
Abstract
Keywords
Introduction
Intravascular large B-cell lymphoma (IVLBCL) is a rare subtype of non-Hodgkin’s lymphoma, pathologically characterized by intravascular proliferation of malignant lymphocytes predominantly within the microvasculature of small-caliber vessels. 1 With potential to infiltrate several organs, including the skin, bone marrow, and central nervous system, 2 IVLBCL poses diagnostic challenges due to its overlapping radiological manifestations with interstitial lung disease (ILD) on high-resolution computed tomography (HRCT), particularly diffuse ground-glass opacities (GGOs) with or without interlobular septal thickening. 3 We report a critical case of a 51-year-old woman presenting with rapidly progressive respiratory failure secondary to delayed diagnosis of IVLBCL. Timely implementation of multidisciplinary therapeutic strategies resulted in favorable clinical outcomes, highlighting the importance of early histopathological confirmation in this diagnostic paradigm. The reporting of this study conforms to the CARE guidelines. 4 The CARE checklist is available in the Supplemental Material.
Case presentation
On December16, 2021, a 51-year-old female hairdresser with 20-year occupational exposure to hair dyes and no history of smoking came to our department for treatment. She presented with a 6-month history of non-productive cough, progressive exertional dyspnea, and a weight loss of 7 kg, which was classified as Modified Medical Research Council (mMRC) grade 2 (Figure 1). She has no symptoms of xerostomia or dry eyes, and physical examination revealed no Gottron’s sign, V-sign, arthralgia, or myasthenia. Previously, she had visited the community hospital multiple times due to persistent dry cough and was misdiagnosed with chronic bronchitis in May 2021. After taking the dextromethorphan tablets as prescribed by the doctor, her condition did not improve. On August 13, 2021, she began to experience shortness of breath after physical activity, which gradually worsened. Laboratory examination revealed a diffusion capacity of the lungs for carbon monoxide (DLCO) of 3.58 mL/min/mmHg (46.1% predicted). HRCT demonstrated diffuse bilateral involvement with GGOs (Figure 2(a)–(f)). Based on occupational organic compound exposure and imaging findings, she was misdiagnosed with non-fibrotic hypersensitivity pneumonitis (HP) and treated with prednisone (30 mg/day), showing partial improvement (mMRC grade 1) after 2 weeks. However, her dyspnea worsened to mMRC grade 3 with saturation of peripheral oxygen (SpO2) dropping to 85% as prednisone was tapered to 15 mg/day. Consequently, she was admitted to our hospital for further treatment this time.

Timeline showing the clinical course.
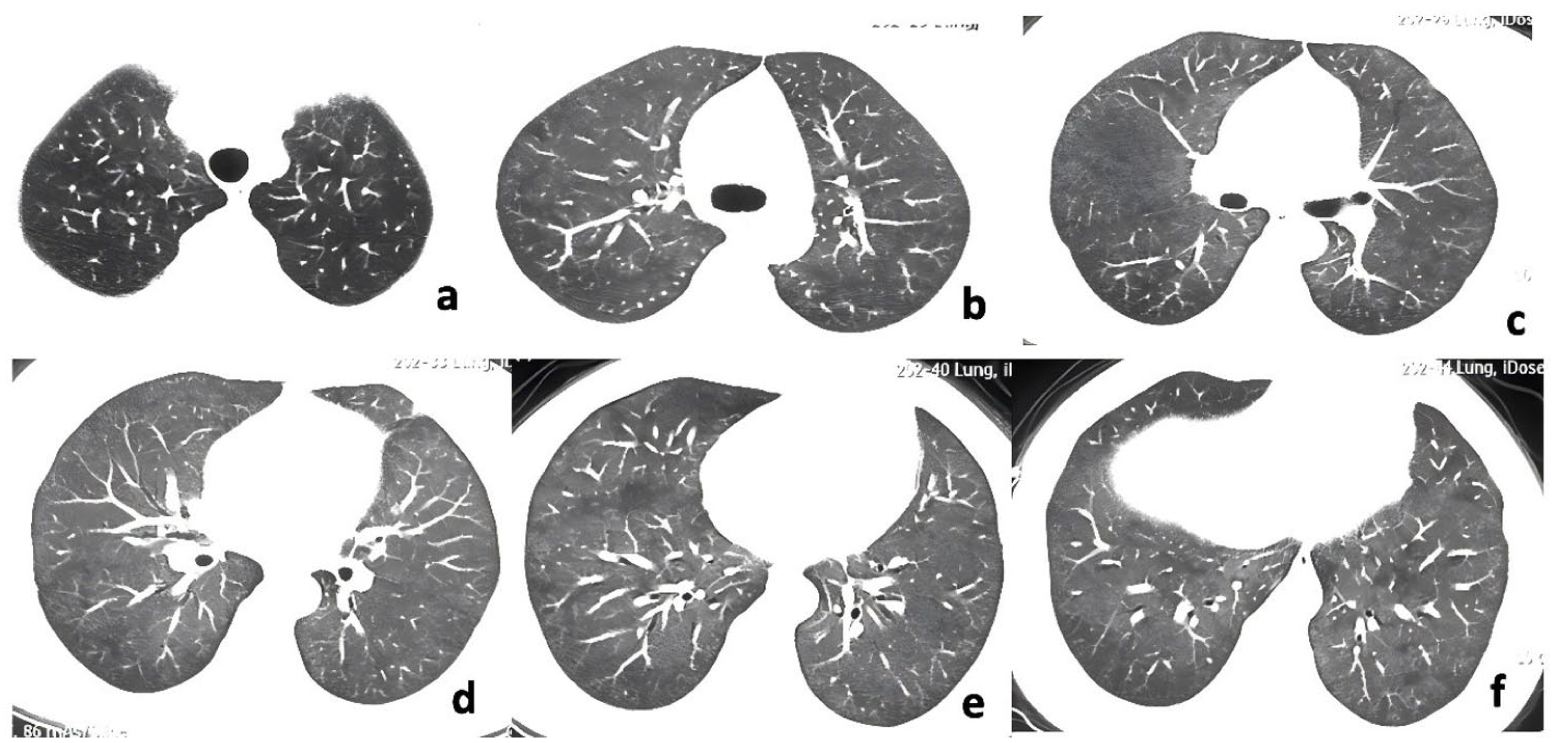
The HRCT of the chest of the patient on August 13, 2021.
The day after admission, laboratory investigations revealed pancytopenia with leukocyte count 1.92 × 109/L (neutrophils 1.13 × 109/L, lymphocytes 0.56 × 109/L), anemia (hemoglobin 102 g/L), and thrombocytopenia (84 × 109/L). Liver, cardiac, and renal function tests showed no abnormalities. Sputum bacterial and fungal smears showed no pathogenic microorganisms. Elevated inflammatory markers included D-dimer (596 ng/mL), lactate dehydrogenase (LDH, 1055.6 U/L), and ferritin (522.4 ng/mL). The level of serum interleukin-10 (IL-10) rose to 153.70 pg/mL. Autoimmune serology revealed positive antinuclear antibodies with a cytoplasmic granular pattern (titer 1:320) and elevated myositis-specific anti-SRP antibodies (+++). Serum krebs von den lungen-6 (KL-6) was elevated at 670 U/mL. Chest CT revealed diffuse GGOs with peribronchiolar distribution and adjacent consolidation in both lungs (Figure 3(a)–(f)). Pulmonary function testing demonstrated significantly impaired gas exchange capacity with DLCO at 39.4% predicted on December 17, 2021.

The HRCT of the chest of the patient on December 17, 2021.
The first round of multidisciplinary team (MDT) was promptly convened to address this complex ILD case. The radiologist’s assessment indicated that the patient exhibited imaging features consistent with nonspecific interstitial pneumonia (NSIP) or non-fibrotic HP. Hematology findings revealed bicytopenia, elevated LDH, prompting hematologic malignancy evaluation. Then, an 18 F-fluorodeoxyglucose positron emission tomography/computed tomography ( 18 F-FDG PET/CT) scan revealed diffuse GGOs in both lungs with a maximum standardized uptake value (SUVmax) of 2.8. The spleen was slightly enlarged with an SUVmax of 2.7, while bone marrow aspiration smear showed no abnormalities. Following the MDT discussion, we concluded that further pulmonary biopsy is warranted. However, severe respiratory failure precluded video-assisted thoracoscopic surgery lung biopsy (VATS-SLB), necessitating transbronchial cryobiopsy (TBCB) as an alternative minimally invasive approach. Histopathological examination of TBCB specimens showed dense lymphoid infiltration within vascular lumens and focal granulomatous lesions with atypical lymphocytes (Figure 4(a) and (b)). Immunoprofiling confirmed a B-cell lineage (CD20+/CD79a+/PAX5+) with germinal center markers (BCL-6+/CD10-) (Figure 4(c) and (d)), partial T-cell markers (CD5+/CD43+), and high proliferative index (Ki67 ≈ 80%).

Pathological and immunohistochemical staining results of TBCB.Histopathological analysis of Lung biopsy findings. (a-b) H&E staining showing intravascular lymphoid cells; (c-d) Immunohistochemistry demonstrating CD20 and BCL-6 positivity, confirming the diagnosis of intravascular large B-cell lymphoma.
The second MDT consultation ultimately verified that the tissue alterations were compatible with PIVLBCL. Following MDT consensus, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) chemotherapy was administered as follows: vincristine (4 mg, day 1), cyclophosphamide (1.2 g, day 1), doxorubicin liposome (40 mg, day 1), rituximab (600 mg, day 0), and dexamethasone (15 mg/day, days 1–15).
Following combined biologic and chemotherapy regimens, the patient demonstrated marked improvement in respiratory symptoms, with resolution of dyspnea and cough. Follow-up chest HRCT at 6-month post-treatment (April 12, 2022) revealed substantial resolution of GGOs with residual interstitial thickening (Figure 5(a)–(f)). Pulmonary function tests are close to normal, with forced vital capacity (FVC): 2.76 L (92.5% predicted) and DLCO: 5.28 mL/min/mmHg (68% predicted). During the latest follow-up in April 2025, she mentioned that she now walks without significant difficulty. After completing eight cycles of her original treatment regimen, she has discontinued medication and shows no signs of recurrence.

The HRCT of the chest of the patient on April 12, 2022.
Literature review
Search strategy
A systematic exploration was conducted on the PubMed online databases employing the search formula: (“intravascular large B-cell lymphoma” OR “IVLBCL” ) AND ( pulmonary OR lung OR “pulmonary involvement” OR “lung involvement”). The search period for the literature review is from 1 January 1998 to 22 April 2025.
Inclusion and exclusion criteria
Eligible studies or cases were included if they met the following inclusion criteria: (1) case reports, case series, and the case reports in literature review or comparative study, etc. on PIVLBCL published in English language during the above search period; (2) only cases of IVLBCL involving pulmonary vessels were included. Exclusion criteria included: (1) duplicated or inaccessible literature; (2) the articles whose case has been statistically processed, resulting in the loss of a large amount of patient information and the loss of statistical significance.
Data extraction and analysis
A meticulous review of all articles was undertaken to eliminate duplicate cases, ensuring comprehensive information for inclusion in the review. Data were meticulously extracted and presented as descriptive statistics in tables.
Results
Search results
A total of 118 articles were retrieved using the designated retrieval formula, yielding 108 case reports, 4 literature reviews, 3 reviews, 1 multicenter study, 1 comparative study and 1 book. Following a full-text review, 47 articles were excluded (not involved or was not exclusively involved in PIVLBCL, not published in English, loss of source, not in the required style of articles, and missing patient information in the case series), resulting in 64 studies meeting the inclusion criteria. A total of 75 patients were included, and the specific clinical characteristics of them are detailed in Table 1. Specific information on the sources of the included articles is given in Supplemental Table 1.
Baseline characteristics of 75 patients with PIVLBCL.

DLCO declining was described in 11 patients, and the values were available in 7 patients.
sIL2R rising was described in 27 patients, and the values were available in 26 patients.
CRP rising was described in 30 patients, and the values were available in 29 patients.
LDH rising was described in 54 patients, and the values were available in 52 patients.
The results of the histopathological examination were described in 64 patients.
18F-FDG PET/CT, 18F-fluorodeoxyglucose positron emission tomography/computed tomography; ANED, alive with no evidence of disease; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisolone; CRP, C-reactive protein; CT, computed tomography; DLCO, diffusion lung capacity for carbon monoxide; DOD, dead of disease; GGN, ground-glass nodule; GGO, ground-glass opacity; ILVBCL, intravascular large B-cell lymphoma; LDH, lactatedehydrogenase; NA, not available; PFS, progression-free survival; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone; sIL2R, soluble interleukin-2 receptor; SLB, surgical lung biopsy; TBCB, transbronchial cryobiopsy; TBLB, transbronchial lung biopsy.
Symptoms
Prominent complaints included fever (
Laboratory examination
As a common marker of lymphocyte activation, soluble interleukin-2 receptor (sIL2R) was found to be elevated in 27 patients (36.0%) with a median value of 3065.5 U/mL (range 1041 to 20300 U/mL); LDH was found to be elevated in as many as 54 patients (72.0%) with a median value of 1363 IU/L (range 280–4989 IU/L); in addition to that C-reactive protein (CRP) was found to be abnormally elevated in 30 patients (40.0%) with a median value of 4.30 mg/dL (range 0.6 to 36.28 mg/dL).
Chest CT and 18F-FDG PET/CT
GGOs were most common in chest CT images of patients with PIVLBCL, with 41 patients (54.7%) reported with this condition. In addition, pleural effusion (
Diagnostic methods
Of all confirmed methods, 23 patients underwent conventional surgical lung biopsy. As for thoracoscopic surgery, transbronchial lung biopsy (TBLB was performed in 23 cases (33.3%). However, TBCB was only performed in 1 case (1.3%). In addition, 6 cases (8.0%) were diagnosed as PIVLBCL at postmortem examination.
Histopathology
Among the common markers of B cells, CD20 was found to be expressed in almost all biopsy samples (
Statistics of misdiagnosis
PIVLBCL is often misdiagnosed as other diseases as well. We have summarized 22 cases that were misdiagnosed during the treatment process, which are presented in Table 2. Among these cases, interstitial lung disease (
The statistics of misdiagnosis of large B-cell lymphoma in pulmonary vessels and the basic conditions of patients.

ADM, adriamycin; ANED, alive with no evidence of disease; APTT, activated partial thromboplast; AST, aspartate transaminase; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisolone; COP, cryptogenic organizing pneumonia; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; CT, computed tomography; CTX, cyclophosphamide; DIC, disseminated intravascular coagulation; DLCO, diffusion lung capacity for carbon monoxide; DOD, dead of disease; ESR, erythrocyte sedimentation rate; F, female; FDG, flurodeoxyglucose; GGN, ground-glass nodule; GGO, ground-glass opacity; HP, hypersensitivity pneumonitis; HRCT, high resolution computed tomography; IIP, idiopathic interstitial pneumonia; ILD, interstitial lung disease; ILVBCL, intravascular large B-cell lymphoma; IP, interstitial pneumonia; LDH, lactatedehydrogenase; M, male; MAHA, microangiopathic hemolytic anemia; NA, not available; OLB, open lung biopsy; PET, positron emission computed tomography; PFS, progression-free survival; PT, prothrombin time; PTE, pulmonary thromboembolism; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone; SCLC, small cell lung cancer; SHP, summer-type hypersensitivity pneumonitis; sIL-2R, soluble IL-2 receptor; SSc, systemic sclerosis; TBCB, transbronchial cryobiopsy; TBLB, transbronchial lung biopsy; VATS, video-assisted thoracoscopic surgery; VCR, vincristine.
Treatments after a clear diagnosis
R-CHOP and CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) are both commonly used treatments for PIVLBCL. Among them, 39 patients (52.0%) received R-CHOP therapy, and 15 patients (20.0%) received CHOP therapy. Besides, CHASER (cyclophosphamide, high dose of cytarabine, dexamethasone, etoposide, and rituximab), R-ICE (rituximab, ifosphamide, carboplatin, and etoposide), MCEC (ranimustine, carboplatin, etoposide, and cyclophosphamide), IT-MTX (intrathecal methotrexate), MR-CHOP (methotrexate, rituximab, cyclophosphamide, adriamycin, vincristine, and prednisolone), DeVIC (dexamethasone, etoposide, ifosfamide, and carboplatin), MACOP-B (methotrexate, leucovorin, doxorubicin, cyclophosphamide, vincristine, and bleomycin) and other therapies were also used in individual cases for the treatment of PIVLBCL.
Outcome
Most patients received good treatment, including 19 cases (25.3%) who were alive with no evidence of disease (ANED) and 21 cases (28.0%) who achieved progression-free survival (PFS). Unfortunately, at the same time, 24 patients (32.0%) died of PIVLBCL and other concurrent diseases. In addition, there were 11 cases (14.7%) where no follow-up survival results were reported, or the patients gave up treatment.
Discussion
IVLBCL is an extremely rare malignant extranodal DLBCL with an annual incidence of less than one in a million, 5 which can be categorized into classical, cutaneous, and phagocytosis-associated subtypes. 2 Microscopically, tumor lymphocytes are present in large numbers in the lumen of small and medium-sized blood vessels, especially capillaries, and often have a single prominent nucleolus and frequent mitotic figures. 6 The median age of IVLBCL patients is about 70 years, and the incidence is similar in males and females. 2 IVLBCL is characterized by vascular invasion, which can involve various organs of the body, including bone marrow, central nervous system, skin, adrenal gland, lung, liver, kidney, spleen, thyroid gland, pituitary gland, and gastrointestinal tract, 7 and can present with dyspnea, epilepsy, bone marrow suppression, and other manifestations. In the 75 patients counted in this paper, fever, and exertional dyspnea were the two most common manifestations, and other symptoms such as fatigue, night sweats, and cough are also part of the manifestations of PIVLBCL, but it is relatively rare for patients to present with chest pain.
Unfortunately, according to current research data, the median survival time of IVLBCL patients is only about 1 year. The atypical symptoms of IVLBCL make early diagnosis and treatment crucial, which can be confirmed by biopsies, such as skin biopsies and biopsies of the corresponding organs. In particular, the diagnosis of IVLBCL patients with lungs as the first symptom is extremely difficult and requires adequate histopathologic biopsy of the lungs. In most cases, tumor lymphocytes in PIVLBCL do not appear in routine peripheral blood smears, and limited findings such as anemia, elevated LDH, CRP, and sIL2R do not give a definitive diagnosis of PIVLBCL. 8 In addition, radiologic images of PIVLBCL also usually show only nonspecific ground-glass shadows and nodules, 3 and in a few cases, pleural effusion is present, which makes it very challenging to separate it from other lung diseases. In the absence of a diagnostic basis and pathologic findings, PIVLBCL is often misdiagnosed in its early stages as pneumonia, interstitial lung disease, and pulmonary thromboembolism.9,10 18 F-FDG PET/CT demonstrates significant diagnostic value in PIVLBCL in this situation, particularly the characteristic diffuse bilateral pulmonary FDG uptake pattern, known as the “hot lung sign.” 11 Notably, some patients may present with significant FDG uptake even when conventional CT imaging appears normal, highlighting the superior sensitivity of 18 F-FDG PET/CT in detecting early vascular lymphomatous infiltration. This suggests that 18 F-FDG PET/CT should be considered as an important diagnostic tool when PIVLBCL is suspected, especially in cases where structural imaging findings are minimal or nonspecific.
Recent studies have also highlighted the potential diagnostic significance of serum IL-10 in IVLBCL. IL-10, an immunosuppressive cytokine, could facilitate tumor growth and immune evasion by mediating an immunosuppressive tumor microenvironment. Zhang et al. reported that all 17 IVLBCL patients tested for IL-10 were positive. When the serum IL-10 cutoff was defined as 95.65 pg/mL, the diagnostic sensitivity and specificity for IVLBCL were 80% and 100%, respectively. IL-10 levels decreased in all patients following treatment, but only those achieving complete remission (CR) had IL-10 levels falling below 30 pg/mL. 12 Li et al. also reported that elevated IL-10 levels were observed in 5 of 6 patients (83.3%) with IVLBCL. 13 In this case, the patient’s IL-10 level reached as high as 153.70 pg/mL prior to R-CHOP therapy, although it is regrettable that this patient did not undergo another IL-10 level test subsequently. A case report in the literature review also reported a patient with extremely high IL-10 level (>1000.0 pg/mL) on the day of hospitalization and subsequently decreasing to 5.8 pg/mL after R-CHOP treatment. 14 All the above reports have consistently indicated that IL-10 is a valuable biomarker for the early diagnosis and treatment monitoring of IVLBCL. It will be of great significance to combine it with commonly used indicators such as LDH and sIL2R for the combined diagnosis of IVLBCL.
In this case, the misdiagnosis occurred due to the patient’s 20-year history of hair dye exposure and imaging similar to non-fibrosing HP, which makes confirmation of the diagnosis by lung biopsy particularly important. The main modalities for lung biopsy include traditional surgical open lung biopsy, TBLB and TBCB. 15 Although surgical lung biopsies are able to obtain larger volumes of tissue samples and provide more comprehensive lung tissue information contributing to diagnostic accuracy, there is an increased risk of bleeding, pneumothorax, and infection. 16 Therefore, TBLB and TBCB have become safer and more reliable options. TBLB offers the advantages of simplicity, speed, and lower risk of moderate-to-severe bleeding. However, it yields a limited sample volume and tissue susceptible to mechanical compression, resulting in lower detection rates and unnecessary repeat procedures for patients. In contrast, TBCB obtains larger tissue blocks covering broader areas, providing higher diagnostic value. Yet, it requires longer procedure times than TBLB and carries higher rates of bleeding and pneumothorax. 17 A multicenter study involving 124 patients with interstitial lung disease reported a diagnostic yield of 47.6% for TBCB versus 19.4% for TBLB, with TBCB requiring fewer average biopsies (3.5 vs 4.1). However, 6.5% of patients experienced Grade 3 (moderate) bleeding after TBCB, compared to 0.8% with TBLB. 18 Another study involving 359 IPD patients similarly reported fewer average biopsies per patient with TBCB (3.2 vs 3.6), but TBCB was associated with increased bleeding risk. 19 Overall, TBCB enhances diagnostic yield for histologically complex entities in multidisciplinary settings, approaching the diagnostic efficacy of surgical biopsy while preserving the minimally invasive nature of TBLB. Future efforts to standardize TBCB techniques, including probe size selection and hemostasis protocols, could help reduce complication rates and optimize its application in diagnosing rare pulmonary vascular lymphomas. In contrast, TBCB is able to obtain tissue samples over a larger area, avoiding the tissue extrusion commonly seen in traditional bronchoscopic forceps biopsies, resulting in a more accurate pathologic diagnosis. 17 In pathological tissue staining, high expression of CD20 and CD79a often suggests the development of B-cell-associated malignancies, while the expression of paired box protein 5 (PAX-5) and Ki-67 correlates with tumor aggressiveness, growth rate, and poor prognosis. In our count of 64 patients who underwent tissue biopsy, as many as 61 patients showed high expression of CD20. This process of pathologic diagnosis requires a high degree of clinical experience and skill on the part of the pathologist, underscoring the importance of accurate diagnosis in the disease identification and management of interstitial lung disease.
In addition, the value of this case is reflected in its two noteworthy features; first, the patient presented with isolated diffusion loss, which, in combination with the patient’s diffuse ground-glass shadow lung CT presentation, is usually suggestive of interstitial lung disease. The most common cause of reduced diffusion function is reduced alveolar membrane permeability due to pulmonary fibrosis. 20 However, the patient did not show signs of restrictive ventilatory dysfunction. For this reason, another factor that may affect diffusion function needs to be considered: extensive pulmonary capillary disease, including pulmonary capillary hemangiomatosis, pulmonary veno-occlusive disease, and PIVLBCL, which leads to thickening of the pulmonary capillary membranes and a decrease in permeability, which in turn causes reduced diffusion function. Among the 75 patients with PIVLBCL that we counted, a total of 11 patients showed decreased pulmonary diffusion function,10,21–28 but invariably reported no pulmonary ventilatory dysfunction, among which even six patients were misdiagnosed during the diagnostic process and achieved continued survival in only five of the reported cases. This suggests that we need to be alert to the possibility of PIVLBCL in patients found to have diffuse ground-glass shadows in both lungs accompanied by purely diffusion hypoplasia and that an early definitive diagnosis can help prolong the patient’s survival.
In terms of treatment, following chemotherapy, the management of IVLBCL has entered a new era of immunotherapy and targeted therapy. R-CHOP and CHOP remain the most commonly used regimens for treating IVLBCL at present, with rituximab offering substantial survival benefits for patients. Bruton’s tyrosine kinase (BTK) inhibitors directly suppress tumor growth by blocking B-cell receptor signaling, bringing new hope to targeted therapies for IVLBCL and demonstrating favorable synergistic effects when combined with R-CHOP. 29 Two recent studies demonstrated favorable outcomes with zanubrutinib combined with R-CHOP in patients with IVLBCL, with or without central nervous system (CNS) involvement.30,31 This literature review also reports one patient achieving CR using the same regimen. 14 Although studies on BTK inhibitors for IVLBCL remain limited, their therapeutic outcomes suggest potential as a key component of standard IVLBCL treatment regimens. Furthermore, patients with CNS involvement in IVLBCL have a poor prognosis, as most drugs cannot cross the blood-brain barrier (BBB). BTK inhibitors, leveraging their small-molecule advantage, exhibit strong BBB penetration, making them a preferred adjunctive therapy for such patients. 13
The diagnostic and therapeutic course of this case emphasizes the critical role of accurate pathological diagnosis in the management of difficult interstitial lung diseases, and the successful application of TBCB provides key evidence for the definitive diagnosis of PIVLBCL. Patients presenting with diffuse ground glass shadows in both lungs accompanied by pure diffusion hypoplasia should be alerted to the possibility of PIVLBCL development. In addition, this case highlights the importance of a broad differential diagnosis in patients with atypical presentations of interstitial lung disease and the need for multidisciplinary collaboration in the face of difficult cases.
Conclusion
The diagnosis and treatment of this case highlighted the key role of accurate pathological diagnosis in the management of difficult interstitial lung diseases, and the successful application of TBCB provided key evidence for the diagnosis of PIVLBCL. In addition, this case highlights the importance of a broad differential diagnosis in patients with interstitial lung disease with atypical presentation and the need for multidisciplinary collaboration in challenging cases.
Supplemental Material
sj-docx-1-tar-10.1177_17534666261424374 – Supplemental material for Pulmonary intravascular large B-cell lymphoma misdiagnosed as allergic pneumonia: a case report and literature review
Supplemental material, sj-docx-1-tar-10.1177_17534666261424374 for Pulmonary intravascular large B-cell lymphoma misdiagnosed as allergic pneumonia: a case report and literature review by Hao Deng, Bingpeng Guo, Gengjia Chen, Qiexinhao Li, Du Feng, Chuoqi Yang, Xiaolu Zhong, Qun Luo, Shiyue Li and Qian Han in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_17534666261424374 – Supplemental material for Pulmonary intravascular large B-cell lymphoma misdiagnosed as allergic pneumonia: a case report and literature review
Supplemental material, sj-pdf-2-tar-10.1177_17534666261424374 for Pulmonary intravascular large B-cell lymphoma misdiagnosed as allergic pneumonia: a case report and literature review by Hao Deng, Bingpeng Guo, Gengjia Chen, Qiexinhao Li, Du Feng, Chuoqi Yang, Xiaolu Zhong, Qun Luo, Shiyue Li and Qian Han in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We sincerely thank the patient and her family for their acceptance and cooperation to participate in our case report. We thank all the staff in our department who have been involved in the treatment of this patient. We also extend our heartfelt appreciation to the anonymous reviewers, whose diligent efforts significantly enhanced the quality of this paper.
Declarations

Supplemental material
Supplemental material for this article is available online.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Artificial intelligence policy
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.