
Abstract
Introduction
Interferon (IFN) betas are effective therapies for the treatment of relapsing multiple sclerosis (RMS) and are typically viewed as having a good safety and tolerability profile.1,2 The most prevalent adverse events (AEs) across all IFN betas are flu-like symptoms (FLS) and injection site reactions (ISRs), which are both commonly reported reasons for non-adherence (i.e. not taking a therapy as prescribed).3,4 Pivotal IFN trials have demonstrated that FLS occur in 49–59% of patients and ISRs with subcutaneous administration occur in 78–92% of patients.5–7 Better adherence has been associated with improved clinical outcomes and quality of life, as well as reduced hospitalization and healthcare costs8,9; therefore, reductions in the frequency or severity of AEs related to non-adherence such as FLS may improve RMS treatment outcomes.
Peginterferon beta-1a is an IFN beta-1a formulation that has been pegylated, providing it with a longer half-life than other IFN beta formulations. It is approved for the treatment of patients with RMS and is administered subcutaneously at a dose of 125 μg every 2 weeks, the lowest injection frequency approved for IFN beta in multiple sclerosis (MS). In the pivotal phase 3 ADVANCE trial, patients receiving peginterferon beta-1a every 2 weeks exhibited a 36% reduction in the annualized relapse rate compared with patients receiving placebo (
In clinical practice, patients initiating peginterferon beta-1a may be switching from other IFN therapies, so it is valuable to understand changes in FLS incidence and severity in these transitioning patients. The high proportion (83%) of treatment-naive patients in the ADVANCE study precluded such analysis. 10 The ALLOW study was therefore specifically designed to evaluate the safety and tolerability of switching from non-pegylated IFN to peginterferon beta-1a. This study also examined FLS management in patients who have transitioned from non-pegylated IFN to peginterferon beta-1a. The primary objective was to evaluate the proportion of patients who experienced new or worsening FLS. This study also aimed to determine whether long-acting non-steroidal anti-inflammatory prophylactic treatment (naproxen) has a greater impact on FLS during peginterferon beta-1a treatment than does standard clinical practice at the discretion of the treating neurologist. FLS onset and duration following peginterferon beta-1a injection versus non-pegylated IFN were also compared. As another aspect of ALLOW, the Delphi method was used to characterize peginterferon beta-1-associated ISRs and to obtain consensus on ISR management strategies; Delphi results have previously been published. 13
Patients and methods
Study design and participants
ALLOW was a 1-year, multicenter, open-label phase 3b study to characterize FLS in patients with RMS who transitioned from their current non-pegylated IFN beta therapy to peginterferon beta-1a. A total of 251 patients on a stable dose of non-pegylated IFN were screened during a 4-week screening/run-in period (weeks −4 to 0) on their current medication. At week 0 (baseline), 201 eligible patients initiated treatment with subcutaneous peginterferon beta-1a in accordance with the approved treatment initiation schedule (63 μg at week 0, 94 μg at week 2, and 125 μg at week 4, with 125 μg administered every 2 weeks for all subsequent weeks). Week 0 also began an 8-week phase during which naproxen (500 mg) was compared with the patients’ existing FLS management regimen. The 201 patients who initiated treatment with peginterferon beta-1a were randomly assigned (1:1) to receive either their current FLS management regimen as determined by the prescribing neurologist or naproxen 500 mg twice daily. In patients randomly assigned to the naproxen arm, naproxen 500 mg was administered up to 24 hours before peginterferon beta-1a treatment and continued for 48 hours after injection. Thirty-eight sites in the USA randomly assigned patients using an interactive voice/web response system (Endpoint, San Francisco, CA, USA). Following this 8-week treatment phase, patients entered the monitoring phase (weeks 8–48), in which they continued receiving peginterferon beta-1a treatment and either their treatment-phase FLS management regimen or a regimen chosen by their investigator.
The study included patients aged 18–65 years with RMS and an Expanded Disability Status Scale score of 5.0 or less who had been treated with a stable dose of non-pegylated IFN beta for 4 or more months immediately prior to screening/run-in. Other key exclusion criteria were prior treatment with peginterferon beta-1a, prespecified laboratory abnormalities, and the occurrence of an MS relapse within 50 days of study baseline. Supplementary Table 1 provides a full list of inclusion and exclusion criteria. To ensure a good representation of the subcutaneous IFN beta-1a patient population, no more than 50% of patients could be transitioning from intramuscular IFN beta-1a.
The protocol was approved by the institutional review board at each site and the study was conducted according to the International Conference on Harmonisation Guidelines for Good Clinical Practice and the Declaration of Helsinki. Every patient provided written informed consent before entering the study. This trial is registered with ClinicalTrials.gov (number NCT01939002).
Study procedures and endpoints
FLS severity scores (FLS-S), based on the FLS severity scale, 14 were recorded by the patient using a study-provided electronic diary at pre-injection (1 hour or less prior to the scheduled peginterferon beta-1a injection) and post injection (within every 6 hours after the injection and within every 6 hours for at least 48 hours until FLS symptoms had stopped). Patients reported an FLS-S from 0 to 3 describing the severity of each of the following categories: muscle aches, chills, fatigue, and body temperature. Muscle aches, chills, and fatigue were each rated from 0 to 3: ‘0’ for absent; ‘1’ for mild, did not interfere with daily activities; ‘2’ for moderate, sufficient to interfere with daily activities; and ‘3’ for severe, bedrest required. Patients’ body temperatures were also assigned a score from 0 to 3: ‘0’ if less than 99.1°F, ‘1’ if 99.1°F or greater but less than 100.1°F, ‘2’ if 100.1°F or greater but less than 101.1°F, and ‘3’ if 101.1°F or greater. The total FLS-S was calculated as a sum of the three symptoms scores and the fever score, for a score ranging from 0 to 12. A mean increase of 2 points or more was considered worsening.
The primary endpoint was the proportion of patients experiencing new and/or worsening FLS, defined as an increase of 2 points or more in total FLS-S during the first 8 weeks of peginterferon beta-1a (the treatment phase) after switching from non-pegylated IFN beta. Secondary endpoints evaluated at baseline, 12 weeks, and 48 weeks included the severity of FLS, the impact of naproxen (500 mg twice daily) on FLS, the onset and duration of FLS following injection with peginterferon beta-1a, the incidence of AEs, and the Patient-Determined Disease Steps (PDDS) score.15–17 Total time experiencing FLS over the 4 weeks before and after switching to peginterferon beta-1a was examined as a post hoc analysis.
Statistical analysis
For this exploratory study, the sample size calculation was not based on statistical power considerations but aimed to provide meaningful data to evaluate the proportion of patients experiencing FLS. Assuming 25% (the best possible case) to 39% (the worst possible case) of the patients in this study would experience FLS, with a sample size of 160 patients, the upper and lower 95% confidence bounds of the estimated proportion would extend 6.7% to 7.6% from the assumed proportion (25% to 39%) of subjects who would experience FLS during the study. Assuming a 20% dropout rate, the target sample size was 200 patients.
For the primary analysis, a one-sample chi-square test was used to test the null hypothesis that 25% of enrolled patients would have FLS after switching to peginterferon beta-1a. New or worsening FLS were defined as a 2-point-or-more increase in FLS-S during the first 8 weeks of peginterferon beta-1a treatment compared with the 4-week run-in period.
18
FLS severity, onset, and duration were summarized using mean (standard deviation) and median (minimum and maximum) values. FLS management regimen groups were compared using a
Results
Patient disposition and baseline characteristics
Patient demographics and baseline disease characteristics were generally well balanced in the two treatment groups (Table 1). The mean patient age was older and time with RMS since diagnosis was longer than typically observed in the RMS pivotal clinical trials, a reflection of a study design that required a treatment-experienced group. The median (range) of the duration of previous IFN use was 93.9 (4.0–278.4) months for patients remaining on their current FLS regimen and 72.1 (1.3–336.4) months for patients randomly assigned to naproxen. All other patient characteristics were similar to those found in typical phase 3 RMS trials. 10
Baseline characteristics of patients enrolled in the ALLOW study.

FLS: flu-like symptoms; SD: standard deviation; MS: multiple sclerosis.
Before transitioning to peginterferon beta-1a, 50.8% of patients used intramuscular interferon (IFN) beta-1a, 27.3% used subcutaneous (SC) IFN beta-1a, and 18.9% used SC IFN beta-1b; 82% of patients completed the study.
*Data missing for 1 patient in cohort.
Patients
In total, 201 patients (103 in the current FLS regimen and 98 in the naproxen group) from 38 sites received at least one dose of medication (Figure 1). The first patient was dosed on 6 November 2013, and the study was completed on 13 November 2015. Overall, 164 patients completed the study (81.6% in each group). AEs were the most common reason for study withdrawal in each group (with 12.6% of patients on the current FLS regimen and 13.3% of patients in the naproxen group withdrawing on this basis). Almost all patients (99.5%) used concomitant medications during the study, including analgesics, antipyretics, and vitamins. Concomitant medications used by more than 20% of patients in the study were ibuprofen (46.3%), naproxen (32.8%), and paracetamol (25.9%) (Supplementary Table 2).

Patient disposition. FLS: flu-like symptoms.
FLS and other AEs
Of the 194 patients in the efficacy population, 174 (89.7%) reported at least one occurrence of FLS during the 4-week screening/run-in period. A total of 174 patients (89.7%) also reported an FLS-S score greater than 0 in the first 8 weeks of the study following the transition to peginterferon beta-1a; only 20 (10.3%) of these were new or worsening FLS events, significantly less than the null hypothesis best case of 25% (
To determine whether there were any differences between the intramuscular IFN beta-1a and subcutaneous IFN beta-1a/b patient groups, the change in each group in the proportion of patients experiencing new and/or increased FLS between the 4-week run-in period and the first 8 weeks of peginterferon beta-1a was compared. There was no significant difference in new and/or increased FLS between patients previously receiving intramuscular IFN beta-1a and those previously receiving subcutaneous IFN beta-1a/b (12.4% (
FLS severity was low during the 4-week screening/run-in period prior to the initiation of peginterferon beta-1a and remained low over 48 weeks of treatment (Figure 2). Patients randomly assigned to the naproxen FLS treatment regimen did not experience a significant change in FLS severity compared with patients who maintained their current FLS treatment regimen.

Severity of flu-like symptoms (FLS) over 48 weeks. The mean overall FLS severity score (FLS-S) on non-pegylated interferons during the 4-week screening/run-in was 1.13. The overall minimum and maximum duration during the 4-week screening/run-in on prior interferon (IFN) were 0 and 7.3, respectively; the overall FLS-S minimum and maximum during 48 weeks on peginterferon beta-1a were 0 and 6.5, respectively. Only data up to 48 hours post-injection are included. The number of patients indicates patients recording an FLS-S score greater than 0. (Pre-dose data are not used.) bid: twice a day.
Overall, the median duration of FLS following injection was 17.0 hours (interquartile range 12–22 hours) over 48 weeks. The median FLS duration following injection was 3.2 hours longer with peginterferon beta-1a than with the prior non-pegylated IFN (median 17.0 vs. 13.8 hours;

Median duration of flu-like symptoms (FLS) post-injection over 48 weeks. The median duration (in hours) of FLS for a treatment is defined as the sum of hours from the treatment to 48 hours with a FLS score greater than 0. Pre-dose data were not used. The overall FLS duration minimum and maximum on prior interferon (IFN) were 6.00 and 42.86, respectively; on peginterferon beta-1a it were 6.00 and 39.00, respectively.
While the median duration of FLS was greater per injection with peginterferon beta-1a compared with the prior IFN, the total time experiencing FLS decreased with peginterferon beta-1a due to the reduced frequency of drug administration. The mean cumulative FLS duration during weeks 0–4 and 5–8 of peginterferon beta-1 treatment was 28.2 and 19.7 hours, respectively, compared with 85.3 hours during the 4-week run-in period on the prior IFN (
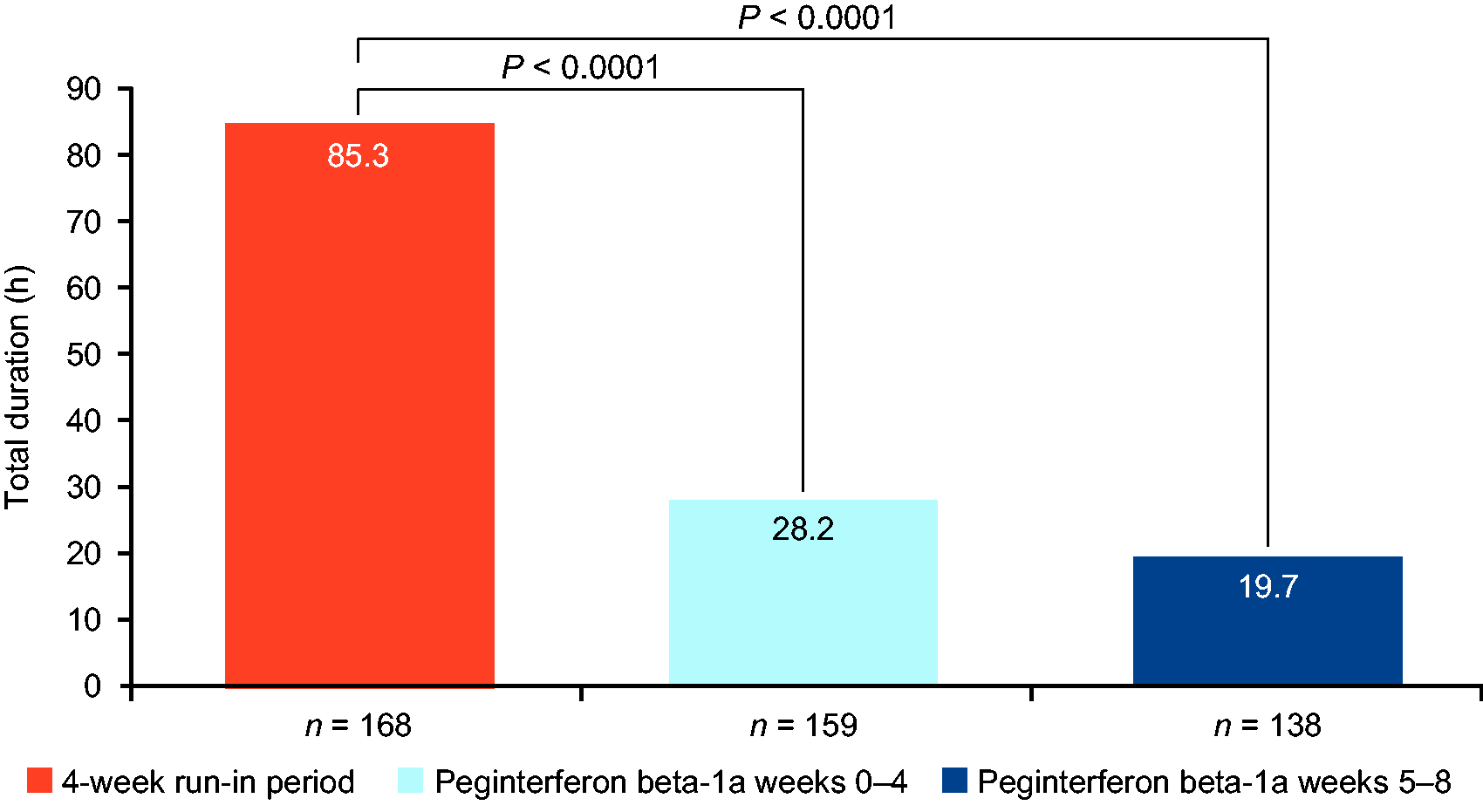
Mean cumulative duration of total flu-like symptoms (FLS) over 4 weeks on prior interferon (IFN) and following transition to peginterferon beta-1a. The duration of FLS for a treatment was defined as the sum of hours from the treatment to 48 hours with a FLS score greater than 0. If the FLS score was greater than 0 at an evaluation time, the event was assumed to have started at the previous evaluation time, and 6 hours was counted as the duration. The total duration of FLS was defined as the total duration by weeks in screening/run-in, the 0–4-week period, and the 5–8-week period. The
Most patients (91.0%) experienced one or more AEs during the course of treatment. The most commonly reported AEs were injection site erythema (39.8%), ISR (21.9%), and influenza-like illness (11.9%; Table 2). Influenza-like illness is an investigator-reported AE and is distinct from FLS reported by patients. Injection site AEs were generally mild (Supplementary Table 3). The majority of patients experienced either mild events (34.3%) or moderate events (47.3%), whereas 9.5% experienced severe events. Serious AEs occurred in 5.0% of patients overall, with 6.1% occurring in the naproxen and 3.9% in the current FLS regimen groups (Table 2). In total, AEs led to permanent study discontinuation in 13.4% of patients, with 4.0% discontinuing due to ISRs and 2.5% discontinuing due to FLS. No deaths occurred during the study.
Incidence of adverse events (AEs).

FLS: flu-like symptoms; MS: multiple sclerosis.
Patients were dosed at least once with peginterferon beta-1a; only post-dose AEs are included.
Patient-reported outcomes
The majority of patients reported good control of their walking disability through 48 weeks. PDDS scores were similar at baseline and 48 weeks (0.830 (
Discussion
The results of the ALLOW study indicated that patients who switch from a non-pegylated IFN to peginterferon beta-1a do not experience a worsening of FLS as measured by a 2 or greater point change on the FLS-S scale. Overall, 89.6% of patients did not experience new and/or worsening symptoms during the initial 8 weeks of switching to peginterferon beta-1a, and FLS severity remained low throughout the 48 weeks of the study.
This study also further characterized FLS timing and duration. Patients switching from a non-pegylated IFN to peginterferon beta-1a may be counseled that FLS most commonly begin approximately 10 hours after injection and last roughly 17 hours, approximately 3 hours longer than would be experienced with a non-pegylated IFN, though FLS onset and duration may vary widely among individuals. However, peginterferon beta-1a has the least frequent dosing schedule of all IFN medications for patients with MS, so although peginterferon beta-1a increases individual FLS event duration following each injection, the total number of FLS events per month is reduced by 50% compared with intramuscular IFN beta-1a (weekly dosing) and by 86% compared with subcutaneous IFN beta-1b (every-other-day dosing).5,7,19 Moreover, following the switch to peginterferon beta-1a, the total mean duration of FLS was 57.1 hours shorter (a 67% reduction) in weeks 0–4 and 65.5 hours shorter (a 77% reduction) after acclimation to the new therapy in weeks 5–8.
The overall safety and tolerability of peginterferon beta-1a over the 48 weeks of treatment was similar in this study to that observed in the pivotal phase 3 ADVANCE trial for patients receiving peginterferon beta-1a every 2 weeks. 10 In the current study, 91% of patients experienced an AE, similar to what was seen in ADVANCE. The most common AEs in the current study and ADVANCE were injection site erythema and influenza-like illness. Although most AEs were mild to moderate in both studies, fewer severe (9% vs 18%) and serious (5% vs 11%) AEs occurred in this study than in ADVANCE. This could reflect most of the patient population in the current study having previously received IFN treatment, whereas the ADVANCE patient cohort was mostly treatment naive.
Naproxen did not significantly change FLS outcomes compared with patients’ current FLS management regimens. This could be explained in part by the study design, which did not restrict the use of non-steroidal anti-inflammatory drugs (NSAIDs) and other analgesic agents for those patients randomized to their current FLS treatment; in fact, 24.3% of patients in the current therapy arm were on naproxen. Moreover, established regimens may have already been optimized to the individual patient. These results indicate that FLS management in patients initiating peginterferon beta-1a treatment should be tailored to the individual, but they do not exclude the possibility that NSAIDs may be an effective FLS treatment. Strategies used to mitigate FLS in patients using non-pegylated IFN include the analgesic use, dose titration, and consideration of the timing of administration so that FLS occur during sleep. Strategies used to mitigate ISRs include site massage, injection site rotation, and ice application before and/or after injection.20–22 An initial analysis of phenylephrine’s effect on ISRs in patients treated with peginterferon beta-1a demonstrated a non-significant trend towards reduction in injection site redness compared with the no-treatment control group. 23 In two Delphi analyses conducted to gain consensus on ISR and/or FLS experience and management, patient education and setting treatment expectations before treatment initiation were identified as playing a critical role in both ISR and FLS management.13,24
Over 48 weeks, study participants appeared clinically stable, with no increase in relapses upon switching treatment. Based on PDDS scores, patients did not experience a clinically significant increase in walking disability within 48 weeks after transitioning to peginterferon beta-1a.
This study supports the safety and efficacy of peginterferon beta-1a and demonstrates that peginterferon beta-1a has a consistent safety and tolerability profile over a broader age range (mean age of 49.8 in ALLOW vs 36.9 years in ADVANCE), in patients who have had MS for a longer duration (13.4 years in ALLOW vs 6.9 years in ADVANCE), and in those who are DMT-experienced, consistent with an ADVANCE subgroup analysis. 25
These data may help inform clinicians in setting expectations regarding FLS severity, duration, and management with patients treated with peginterferon beta-1a. The study provides evidence that patients administered peginterferon beta-1a generally experience FLS of similar severity and no greater frequency than patients receiving other IFN formulations. Most FLS were mild or moderate, indicating minimal impact on patients’ daily lives. Although the data show wide ranges of FLS onset and extended FLS duration per injection, which should be accounted for when considering injection timing, cumulative FLS duration over 4 weeks was significantly reduced with peginterferon beta-1a because of the less frequent dosing regimen compared with non-pegylated IFNs. With healthcare providers’ treatment guidance and an effective FLS management regimen, peginterferon beta-1a may provide relief for patients who experience FLS following injections with more frequently administered medications, resulting in improved compliance and treatment adherence.
The PDDS is provided for use by the NARCOMS Registry: www.narcoms.org/pdds. NARCOMS is supported in part by the Consortium of Multiple Sclerosis Centers (CMSC) and the CMSC Foundation.
Supplemental Material
Supplemental material for Patients transitioning from non-pegylated to pegylated interferon beta-1a have a low risk of new flu-like symptoms: ALLOW phase 3b trial results
Supplemental Material for Patients transitioning from non-pegylated to pegylated interferon beta-1a have a low risk of new flu-like symptoms: ALLOW phase 3b trial results by Robert T Naismith, Barry Hendin, Sibyl Wray, DeRen Huang, Fiorenza Gaudenzi, Qunming Dong, Bjørn Sperling, Monica Mann and Brian Werneburg in Multiple Sclerosis Journal—Experimental, Translational and Clinical
Footnotes
Acknowledgements
ALLOW investigator group
Conflict of Interests
Funding
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.