
Abstract
Introduction
The first reported case of ureteroscopic treatment for stone disease in a paediatric case was in the year 1988 by Ritchey
In their study regarding neurological development, Le
Paediatric ureteroscopy is specialised due to the minimisation of equipment, anaesthetic challenges, and developmental and anatomic abnormalities which are common in children with kidney stones.5–11 The outcome of intervention is variable between centres based on their experience, expertise and choice of chosen intervention. In a study of 54 patients, Gedik
In this two-centre study, we compared the outcomes of ureteroscopy for stone disease management in early and late childhood to contribute to progression of surgical management and provide data for safety and efficacy for the same. We hypothesise that the role of ureteroscopy and laser stone fragmentation (URSL) is safe and effective across all age groups of paediatric patients.
Materials and methods
Data was collected on consecutive patients from two tertiary paediatric endo-urology European centres [University Hospital Southampton (UHS), United Kingdom, and Fundació Puigvert (FP), Barcelona, Spain] operating independently of each other. The study was registered as an audit with UHS audit committee (audit number 6901) and was approved by the FP Hospital Ethics Committee, and retrospective data was collected from both centres. A valid written informed consent was obtained from all the patients/parents/legal guardians for their data to be utilised in this study. This was further analysed using electronic health records and cross-checked with patient correspondence and discharge summary. The operating teams were trained in paediatric ureteroscopy, with medical and surgical expertise in order to provide best possible patient care.
Collection of data was spread over a period of 15 years from June 2006 to January 2021, and a total of 184 ureteroscopies were performed in 148 patients. Patients were divided into two groups, namely, early childhood (age ⩽ 9 years) and late childhood (age 9 to ⩽16 years).2,3 Data regarding patient age, sex, initial presentation, mode of initial investigation, co-existing anatomical and metabolic anomalies, date of surgery, pre- and post-operative stenting, operative duration, access sheath use, intra-operative complications, post-operative complications (within 30 days), SFR, re-intervention and follow-up imaging were recorded.
Procedural details have previously been extensively detailed and discussed.7–9 Stone diagnosis was established by ultrasound scan or plain KUB XR and during follow-up, a renal USS (Ultrasound Scan) was done to confirm the stone-free status. A multidisciplinary team (MDT) discussed all cases. SFR was defined as endoscopically stone free and radiologically stone free (defined as fragments < 2 mm) at follow-up, 2 to 4 months post-procedure. During the procedure, a 4.5 F (Richard Wolf, USA) semirigid and 7.5 F Flex X2 fURS (Karl Storz Endoscopy Ltd., UK) was used, with a Holmium: YAG laser (100, 60 or 20 W Lumenis, USA) for fragmentation using a 272-lm laser fibre (Lumenis, Inc.). The use of intra-operative access sheath and post-procedural stent was surgeon-dependent, and a stone fragment was extracted and sent for crystallographic analyses.
The data was anonymised and analysed using excel (Microsoft, USA) and SPSS (IBM® SPSS® version 27). Chi-square test was used in SPSS to obtain the statistical significance in the form of
Results
A total of 148 patients underwent 184 procedures (1.2 procedure/patient) during the study period (Table 1), with 66 patients in early childhood group and 82 patients in late childhood group. The mean age in early and late childhood groups were 5.6 and 13.3 years, and a male: female ratio of 1.6:1 and 1.1:1, respectively. The median stone size in both groups was 9.0 mm. The clinical presentations in early and late childhood groups were with pain (40.9%
Pre-operative demographics of patients undergoing URSL procedure for both groups.
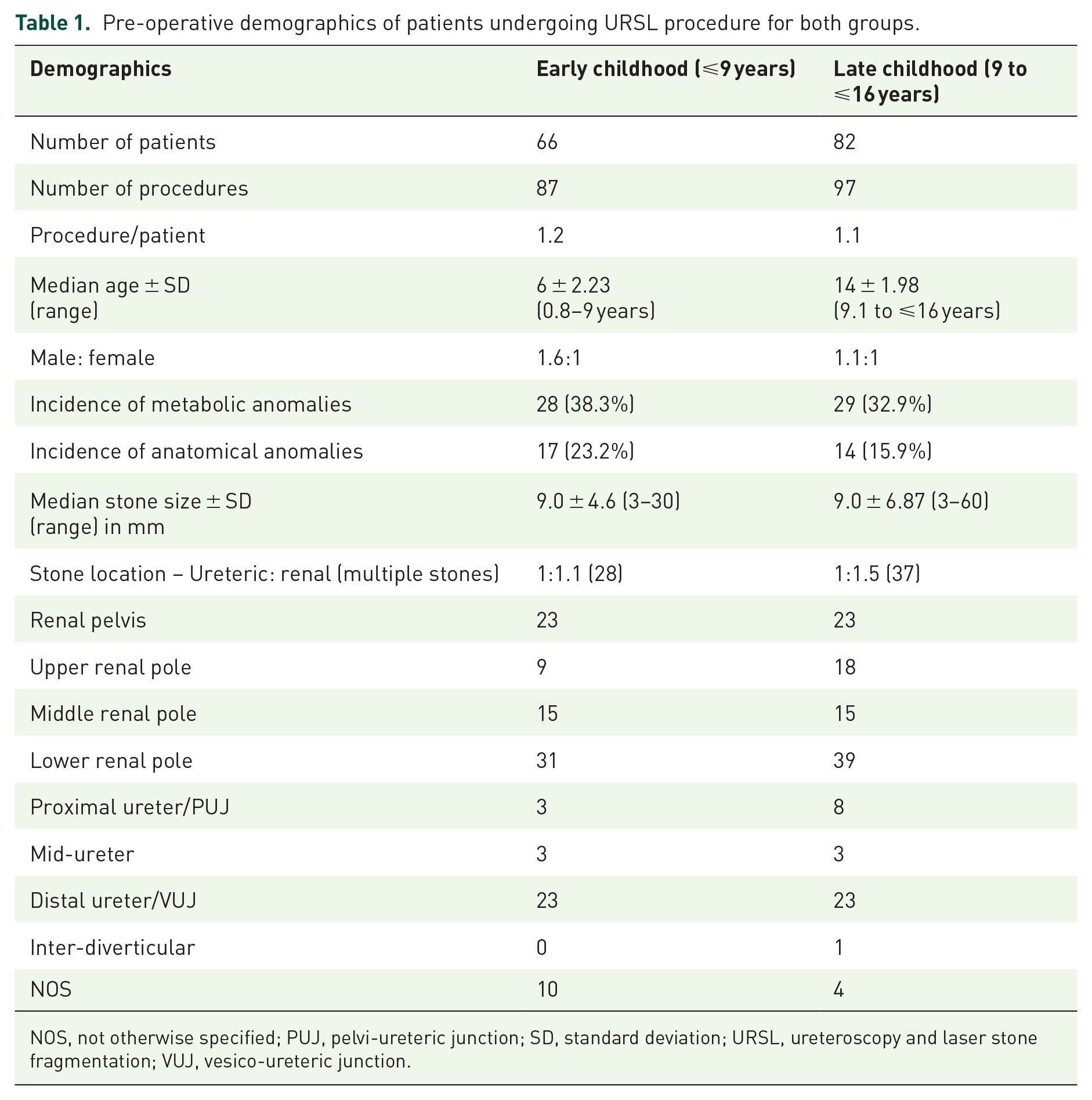
NOS, not otherwise specified; PUJ, pelvi-ureteric junction; SD, standard deviation; URSL, ureteroscopy and laser stone fragmentation; VUJ, vesico-ureteric junction.
The mean operative duration for early and late childhood was 86.2 and 82.4 min, respectively. There was no significant difference in pre- or post-operative stent rates in early and late childhood groups (42% and 51.5%,
Post-operative outcomes of patients of both age groups undergoing URSL.

UAS, ureteric access sheath; URSL, ureteroscopy and laser stone fragmentation.
Discussion
This study demonstrates the safety of performing URS for renal stone disease across all paediatric age groups with our SFR comparable with previously published data5–13 and an overall post-operative complication rate of 7% across all age groups. All the ureteric injuries (1.6%) were of grade 1 classification and were managed conservatively with stent insertion.
Ureteroscopy seems to have evolved itself as the most favoured treatment strategy balancing the clinical efficacy with safety perhaps in contrast to shock wave lithotripsy (SWL) and percutaneous nephrolithotomy (PCNL), respectively.7–14 With the advancement in technology providing smaller size equipment for URS and more surgeons trained in paediatric endo-urology operating in high-volume centres, it is emerging as a frontline alternative. Our study used fragmentation and stone dusting for treatment and reflects a SFR of 87.8% in early childhood and 90.2% in late childhood with minimal associated morbidity. Rob
The European Association of Urology (EAU) urolithiasis guidelines
18
includes all the three modalities (SWL, URS and PCNL) for active intervention of renal stone disease, with SWL and fURS offering a SFR of 70–90% and 76–100%, respectively. SWL is the first choice of treatment for paediatric stone disease though it often requires sedation or general anaesthetic in this population for patient positioning and tolerability of the procedure. It is often associated with renal colic, steinstrasse, sepsis and transient hydronephrosis, and may not always be successful. In their follow-up post SWL
In their paediatric patient cohort of 11 patients, Utang˘aç
A systematic review by Pietropaolo
With easy access to miniaturised instrument, courses for training and newer lasertripsy methods like ‘pop-dusting’,
28
URS can be safely used in paediatric cases in appropriately equipped centres where staff are well trained to aide early recognition of intra- and post-operative complications. With advent in technology, cost-effectiveness and more research available on URS, improved outcomes can be expected and perhaps equivocal findings when compared with adult population.
29
In the management of upper urinary tract stones in children, Freton
Our article is based on retrospective data, and due to small number of patients, it was not possible to perform a multivariate analysis, but this has been a consecutive series of patients with data collected and analysed by neutral third party not involved in the original study. However, failure to access during the primary URS procedure was not uniformly captured, which has been shown to be higher for the early age group patients. 31 It is the largest observational study comparing outcomes of URSL in early and late childhood. This will set an important benchmark in counselling patients although studies should also look at standardising outcome measures such as SFR and looking at cost and quality of life of patients. The future paediatric urolithiasis guidelines should factor in patient age for recommendations of any surgical treatment, as the choice of treatment and outcomes could be influenced by the age. Based on our results, perhaps ureteroscopy could become a first-line treatment for paediatric urolithiasis in the late childhood.
Conclusion
Paediatric URSL achieves good results in both early and late childhood with comparable SFRs, although the complications and need for second procedure were marginally higher in the early childhood group. Our study would set up new benchmark for patient counselling in future, and perhaps this needs to be reflected in the paediatric urolithiasis guidelines. Future prospective randomised studies are needed to corroborate our results.