
Abstract
Introduction
In recent years, there has been a notable rise in youth sports participation in Europe, concomitant with an increased incidence of related injuries. 1 It has been demonstrated that the participation in high-risk traumatic activities and increased specialization of young athletes in a single sport is associated with a rise in injuries. 2 Specifically, there has been a notable increase in conditions such as anterior cruciate ligament (ACL) 3 and meniscal 4 tears necessitating surgical intervention.
The increase in sports injuries can be attributed, at least in part, to improved identification of injuries, while advancements in surgical techniques and increased confidence among surgeons in managing paediatric sports injuries have resulted in a higher incidence of surgical interventions.
This trend has generated a growing interest in the application of arthroscopy as an effective intervention for sports-related injuries: using arthroscopy, surgeons can perform diagnosis and treatment of the involved joint. Thanks to its minimally invasive nature, it has proven to be a versatile and efficient treatment modality for various pathologies.5,6 This approach offers significant benefits, such as facilitating quicker recovery, better aesthetic results and minimizing disruption to the daily activities of young patients. Different from adults, children’s joints are smaller and closer to the growth plates: however, due to advancements in technique, increasingly miniature instrumentation and improved knowledge of pathologies, the use of arthroscopy has also become widespread among paediatric orthopaedics. 6
Studies from North America suggest an increase in arthroscopic knee cases, especially for ACL reconstruction under 15 years of age, 7 and hip surgeries in skeletally immature patients. Moreover, paediatric sports medicine is becoming a new subspecialty. 8
In Europe, there has been an increase in research, study groups, medical education and attention to arthroscopy and paediatric sports medicine but the real impact of this type of surgery in our hospitals was not yet defined.9,10 An analysis of the trend of paediatric arthroscopies in Europe is therefore essential due to its growing role in the management of sports-related injuries.
The purpose of this study is to describe and identify trends over a 20-year period, from 2000 to 2019 in the number of arthroscopic surgeries performed throughout European hospitals involved in paediatric sports. The primary objective was to identify a trend in the number of arthroscopic surgeries performed throughout European hospitals. The secondary objective was to assess potential variations or new entries in the anatomical regions undergoing arthroscopy. Additionally, we aimed to investigate changes over the years in the targeted age group as well as the gender distribution of patients.
Methods
Our retrospective study was conducted within the European Paediatric Orthopaedic Society (EPOS) Sport Study Group, a recent division specializing in paediatric orthopaedics sports medicine in Europe.
Participants were recruited at the 2022 EPOS Sport Study Group Annual Meeting. Additionally, to expand the participant pool, a cohort of experts, including both adult and paediatric orthopaedic surgeons, was recruited through the EPOS mailing list in September 2022. Only orthopaedic surgeons specializing in paediatric sports medicine surgery and research were included. This specialized focus ensures that the collected data are highly relevant and of exceptional quality, reflecting the expertise and targeted experience of the contributors. No monetary incentives were given to participants. Figure 1 illustrates the flowchart for excluding centres and data.

Centres’ recruitment process.
If a centre did not send the response within 3 months, a second e-mail was sent. E-mails included the link to an electronic Google Forms survey, an explanatory letter with the purpose of the study and a list of all the questions. Participants were independently tasked with completing the online questionnaire, after confirming their consent to participate in the survey. Clarifications from the Principal Investigator (P.I.) were available if needed.
The questionnaire was developed by an orthopaedic surgeon highly specialized in paediatric surgery with international experience and was reviewed by two other surgeons with similar expertise, based on the Checklist for Reporting Results of Internet E-Surveys. 11 The original development team conducted an internal review of the survey, assessing its format and clarity: following necessary revisions, subsequent modifications were made through collaborative discussion among all authors. The final questionnaire comprised 21 questions divided into four parts. The first part involved the country and hospital’s surgical intervention profile, distinguishing between paediatric, adult or mixed caseload. The remaining three parts, consistent across the three selected years, gathered data on the total number of paediatric orthopaedic surgery and paediatric arthroscopy cases (categorized by elective and emergency procedures): our survey did not inquire about the specific number of diagnostic and interventional procedures performed. Subsequently, participants were prompted to delineate arthroscopy cases based on anatomical region and specify patient age (divided into three different groups: under 11, 11–14 years and 15–18 years) and gender. The survey took approximately 10 min to complete, and respondents were given the opportunity to review and modify their answers, ensuring data accuracy and quality. The survey was only submitted to the server if all required fields were completed.
To assess the trends in arthroscopy over the past 20 years, we collected data from surgical hospital records, focusing on three exemplary years: 2000, 2009 and 2019. A one-year margin was allowed for analytical purposes.
Each hospital conducted the investigations independently using its Operating Room Management System. Only units with confirmed data accuracy were invited to participate. Data collection was limited to digital records. Any data with insufficient accuracy were excluded: incomplete data provided by the centres in the various survey categories were excluded from the analyses (e.g. the anatomical site not specified in the type of procedure). To comply with regional Internal Review Board (IRB) regulations, certain patient data, such as age and gender, were not collected. To ensure data integrity, these variables were excluded from the analyses and visualizations.
In cases where a centre was not yet operational or unable to retrieve the data due to organizational issues (i.e., no digital archive in the early 2000s), data were excluded, so two separate analyses were conducted: one including centres with data available from 2000 to 2019 and another including those with data available only in the most recent 10 years (i.e. 2009 and 2019).
The collected cases included all orthopaedic surgeries performed on paediatrics (patients aged below 18 years), both elective and emergency, and all arthroscopic procedures, regardless of type and anatomical region.
Statistical analysis
Descriptive analysis was used to characterize the observed trends in the number of performed paediatric arthroscopies in the involved European centres over the study period. Data were described as absolute frequencies and percentages and displayed through spaghetti plots or bar plots. The Cochran-Armitage test was performed to highlight trends in time.
Statistical analyses were performed with R 4.3.1 (http://www.R-project.org). All
Results
A total of eight different centres were recruited from seven different countries (Finland, France, Italy, Portugal, Spain, Switzerland, UK), with a participation rate of 50.0% (8 out of 16 invited centres).
As three out of the eight centres were not operational in the year 2000 or unable to retrieve the data, the centres were divided into two groups, and the analyses were conducted independently: Group 1 (G1,
In four centres, the predominant activity was paediatric, while the others were considered mixed centres. This approach allowed for an independent analysis of the data, considering that the increase in the number of centres could introduce bias in the rise of case numbers.
Overall number of cases
In G1 (2000–2019), excluding Finland from the analysis (see Discussion for comprehensive explanation), the total number of paediatric arthroscopic surgeries performed in Europe significantly increased (Figure 2(b),

Total paediatric surgeries performed between 2000 and 2019 in G1: orthopaedic surgeries (a), arthroscopic surgeries (b) and the ratio between arthroscopic and orthopaedic surgeries (c). The red line represents the overall number, and the black line represents the overall number calculated excluding Finland.
Examining trends in the different centres, cases of arthroscopies increased both in terms of total number and percentage in all states except for Finland, where the number of arthroscopies decreased from 12% to almost 4%. In some countries (e.g. Italy), there was a peak of 18.5% in the percentage of arthroscopies in 2019.
Considering all centres in the period 2009–2019 (G2), the upward trend is confirmed both in the total number of cases (from 393 to 615 cases, Figure 3(b)) and in the percentage of arthroscopies (from 5.1% to 6. 8%) (Figure 3(c)). The increase is observed in all centres, with the sole decrease noted in Finland. The overall trend, both accounting for or excluding Finland, was statistically significant (

Total paediatric surgeries performed between 2009 and 2019 in G2: orthopaedic surgeries (a), arthroscopic surgeries (b) and the ratio between arthroscopic and orthopaedic surgeries (c). The red line represents the overall number, and the black line represents the overall number calculated excluding Finland.
Anatomical region
The study investigated the seven main anatomical districts where arthroscopies are performed.
In G1, the knee was consistently the most frequently treated area, with an absolute number between 150 and 210, that is, around 80% of the total number of arthroscopies over the 20-year period (Figure 4(a)). The total number of arthroscopies for each anatomical region increased in time, except for the shoulder which showed a significant decrease (

G1 paediatric arthroscopic surgeries are divided into seven anatomical regions (a). In panel (b), the knee was excluded to highlight the number of cases in the other regions.
Elbow interventions showed a significant increase in the number of cases performed (
Considering G2, the findings corroborate the aforementioned observations. The knee remained the most common site between 2009 and 2019, with a significant increase in the total number of cases from 310 in 2009 (83% of the total arthroscopies) to 519 in 2019 (88%) (

G2 paediatric arthroscopic surgeries are divided into seven anatomical regions (a). In panel (b), the knee was excluded to highlight the number of cases in the other regions.
Age
We described the number of arthroscopies in age classes (under 11, 11–14 and 15–18 years).
Considering the 2000–2019 period, the number of cases increased in groups of patients with ages higher than 11 years and decreased in those under 11 years (Figure 6(a)). In 2000, the majority of the arthroscopies were done in 15- to 18-year-old patients, whereas in 2019, the higher number of surgeries was on 11- to 14-year-old subjects. In addition, there is a pronounced gap between under and over 11-year-old patients, which intensifies over time.

Paediatric arthroscopic surgeries are divided by age classes (<11, 11–14 and 15–18 years old) in G1 (a) and G2 (b).
In G2, excluding one centre due to a lack of age-related information for IRB reasons, the observations noticed in the G1 analysis were confirmed. In particular, the gap between under and over 11-year-old patients persists, with an increasing difference in time (Figure 6(b)).
Gender
One centre of G1 and, in addition, one of G2 were excluded due to a lack of age or gender-related information for IRB reasons.
Considering the 20-year period of G1, arthroscopies are quite similarly distributed between males and females, with a slightly higher number of interventions among females especially in recent years (116 in females vs 95 in males, Figure 7(a)).
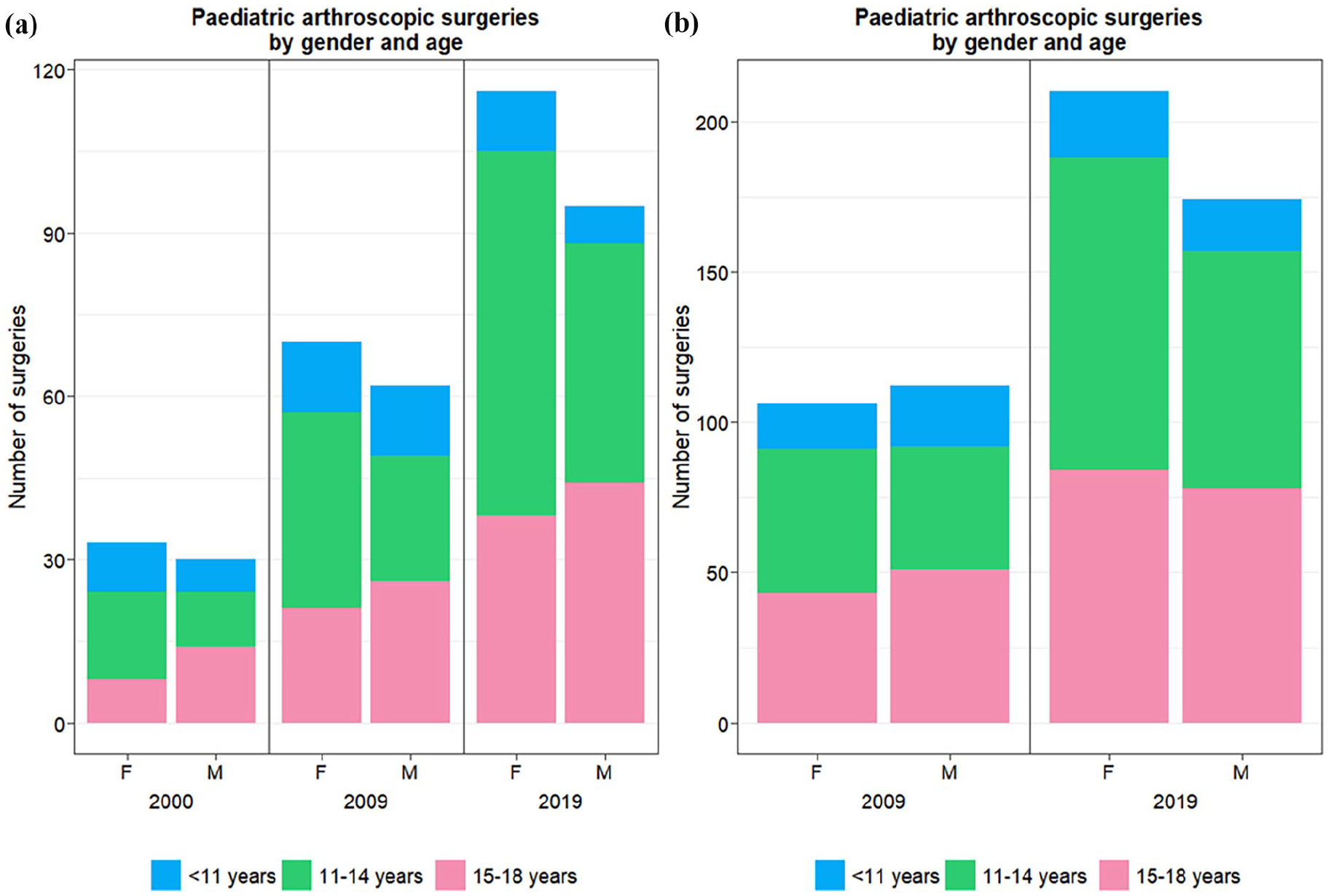
Paediatric arthroscopic surgeries are divided by gender and age class (<11, 11–14 and 15–18 years old) in G1 (a) and G2 (b).
There is a decrease in the ratio and total cases of female patients under 11 years old (among females, 27.3% were under 11 in 2000, while only 9.5% in 2019), whereas the percentage of older increases.
Considering only 2009–2019, data confirm an overall increase in the number of arthroscopies performed on female patients.
Discussion
This survey assesses the trend of paediatric arthroscopies in Europe over the last 20 years within surgical centres where this technique has consistently been practiced: given the rise in sports-related injuries and the technical advancements in arthroscopy, with smaller and precise instruments and implants, coupled with clearer imaging, there is an increase in these surgical procedures. This study is the first to identify an increase in arthroscopic surgical procedures in Europe.
There has been an increase in both the total number of paediatric orthopaedic surgical procedures and the number of paediatric arthroscopy procedures, as well as their ratio: an increasingly higher percentage of interventions on young patients is being performed using arthroscopy. We observed an 18.4% rise in the ratio since 2000, with a notably surprising 34% increase in the last decade in the proportion of arthroscopic procedures.
This European trend is confirmed when analysing the individual states that participated in this survey, except for Finland. In Finland, in the study institution, there has been a decrease attributed to different causes. First, there was a reduction in the number of diagnostic arthroscopies performed in the early 2000s when MRI capacity increased by two to three-fold. Another reason for the decreased need for diagnostic arthroscopies was the acquisition of the first 3T MRI during the later study period (2010–2019). In general, the availability of MRI is particularly high in Finland currently, when analysing the number of MRI units per inhabitant. 13 Furthermore, since 2002, there has been a shift towards MRI-guided joint-sparing perforations and bone transplantation instead of arthroscopy in treating OCD (osteochondritis dissecans) in the Finnish study centre, with further decline between 2009 and 2019. Keeping these backgrounds in mind, the current rate (4%) of arthroscopy versus all orthopaedic surgeries in Finland is in accordance with the other study countries (mean 6.7%), and still higher than another study centre in France. In addition, treatments for ACLs and menisci have remained stable in number between 2009 and 2019 in Finland, similar to what happens in other countries. A 20-year report on adult arthroscopy cases in Finland has highlighted a declining trend, particularly in diagnostic procedures and arthroscopic lavage for osteoarthritis: this decline follows a peak in 2006. 14 Recently, European countries demonstrated a decline in knee arthroscopies due to a change in guidelines regarding knee arthroscopy.15,16
Comparing the paediatric situation in Europe with the United States, Hosseinzadeh et al. reported an increase on case logs submitted for ABOS (
Over the observed period, our data indicated that the knee (84.39% in 2019) consistently remained the most affected anatomical region undergoing arthroscopic procedures, followed by the ankle (4.39%) and elbow (3.09%). The ABOS Part II examination database has shown that, similarly to our European registry, the anatomical region most affected in the United States has been the knee. 8
In the USA, the knee joint comprised an average of 52.1% of the respondents’ overall practice, ACL reconstruction being the most common procedure, followed by the shoulder (15.2%) with arthroscopic Bankart repair and labral repair/capsular plication, hip (13.9%) for femoral acetabular impingement increase, ankle (7.5%), elbow (7.1%), and wrist (4.2%) 21 : variations in popular youth sports between the United States (e.g. baseball and basketball) and Europe (e.g. soccer) could contribute to differing rates of arthroscopic procedures. Besides OCD and ankle instability, Kushare demonstrated the efficacy of arthroscopies for Ankle Impingement in paediatric athletes. 22 Andelman demonstrated an increasing prevalence of elbow arthroscopies in the paediatric population, encompassing not only cases related to OCD but also those involving abnormalities, contractures and fractures. 23 Surprisingly, our experience revealed that shoulder arthroscopies accounted for only 0.65% of the procedures conducted, despite Imam’s review revealing an increased prevalence for instability, brachial plexus birth palsy and rotator cuff tears. 24
Regarding age, we observed a decrease in the number of arthroscopies in patients under 11: there was a gap between over and under 11, which intensifies over the years. This could be attributed to a reduction in injuries within this age group, possibly due to increased focus on prevention and non-contact activities in this period. However, unlike our European registry, North America has experienced an increase in cases of sports medicine in individuals under 13 years of age. 8 Buller et al. 7 documented a 37% rise in the instances of ACL reconstructions in the United States from 1994 to 2006. Notably, the most substantial increase (924%) was observed among patients below the age of 15.
Our data did not show a gender-based difference over time in the number of arthroscopies: in 2000, the percentage was 52.4%, and, it had increased to 55% by 2019 for females. As mentioned earlier, there was a significant decrease in female patients under the age of 11, with a ratio decline of 65.2% over 20 years. Previous study suggested that males were more likely to have had sport-related injury due to a different competitive approach, type of traumatic sport and time spent doing sport. 25 These changes may change as the gender gap in contact sport continues to narrow. Focusing on the most prevalent joint, the Norwegian National Knee Ligament Registry showed that the gender difference in ACL reconstruction starts at the age of the growth spurt, increases during adolescence, then reduces. 26
This study is not exempt from limitations. Primarily, the absence of survey validation and the possibility of question misinterpretation may have led to biased findings. The main constraint is the potential lack of representativeness in the surveyed population, as the questionnaire was exclusively distributed among members of EPOS Sport Study Group and therefore may not be scalable to all the patients treated within Europe: an unified, European registry for all paediatric arthroscopy procedures could mitigate data collection bias, facilitate future research, minimize discrepancies among participating centres and improve the comprehensiveness and accuracy of the data. It also does not cover a wide geographical spread of countries where practices any differ. Trends found in this study may not be generalizable to the hospitals without surgeons specialized in paediatric sports medicine. Our survey’s inability to distinguish between diagnostic and interventional procedures presents an opportunity to explore the evolution of diagnostic arthroscopy practices over time.
Conclusion
Our study reveals a positive trend in paediatric arthroscopy in Europe, showing a significant increase in procedures over the past 2 decades: the increase in the number of procedures within institutions that have historically performed a substantial volume of surgeries suggests a noteworthy growth in paediatric arthroscopy. Advances in techniques, instrumentation miniaturization and enhanced knowledge of paediatric injuries have facilitated a surge in procedures, extending to new anatomical areas with favourable outcomes. Further studies to better characterize and investigate the reasons of these results are recommended.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241302997 – Supplemental material for An increase in paediatric arthroscopy in Europe: Experience of the EPOS Sport Study Group
Supplemental material, sj-pdf-1-cho-10.1177_18632521241302997 for An increase in paediatric arthroscopy in Europe: Experience of the EPOS Sport Study Group by Marco Turati, Marco Crippa, Nicolas Nicolaou, Elena Tassistro, Jaakko Sinikumpu, Aurelien Courvoisier, Marcus Mumme, Julio Duart, Monika Thüsing, Marco Bigoni and Franck Accadbled in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Declaration of conflicting interests
Funding
Ethical approval
Informed consent
Submission declaration
ORCID iDs
Supplemental material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.