
Abstract
Introduction
Hip resurfacing with metal–metal friction seemed an attractive option in the young patient group due to its bone-conserving nature, with possible simple revision and the large head contributing to greater stability. It was also conceptually sound as it dealt with arthritis as a disease of the joint and not of the whole head and neck. We present a case report of pseudotumor associated with metal-on-metal (M-M) hip resurfacing.
Case report
A 47-year-old man with ankylosing spondylitis underwent surgery 7 years ago to implant an M-M hip resurfacing ASR™ (DePuy, Warsaw, IN, USA) in the right hip. The patient attended the clinic complaining of progressive pain in the right groin exacerbated by stair climbing, getting into or out of bed and rising from seated position, but does not affect his ability to walk. A plain radiograph showed the arthroplasty in good position with no signs of failure (Figure 1). High levels of metal ions appeared in blood analytical studies (56.7 ppb chromium, 63.2 ppb cobalt) and urine (163.7 ppb chromium, 628.6 ppb cobalt). A magnetic resonance imaging (MRI) study was performed (Figure 2). The patient was revised to remove the arthroplasty and reimplant a conventional metal-on-polyethylene model. In this revision surgery, we found a pseudotumor and profuse metallosis area with inflammatory reaction and partial destruction of the femoral neck (Figure 3). After 3 months, analytical studies showed 22.9 ppb of chromium and 2.9 ppb of cobalt in blood and 33 ppb of chromium and 8.9 ppb cobalt in urine. The patient is asymptomatic after 2 years of revision surgery.

X-ray: the implant position is correct with no signs of failure.

MRI: STIR-weighted and T1 images showed a bulky periprosthetic fluid collection above and below acetabular (arrows) component, with areas of low signal within it (arrowheads) due to metal debris.
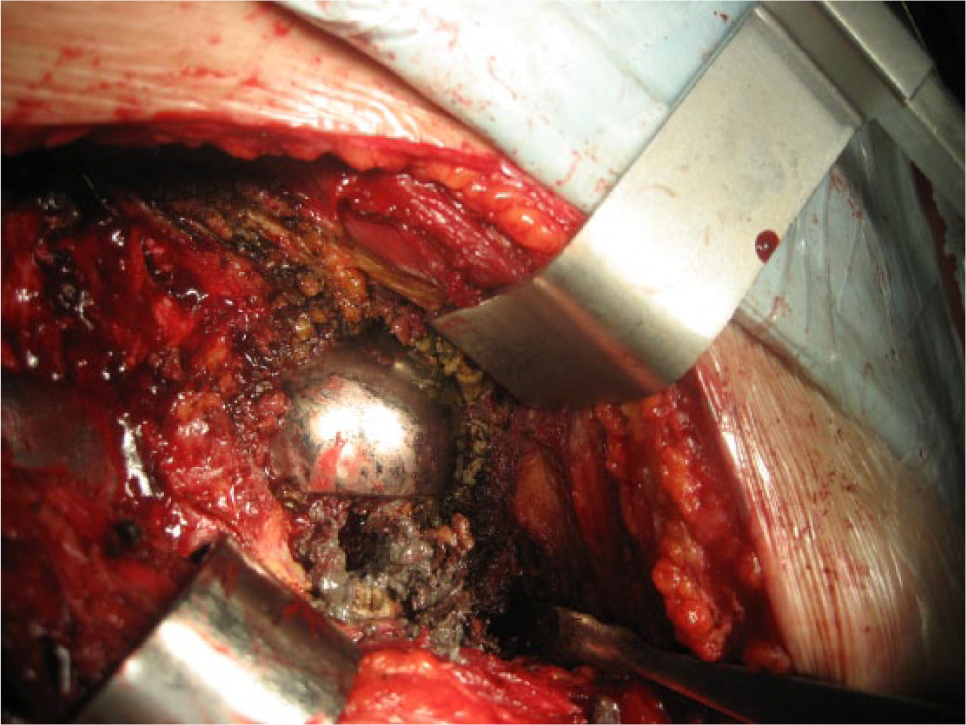
Metallosis tissue and metal debris in revision surgery. Osteolysis in femoral neck.
Discussion
With the introduction of resurfacing arthroplasty and the increasing use of various M-M articulations, groin pain has once more been reported as a complication. 1 M-M articulation in total hip replacement (THR) has a higher prevalence of groin pain. This is well known to orthopedic surgeons. The aim of this case study is to report this event to other physicians: rheumatologists, general practitioners or internal medicine.
Bartelt et al. 2 reported groin pain in 7% of metal-on-polyethylene or ceramic-on-ceramic THRs, 15% of M-M and 18% of M-M resurfacings. The articular surface replacement (ASR) prosthesis has recently been recalled for unacceptably high revision rates. Langton et al. 3 reported that in a series of 660 M-M hip resurfacings, 3.4% of ASR components required revision. Metal hypersensitivity, synovitis due to elevated metal ion levels or adverse local tissue reactions (formerly aseptic lymphocytic vasculitis–associated lesions (ALVAL)) should be considered in persistent groin pain and no evidence of infection, loosening, fracture or iliopsoas tendonitis. Many articles have been published recently 4 on the subject of pseudotumors surrounding M-M hip resurfacing and replacement prostheses. These pseudotumors are sterile, inflammatory lesions within the periprosthetic tissues and have been variously termed masses, cysts, bursae, collections or ALVAL. The prevalence of pseudotumors in patients with a well-functioning M-M hip prosthesis is not well known. A periprosthetic cystic pseudotumor was diagnosed commonly in 60% of patients with the use of metal artifact reduction sequence MRI. The prevalence of pseudotumors was similar in patients with a well-functioning hip prosthesis, patients with a painful hip, patients with a well-positioned acetabular component, both men and women and symptomatic and asymptomatic hips.
Although MRI is useful for surgical planning, the presence of a cystic pseudotumor may not necessarily indicate the need for revision arthroplasty. Previous studies 5 suggest that there are two kinds of lesions: fluid collections and soft-tissue masses; these lesions may be asymptomatic and are associated with reactions to metal wear particles on histology. Therefore, according to the current evidence base, a lesion on MRI is not synonymous with the need for intervention.
The US Food and Drug Administration (FDA) 6 recommends orthopedic surgeons to consider performing special imaging tests, joint aspiration and blood tests, including ion levels on symptomatic patients with an M-M THR. Blood tests include an erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), which can be elevated with either infection or adverse local tissue reaction. When the blood or serum ion levels are <2 ppb, there is a low risk of this complication. When the levels are >7 ppb, the risk is increased. For other authors, 7 preoperative testing of serum ion levels was not helpful in identifying patients with or without soft-tissue damage related to a failed M-M THR. Both Co and Cr levels had poor sensitivity and specificity for tissue damage found at revision. Furthermore, some authors 8 found that the arbitrary cutoff value of 7 ppb was not a predictor of tissue damage. Any patient with even minimal symptoms in the presence of M-M total hip arthroplasty should be counseled with regard to management of symptoms.
Conclusion
We presented a patient with groin pain in an M-M hip prosthesis with normal X-ray and without other symptoms. Neither the symptoms nor the presence of cysts in MRI and high levels of Cr and Co in blood have enough predictive value taken one by one. Only the confirmation of a progressive elevation of metal levels in the presence of periarticular cysts and/or groin pain would force a revision surgery.