
Abstract
Keywords
Introduction
Hypertension has long been the most common disease worldwide, with an estimated global prevalence of 1.13 billion people in 2015. 1 In China, according to the latest data from a nationwide survey on hypertension from 2012 to 2015, the adult age-weighted prevalence of hypertension was 23.2%. 2 The 2017 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the prevention, detection, evaluation, and management of high blood pressure (BP) in adults revised the cutoff for diagnosing hypertension to ⩾130/80 mm Hg; this means that the prevalence of hypertension will increase to 46% in the USA, 3 and to 46.4% in China, which is twice as high as that based on current Chinese guidelines. 4 Studies show that control of high BP can result in significant risk reductions in cardiovascular morbidity and mortality. 5 Office BP measurement (OBPM) has been the standard for diagnosing and managing hypertension; however, results may be confounded by several factors and are limited by time and location. To improve the rates of detection and control of high BP in the general population, guidelines from different countries and organizations have proposed several recommendations. These academic statements concur in their recommendations for using out-of-office BP monitoring in patients with hypertension or in high-risk populations.3,4,6–8 For example, the 2017 ACC/AHA guidelines included an IA (Class of Recommendation and Level of Evidence) recommendation for out-of-office BP measurement to confirm the diagnosis of hypertension and to titrate BP-lowering medications. 3 The 2018 European Society of Cardiology/European Society of Hypertension guidelines for the management of arterial hypertension also recommended that out-of-office BP measurements should be used to confirm a diagnosis of hypertension, 6 and the 2018 Chinese guidelines for the prevention and treatment of hypertension recommended that, if available, out-of-office BP monitoring should be implemented to diagnose white coat hypertension (WCH) and masked hypertension (MH), or to evaluate the effects of antihypertensive treatment. 4
In addition to its use for diagnosing and managing hypertension, out-of-office BP may be practical in screening for hypotension, identifying circadian BP patterns and BP variability, and risk stratification for BP-related target organ damage and mortality. This review aims to summarize the current evidence for the applications of out-of-office BP monitoring, including home blood pressure monitoring (HBPM) and ambulatory blood pressure monitoring (ABPM), with regard to current studies on cardiovascular disease (CVD).
General characteristics of OBPM, HBPM, and ABPM
OBPM is measured by a nurse or doctor with a conventional calibrated mercury sphygmomanometer or an electronic device in the clinic. HBPM, also called self-BP monitoring, is performed by the patient or a family member in a familiar environment, providing at-home long-term BP values. ABPM offers abundant information on 24-h profiles including nocturnal BP and short-term BP variability. The general characteristics of OBPM, HBPM, and ABPM are listed in Table 1.
The general characteristics of OBPM, HBPM, and ABPM.
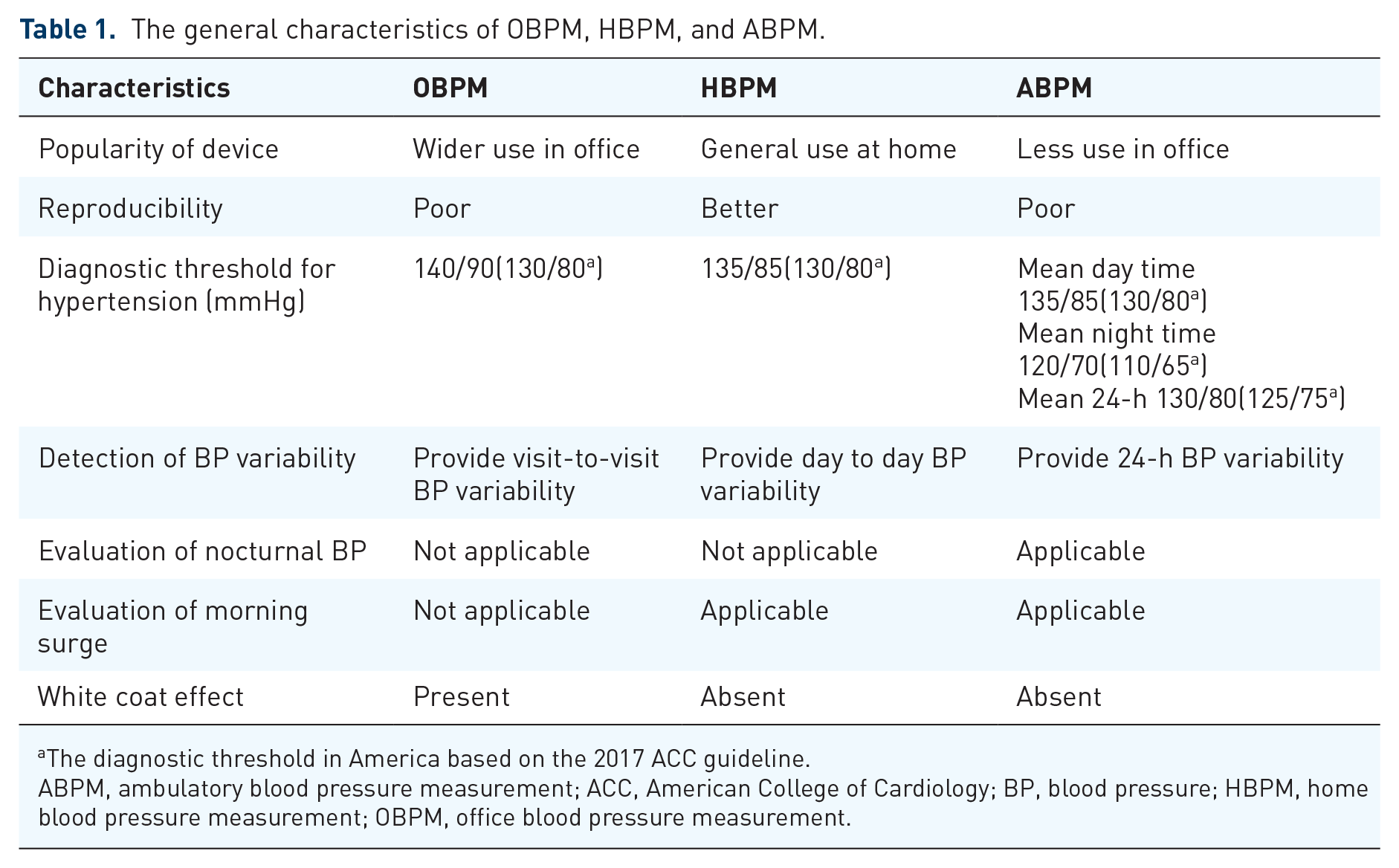
The diagnostic threshold in America based on the 2017 ACC guideline.
ABPM, ambulatory blood pressure measurement; ACC, American College of Cardiology; BP, blood pressure; HBPM, home blood pressure measurement; OBPM, office blood pressure measurement.
Applications for out-of-office BP monitoring
Detecting WCH and MH
Combining OBPM and out-of-office BP readings, BP phenotypes can be divided into normotension, WCH, MH, and sustained hypertension. WCH is defined as an elevated in-office BP and normal out-of-office BP, while MH defines patients with normal in-office BP but with elevated out-of-office BP measurements (Figure 1).

Classification of BP subtypes by combination of clinic office BP and out-of-office BP.
Studies report that overall prevalence of WCH in the general population is 9–23%,9–13 and that WCH accounts for 30–40% of patients with elevated OBPM.
6
WCH has long been considered a benign phenomenon because numerous epidemiological studies found no association between WCH and target organ damage.14,15 Although some observational studies and meta-analyses showed that WCH was associated with subclinical target organ damage, the cross-sectional design of these studies failed to prove causality.16,17 Recently, our large-scale meta-analysis found that, after multivariate adjustment, WCH was associated with an increased risk of CVD and all-cause mortality in individuals without antihypertensive treatment at baseline compared with normotensive counterparts. It is interesting that the risks of CVD and mortality are similar in patients with WCH who receive antihypertensive therapy (‘treated’)
MH is defined as elevated out-of-office BP and normal office BP, and has been generally considered harmful and to require appropriate treatment. The prevalence of MH ranges from 6.7% to 20% in different reports.13,22,23 In the Spanish cohort study, after adjusting for multiple risk factors, MH defined by ABPM was strongly associated with all-cause mortality (HR: 2.83; 95% CI: 2.12–3.79) and cardiovascular mortality (HR: 2.85; 95% CI: 1.66–4.90). 19 Another cohort study including 4261 Japanese patients also concluded that MH based on HBPM was associated with an increased risk of stroke (HR: 2.66; 95% CI: 1.15–6.13). 24
It should be noted that in individuals with prehypertension defined according to office BP (120–139/80–89 mm Hg), a large proportion would be classified as MH if out-of-office BP monitoring was performed. The International Database on Ambulatory BP in relation to Cardiovascular Outcomes (IDACO) study revealed that, in people with prehypertension, 29.3% would be diagnosed as having MH if ABPM was performed. The Masked Hypertension Study also showed that 34.1% of participants defined as prehypertensive were confirmed to be MH under ABPM. 25 In addition, the International Database of HOme BP in relation to Cardiovascular Outcome (IDHOCO) study revealed similar findings by HBPM, stating that MH accounted for 18.4% and 30.4% of patients with low-range (120–129/80–84 mm Hg) and high-range (130–139/85–89 mm Hg) prehypertension, respectively. Without out-of-office measurements, a large number of patients with MH could be misdiagnosed, which might result in inappropriate treatment. Our series studies showed that prehypertension is associated with an increased risk of all-cause mortality, CVD, and end-stage renal disease.26–32 However, whether this target organ damage is caused by undetected MH or prehypertension is unclear and requires further studies. Based on data from the studies cited previously, out-of-office BP measurement, either HBPM or ABPM, is highly recommended for the detection of WCH or MH in suspected individuals.
Prognostic predictive power of out-of-office BP for target organ damage and mortality
Given the limitations of OBPM, the prognostic predictive power for target organ damage of in-office BP may be lower than that of out-of-office BP. Because of rapid developments in electronic technology, numerous studies comparing the prognostic predictive power of out-of-office BP and office BP have been performed. The Finn-Home study showed that HBPM is strongly correlated with cardiovascular risk, 33 and is a stronger predictor of left ventricular hypertrophy and atherosclerosis than office BP.34–36 The Spanish cohort study demonstrated that 24-h systolic BP was a better predictor of all-cause mortality (HR: 1.58 per 1-standard deviation increase in ABPM; 95% CI: 1.56–1.60, after adjusting for OBPM) than office systolic BP (HR: 1.02; 95% CI: 1.00–1.04, after adjusting for 24-h ambulatory BP). 19 Other studies drew a similar conclusion, namely that HBPM or ABPM can better predict cardiovascular events or other target organ damage.37–46 Therefore, people who are at high risk, or have elevated BP, should consider out-of-office measurements, which are stronger predictors.
However, it should be noted that currently there are limited data to support the proposal of whether, in the general population, the use of out-of-office BP instead of office BP in CVD risk scoring systems can provide further incremental value for CVD prediction. Data from a Swedish cohort study showed that, although ambulatory systolic BP was an independent risk factor for CVD, addition to the Framingham Risk Score led to only small increases to the overall model fit, discrimination (a 1% increase in the area under the receiver-operating characteristic curve), calibration, and reclassification. 47 Recently, another study also showed that using BP measurements obtained through ABPM or HBPM instead of OBPM may have little effect on CVD risk estimates obtained from the Framingham, QRISK2 (risk of developing a heart attack or stroke over the next 10 years), or SCORE (Systematic COronary Risk Evaluation) risk equations. 48 Therefore, current cardiovascular risk assessment systems, including China-PAR (Prediction for Atherosclerotic CVD [ASCVD] Risk in China), 49 European SCORE, 50 ASCVD-PCE (Pooled Cohorts Equations) of the USA, 51 the Q risk score (QRISK) model of Great Britain, 52 and the Framingham Risk Score, 53 include only clinic BP in the model. However, all of these cardiovascular risk assessment systems were developed in the general population. In patients with abnormal BP phenotypes, such as WCH or MH, current CVD risk assessment systems may over- or underestimate the risk. Further studies are needed to explore whether incorporation of out-of-office BP has incremental value for CVD prediction in people with abnormal BP phenotypes.
Better BP control
The Telemonitoring or Self-Monitoring of BP in Hypertension (TASMINH4) trial is a parallel randomized controlled trial that was performed in the United Kingdom that aimed to evaluate the efficacy of self-BP monitoring, telemonitoring, and usual care in BP control. In this trial, participants were assigned randomly (1:1:1) to a self-monitoring group, a telemonitoring group, or a usual care group. After 12 months, both self-monitoring and telemonitoring groups had a lower BP level than the usual care group (137.0 ± 16.7 and 136.0 ± 16.1,
Good BP control plays a pivotal role in reducing the prevalence of CVD. A meta-analysis showed that every 5-mm Hg decrease in systolic BP was associated with a 13% lower risk of cardiovascular events, and a 2-mm Hg decrease in diastolic BP was associated with a 12% lower risk of cardiovascular events.
64
However, evaluation of the association between BP reduction and CVD was based on office BP values; studies on BP treatment goals based on HBPM or ABPM are limited. Current academic guidelines recommending initiating treatment and determining BP goals for managing hypertension are still based on OBPM.3,4,6,7 Several ongoing studies are evaluating the use of out-of-office BP monitoring to guide hypertension control. The TELEBPMET (a randomized controlled study based on home BP telemonitoring
Out-of-office BP monitoring for screening hypotension
Hypotension is usually defined as OBPM < 110/70 mm Hg, daytime ABPM < 105/65 mm Hg, or 24-h ABPM < 100/60 mm Hg. 68 Although the ‘J curve’ phenomenon is still controversial,69–71 lower BP readings are undoubtedly not an improvement.68,71 The Systolic Blood Pressure Intervention Trial showed that patients with hypertension and high CVD risk assigned to an intensive BP treatment goal (systolic BP < 120 mm Hg) experienced lower CVD risk but also increased risk of severe hypotension and syncope. 72 In a study including 70,997 patients with hypertension receiving antihypertensive treatment, one in eight patients was at risk of hypotension, and ABPM could better screen for hypotension than OBPM. 68
Orthostatic hypotension, a usually asymptomatic condition whereby BP drops when rising to a standing position, has been confirmed to be associated with cardiovascular events and dementia.73–77 Although it is not difficult to diagnose, orthostatic hypotension is rarely screened using OBPM unless obvious symptoms develop. A study by Cremer and colleagues showed that HBPM is better than OBPM in screening for orthostatic hypotension. 78 Another study showed that ABPM can predict autonomic dysfunction in orthostatic hypotension, 79 and may be useful when assessing patients for orthostatic hypotension. 80 Postprandial hypotension occurs when systolic BP decreases by more than 20 mm Hg within 2 h after a meal. Some studies have shown that this condition also results in an increased risk of stroke, cerebrovascular damage, syncope, and mortality,81–83 and that HBPM is a suitable screening method. 83
Based on these findings, out-of-office BP monitoring is a good choice for screening for hypotension (including orthostatic and postprandial hypotension) in patients with hypertension receiving antihypertensive treatment (especially older patients) or with normal BP with autonomic dysfunction. If hypotension is documented, modifying a patient’s antihypertensive medication or other interventions should be considered. In addition, future studies should focus on individual therapy and optimal thresholds for patients with hypertension in order to avoid undetected hypotension.
Identifying BP variability, circadian BP patterns, and other special BP phenotypes
Variability is an intrinsic property of BP. In patients with regular follow-up, long-term visit-to-visit BP variability is associated more strongly with cardiovascular and all-cause mortality than mean BP. 84 HBPM may be more suitable for determining long-term BP variability because it can improve patients’ adherence to BP monitoring. The Didima study showed that, in the general population with a 19-year follow up, systolic home BP variability exhibited superior prognostic ability compared with office BP. 85
Although long-term BP variability is not available through ABPM, ABPM can provide short-term variability data when variability is defined as the average variation of BP throughout the day and the circadian rhythm. Based on 24-h BP profiles, normal BP circadian rhythm is defined as dipping BP with a decrease of 10–20% at night compared with daytime. Accordingly, other circadian BP patterns, including extreme dipping (>20% drop), nondipping (<10% drop), and reverse dipping (reversely increased) BP, are also defined by night-time mean BP compared with daytime BP. 86 Furthermore, ABPM is useful for detecting other special BP phenotypes, such as isolated nocturnal hypertension and morning BP surge. Nondipping BP,87–89 reverse dipping BP,90,91 nocturnal hypertension,92,93 and morning BP surge88,89,94,95 are associated with an increased risk of target organ damage.
Compared with ABPM, HBPM has been criticized as being inconvenient for the monitoring of circadian BP patterns and nocturnal hypertension. However, recent studies showed that HBPM provided similar values and had close agreement in detecting nondipping BP, as well as target organ damage, compared with ABPM.96,97 However, because of limited available data, additional studies focusing on circadian BP patterns, BP variability, and special phenotypes detected by HBPM are required to determine the optimal strategies for managing hypertension based on out-of-office measurements, and thus reduce adverse outcomes.
Conclusion
Although out-of-office BP monitoring is beneficial, it is not as widely used as we propose. Regarding ABPM, the relatively higher expense, interference with daily activities, and inaccurate readings due to incorrect measuring position are the main reasons for its low rate of use. HBPM, moreover, requires formal skills training and is limited by nocturnal BP detection, recording bias, and arbitrary self-modification of treatment by anxious patients. Given their advantages and disadvantages, HBPM and ABPM should be considered to be complementary rather than competitive in managing hypertension. Our proposed clinical procedure for using out-of-office BP monitoring is presented in Figure 2.

Proposed clinical procedure for application of out-of-office BP monitoring.
To better incorporate out-of-office BP monitoring into clinical practice, initiatives should also be taken regarding the following. First, physicians need to be aware of the indications and limitations of out-of-office BP measurement. Second, patients should receive clearer instructions, training, and education regarding BP monitoring. Third, ideally, governments and public health researchers will engage in efforts to address cost-effective methods of out-of-office BP monitoring. Fourth, combining remote data transmission with clinic-centered monitoring is helpful in avoiding the drawbacks of HBPM, such as recording bias and arbitrary self-modification of treatment, in further improving BP control. We are currently performing the Home Blood Pressure Monitoring Cohort Study Based On Intelligent Cloud Platform (HBPM-iCloud) trial to evaluate HBPM for predicting the risk of CVD and mortality in a large Chinese population.
In conclusion, based on recent clinical studies, out-of-office BP measurements have benefits with regard to the following areas: detecting certain abnormal BP phenotypes, namely, WCH and MH; stronger prediction of determining the prognosis regarding target organ damage and mortality; better BP control; hypotension screening; and offering a unique approach to identifying circadian BP patterns and BP variability.