated with ED. The rationale for selecting HRR over other inflammatory indicators lies in its unique composition. Erythropoietin (Epo) is widely used to treat anemia in patients with uremia. Multiple reports have shown that Epo therapy improves erectile function in dialysis patients, suggesting a link between anemia and/or Epo deficiency and ED (Suzuki et al., 2014). Conversely, RDW increases in the context of systemic inflammation, oxidative stress, and nutritional deficiencies—conditions that promote endothelial dysfunction and neuronal injury, which are key pathophysiological underpinnings of ED (Keenan, 2014). Therefore, a low HRR level concurrently signals diminished oxygen-carrying capacity and an elevated inflammatory burden, providing a composite surrogate marker for the multifactorial damage leading to ED. Visceral obesity, accompanied by an elevation in associated risk factors, is likewise linked to a pro-inflammatory state (Esposito & Giugliano, 2011). It is also a recognized source of pro-inflammatory cytokines and a contributing factor to endothelial dysfunction (Lyon et al., 2003; Trayhurn & Wood, 2004). BRI, serving as an index for the assessment of visceral obesity (Thomas et al., 2013), reveals a significant partial mediating role in the relationship between HHR and ED, as demonstrated by our mediation analysis. This finding aligns with previous research indicating a close link between abdominal obesity and ED (Lin & Lin, 2024). It suggests that one potential pathway linking low HRR to ED may involve inflammation related to visceral obesity. However, the proportion of the mediation effect was not substantial, highlighting that multiple pathways are likely at play, necessitating further investigation. In conclusion, HRR emerges as a novel inflammatory marker that exhibits a negative correlation with ED, thereby possessing substantial significance in evaluating the risk of ED occurrence.
Our study is not devoid of limitations. Primarily, our analysis is grounded in data sourced from the NHANES cycles spanning from 2001 to 2004. Given the substantial demographic shifts that have transpired thereafter, the applicability of our findings to the contemporary population is constrained. Future endeavors could involve examining the influence of HRR on ED within subsequent NHANES cycles. Furthermore, as a cross-sectional study, our research can merely illustrate the correlation between HRR and ED, falling short of establishing causality. In the coming years, we intend to pursue clinical trials or further follow-up studies and conduct larger-scale longitudinal research to delineate the causal link between HRR and ED and validate its predictive prowess across diverse populations. A major barrier to translating these results into practice is the current lack of a validated HRR threshold for ED risk stratification. Establishing this cut-off is a pivotal next step toward clinical application. If validated, HRR could be incorporated into existing ED risk assessment frameworks as an early-warning indicator of potential inflammation or vascular burden. This might prompt earlier clinical implementation of lifestyle interventions (e.g., weight loss, dietary improvement, exercise) to ameliorate inflammatory status, enhance hemoglobin levels, and potentially improve HRR itself. Whether such HRR-targeted interventions can translate into a reduced incidence of ED remains a key question to be addressed through randomized controlled trials. A further limitation is the lack of detailed data on psychological factors, medication use, and other relevant inflammatory markers in the NHANES database. The inclusion of such biomarkers would enable a more comprehensive understanding of the underlying mechanisms. Although subgroup analyses indicated a consistent association between HRR and ED across most subgroups, certain discrepancies were observed. Caution is warranted in interpreting these subgroup findings due to potential uncontrolled confounding within each subgroup and insufficient statistical power in smaller subgroups. Moreover, the generalizability of our results requires validation across populations of different ethnicities and geographical regions through multicenter studies. Conducting a systematic review and meta-analysis of existing studies examining the relationship between HRR and urological/sexual health outcomes would be valuable for synthesizing the evidence and quantifying the overall strength of association.
Despite these constraints, our study boasts several merits. Initially, we introduce a fresh perspective on a potential new marker that is cost-effective and readily accessible through blood indicators, offering avenues for ED prediction and facilitating early interventions. In addition, our data extraction from NHANES ensures rigorous adherence to standardized collection methods, minimizing bias and enhancing data authenticity.
Conclusion
In conclusion, our research shows a strong correlation, partially mediated by BRI, between HRR and ED risk in the adult U.S. population. A viable path for early ED diagnosis and risk assessment is indicated by the high association between HRR and ED. By integrating this marker into clinical practice, the illness burden may be decreased by enabling early therapies and prompt detection of ED risk. Large-scale cohort studies should be employed to further explore the underlying pathogenic mechanisms, and prospective studies should be the main focus of future research to validate these relationships.