
Abstract
Introduction
Motor sport spans a diverse range of events worldwide, encompassing recreational, amateur and professional competition across a broad range of two- and four-wheeled vehicles. These automobiles range from the historic to the state-of-the-art; designed for the road, circuit, all-terrain and rally; engineered to withstand desert heat or sub-zero temperatures of the Arctic. This vast array of vehicles is united by competition and regulated by numerous governing bodies worldwide, each of whom have differing guidelines and recommendations for the assessment and management of the rider or driver diagnosed with head injury.
The spectrum of head injury in motor sport is changing, presenting new challenges to staff both trackside and in onward medical referral centres. The incidence of severe traumatic brain injury has significantly decreased over the past decades, thanks to progress made in the fields of both engineering and medicine. There appears to have been a graduated shift away from severe brain injury and towards mild traumatic brain injury (mTBI) andconcussion. This shift has contributed to reduced mortality in motor sport, yet significant morbidity remains.
The Concussion in Sport Group (CISG), a panel of experts in sports concussion first established in 2001 and led initially by representatives from ice hockey, football and the Olympic Medical Commission, define concussion as: ‘a complex pathophysiological process affecting the brain induced by biomechanical forces’. Concussion is largely a clinical diagnosis, classified by some as a subset of mTBI, which encompasses a heterogenous spectrum of disease and is usually self-limiting. However accurate, objective diagnosis of concussion remains problematic in motor sport. Additionally, there are now concerns regarding long-term negative neurobehavioural outcomes following this diagnosis in other sports.
Driver safety in motor sport is paramount, and mitigating concussion is no exception. Recent advances in protective equipment, for the competitor or their racing environment, have an important role to play in the reduction of concussion. Furthermore, when incidents do occur, it is now possible to analyse the causative forces in an effort to prevent similar injury to future participants.
Lastly, in contrast to other high-risk sports where the effects of concussion are typically limited to the individual, competitors returning to motor sport remain in control of a high-speed vehicle that poses a threat to themselves, other competitors and spectators. Unsurprisingly therefore, the return to race decision in motor sport is of vital importance and must be carefully conducted by all professionals involved.
This review seeks to outline the current medical and technical challenges of concussion in motor sport. Information is extracted largely from published sources and supplemented by the authors’ own data. The incidence and assessment of concussion in motor sport will be discussed, in addition to modifiable risk factors both within and outside the automobile environment. Lastly, promising areas for further research in the fields of medicine and engineering are outlined.
Method
A MEDLINE search strategy was developed and adapted for use in PubMed, TRIP and Cochrane. Scoping searches refined the terms and ensured that relevant studies were obtained. The initial search was complete on 18 October 2016 and was updated in January 2017. No date limits were applied and studies were limited to the English language.
Search terms related to concussion included head injury, mTBI and neurotrauma; for motor sport the terms chosen aimed to create as broad a search as possible across amateur and professional racing and throughout the classes (see Appendix 1). The initial search yielded 4575 studies which were reviewed using title and abstract. Exclusion criteria included all non-human studies. Secondary searches of bibliographies added further publications which were assessed with the criteria outlined above. A small number of additional publications were added by the authors, who had access to historic and offline papers.
A qualitative review of 127 full publications was conducted by two independent reviewers; all disputes were resolved. Only those studies influential in the field or adding new knowledge to the existing literature are discussed in this review.
Results
The problem of concussion in motor sport
With adjustment for national sports participation figures, ‘motor sport’ was attributed the highest rate of concussion (181 per 100,000 participants; 0.18%) in a nine-year retrospective study from Victoria, Australia. 1 This retrospective analysis identified 4745 hospital attendances for sports-related concussion, with motor sport as the cause in 14% (n = 674); third behind Australian football and cycling. The nature of participation was not defined. However, analysis of all types of motor racing at a single circuit in the United Kingdom found that 23 of 364 competitors were diagnosed with minor head injury over a five-year period, representing a far lower prevalence of 6.3%. 2 Additional estimates of prevalence across recreational and competitive motor sport are outlined in Table 1, in addition to calculation of an annual rate.
Overview of concussion diagnoses in motor sport from the published literature: proportion of diagnoses and annual rate of concussion.

ATVs: all-terrain vehicles; Enduro: cross-country, off-road motorcycling; NASA: National Aeronautics and Space Administration; NASCAR: National Association for Stock Car Auto Racing, MotoGP: Grand Prix motorcycle racing.
aCalculated by authors from available data.
bDefined in source as the proportion of hospital attendances attributed to concussion.
cLengthy of study not defined.
dDuration of study less than one year.
A relatively large portion of the motor sport literature explores concussion in motocross events. A retrospective study conducted at a single US trauma centre analysed injuries attributable to a nearby annual motocross competition; 51 competitors from four annual competitions attended the facility, with 16% (n = 8) diagnosed with concussion during the study period. 4 A similar analysis of emergency department attendances at a single centre in the United States found that 9.5% (n = 56) of all treated injuries were concussion in motocross and all-terrain vehicle riders. 5 In a separate study, when surveying an entire motocross racing season, it was found that 48% (n = 67) of riders experienced at least one self-reported symptom of concussion. 12 These results were translated to Emergency Department attendances in a separate study at the same institution, where it was found that between 2000 and 2007, 19% (n = 57) of all attendances were attributed to concussion. Finally, providing a national overview for the United States, an 11-year retrospective study using the National Electronic Injury Surveillance System database recorded concussion as the most common form of head and neck injury in motocross (although participant level was not defined), accounting for 29% (n = 22,788) of these injuries. 13 In summary, concussion in motocross is highlighted as one of the most common injuries sustained, with presentations ranging from 9.5% to 19% in competitive events.
Rates of concussion in professional motor sport
Disappointingly, much less data have been published for professional motor sport racing. The earliest published study of professional four-wheel racing is from Indy Racing League (IRL), where a survey of 124 drivers during four racing seasons (1981–1984) found that only 13 drivers reported previous head injury (defined as loss of consciousness (LOC), with admission for observation or treatment), a prevalence of 10.5%. Throughout the study period, IRL and Championship Auto Racing Teams (CART) had comparable rates of head injury at 16.6% and 17.6%, respectively. Of note, all competitors returned to competitive driving. 14 In contrast, figures from 12 years later (1996–2000) give an incidence of 1.2 concussions per 1000 drives. This data is from a single-centre four-year retrospective study at the Fuji Speedway which investigated all injuries presenting to the circuit medical centre, encompassing professional saloon car and single seat racing. Concussion was defined as any driver with amnesia or confusion and diagnosed in 3 out of 112 drivers (2.7%). 6 The most recent study, a retrospective analysis of all National Association for Stock Car Auto Racing (NASCAR), impact data from the 2002–2008 race seasons, found that head injury (mild concussion, with or without LOC) occurred in 27 of the 274 selected impacts (9.9%). These data are difficult to interpret, but are the only published information for this racing series. 7 In contrast, unpublished data from the British Touring Car Championship (BTCC) and its support series illustrate that the incidence of concussion may be increasing. Formal diagnoses from the Race Medical Director numbered zero to one annually in the early 1990s and are now in double figures. Data from the most recent seasons are as follows: 6 (2012), 7 (2013), 8 (2014), 11 (2015) and 6 (2016). At the time of writing, one diagnosis of concussion has already been made during pre-season testing in the British Formula 4 Championship (certified by the Fédération Internationale de l’Automobile (FIA) and powered by Ford).
A small body of literature relates specifically to professional two-wheel competition, extracted from exhaustive MotoGP data. A study of three US MotoGP races in 2013 (including practice sessions, qualifying and race) recorded 78 crashes, with an incidence rate of 9.7 crashes per 100 rider hours. Ten riders attended the medical facility, with two diagnosed with concussion, resulting in a disproportionately high proportion of concussion diagnoses (20%). 9 A far smaller proportion of concussion diagnoses was collected from the internal database of the ‘Clinica Mobile’ medical team during the 2014 season, encompassing MotoGP, Moto2 and Moto3. Injury was defined as the ‘inability to race or train’, and of the 191 recorded, 1.6% (n = 3) were concussion. 10
Concussion in the adolescent
Regardless of amateur or professional racing status, there are a growing number of adolescent participants in motor sport. Analysis by this sub-type is largely under-represented in the literature; however, a single study provides data for adolescent motocross riders during the 2000–2007 seasons. A total of 299 injuries were recorded in 249 patients, of which head trauma with LOC was reported in 18% of cases. There was an average of 1.37 concussive episodes during the study period (range one to five), and 33% of riders reported repetitive head injuries during the seven-year study period. 3
Assessment and identification
Key clinical features of concussion include confusion and memory loss of varying degrees and duration. Historically, definitions have also included LOC; however, this is no longer a diagnostic criterion. Indeed, recently published literature highlights that LOC occurs in less than 10% of sports-related concussion. The lack of clear clinical diagnostic criteria and objective diagnostic tools results in real challenges for those providing medical cover for motor sport events.
Diagnosing concussion in motor sport
The poor specificity of concussive symptoms was highlighted in the published literature by Luo et al., 11 who found that a large proportion of competitors continued to display symptoms of concussion throughout the racing season. 12 Similarly, Colburn and Meyer concluded that concussion figures were likely to be under-documented, despite representing the most common non-orthopaedic injury identified in their cross-sectional study. 11 The same study also examined self-reporting of concussion in motor sport, one of only two publications to do so. A questionnaire was utilised to report on the types of injuries sustained during four international six-day Enduro events. Of the 172 drivers, 121 were injured during the study period and only 7% (n = 9) reported concussion. Self-reporting was further analysed by a mixed methods questionnaire study of 40 American professional stock car racers who reported on the diagnosis of concussion throughout their careers. 8 A quarter of drivers (n = 10) admitted to concussion during their racing lifetime. Concussion and head injury were the second most common injury-related fear amongst the surveyed participants.
Diagnosis trackside
Only one motor sport governing body publicly mandates the diagnostic tool utilised for concussion trackside. The Federation Internationale de Motocyclisme (FIM) states that: ‘in the event of a suspected concussion, the rider should be assessed using a recognised assessment tool such as SCAT3 (Sports Concussion Assessment Tool) or similar’. 15 Of note, SCAT3 includes a neck examination and additional symptoms which are not included in the previous version, SCAT2. Internal guidelines for Indy Car advise the use of SCAT3 at on-site medical facilities. Colloquial sources also suggest that the King-Devick is utilised, but this is not corroborated in published literature or available guidelines.
Computerised neurocognitive tests
There has been a wave of computerised neurocognitive tests (CNTs) in the past decade, which aim to objectify the diagnosis of concussion. More recently, these platforms have become internet-based, and all have standardised and often automated scoring systems. These ready-prepared tools are employed across a huge range of sports internationally and implemented by a variety of medical personnel.
The Immediate Post Concussion Assessment and Cognitive Testing tool (ImPACT) was created in the 1990s and employed by many professional American sports associations, including the National Football League, National Hockey League and Major League Baseball since its inception. This CNT is performed in 45 min and produces four composite scores: verbal memory, visual memory, visual-motor processing speed and reaction time.
A formal review of ImPACT in sport highlights that the validity and utility of this CNT is strongly affected by environmental, administrator and participant factors. 16 Extrinsic factors include the suitability of the testing environment and the clarity and reproducibility of administrator instructions. Participant factors included physical exertion and hours of sleep prior to testing. The same review highlights that 10%–35% of athletes could intentionally under-perform in their baseline assessment, thus invalidating their post-injury measures. In a separate publication, the authors stated that these threats to validity could be addressed by rigorous standards of clinical practice. 17 Further exploration of measurement error for ImPACT in the systematic reviewfound that 22%–46% of participants experienced a change that exceeded the measurement error in at least one ImPACT composite score; representing an unreliable change. 16 This reviewquestioned the diagnostic accuracy of ImPACT, owing to the poor to moderate reliability of most scores. Indeed, it was specifically stated that: ‘it is hard to establish the diagnosis of concussion on the basis of ImPACT testing alone’. 16
To date, there have been no publications which specifically analyse the use of ImPACT in motor sport, yet ImPACT has been utilised without specific validation in this field since the early 2000s, in the absence of an alternative CNT. ImPACT was first mandated by CART in 2002, later by NASCAR in 2014 and currently mandated by FIA for Formula 1 and other selected international series. Use of ImPACT is also advised by the FIM, AMA ProRacing and the CNT of choice for Indy Car.
Protective measures to minimise concussion in motor sport
Competitor protective equipment: helmets, HANS and headrests
The theoretical utility of helmets in preventing concussion is stated as two-fold in a review by Barth et al. 18 ; firstly, ‘the cushioning effect of helmets increases the distance of deceleration and reduces the forces associated’ and, secondly, on a more basic physical level, the use of helmets increases the surface area across which the blow or force is absorbed. Regardless, it is acknowledged that changes in driver velocity greatly influence clinical outcome. In contrast, a more in-depth review by Lloyd and Conidi collates data from biomechanists and sports neurologists, concluding that helmets do not produce significant protection against concussion, although severe brain injury (such as subdural haematoma) was the main exploratory aim. 19 Finally, a single study was identified which specifically commented upon helmet use and concussive symptoms in motor sport. Prospective analysis of motocross riders at a regional racetrack during the 2010 season found that professional helmet fitting was associated with a 41% decrease in the development of concussive symptoms. The use of neck braces was found not to correlate significantly with a reduction. 3
The Head and Neck Support device (HANS) was first introduced by CART in 2002 and mandated by the FIA in 2003. The HANS was designed with the aim to reduce fatal cranio-vertebral dissociation injuries by transferring the weight of the helmet and head impact loads to the shoulder belts. HANS prototypes were tested using track, sled and direct impact tests in an initial biomechanical feasibility study, which also implied a theoretical reduction in head injury. 20 This ideology is supported by data from a single study of the CART racing series, published in 2002. 21
In direct response to a dramatic rise in severe head injuries in the IRL during the 1997 season (n = 7), the race medical team personnel collaborated with engineering colleagues to alter the composition and location of the in-car padding. This change not only reduced severe head injuries but also minimised the incidence of concussion. This positive affect persisted throughout the 1998 and 1999 seasons. 22 Other attempts at modifying in-car protective measures in order to minimise concussion have included safety harnesses 23 and airbags; the former successful and the latter not. 24
Altering the competitive environment
There is a large amount of literature which investigates the magnitude of a single impact sufficient to cause brain injury; however, few studies specifically comment upon concussion. Furthermore, the varied nature of motor sport incidents (their speed, direction and magnitude) provides a unique platform for analysis of the causative forces implicated in concussion.
The relationship between vehicle gravitational (
Returning to race: Current guidelines in motor sport
A recent survey published in the FIA medical journal,
Road driving after concussion
For those road drivers with severe concussion, it has been shown that both task and driving performance are reduced after injury. 30 Furthermore, objective studies have also shown that traffic hazard perception is impaired in the short-term following concussion; 31 however, this is not replicated in the long-term after self-reported diagnoses. 32 A small quasi-experimental case–control study examining road driving has also shown that patients with mTBI should not drive for 24 hours; however, the optimum period for abstinence was not explored. 33
Recommendations for other sports
The most influential guidelines for the management of concussion in sport are produced by the CISG, who first met in Vienna in 2001, where a consensus definition for sports-related concussion was produced. Minor revisions were made in Prague in 2004 and Zurich in 2008. During the most recently published meeting of the CISG (Zurich, 2012), concussion was formally defined as: ‘a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces’. 34 Five major features were defined relating to the causative event, resultant symptomatology and absence of radiological changes. Additionally, same-day return to play was eliminated for any athlete for which there is a suspicion of concussion. Outside of these guidelines, the general clinical consensus is that athletes should be asymptomatic and cognitively unimpaired before a return to play (or race). For contact sports, the recovery time from sports-related concussion is estimated as 5–10 days after injury.
Formal motor sport guidance
The ongoing desire for formal guidance regarding concussion in motor sport has recently been characterised by an online survey published in
The FIM publish a comprehensive Medical Code, which advises that: ‘Assessment of the injured rider and return to competition should be in accordance with the guidelines for the assessment and management of concussion as contained within the International Consensus Statement on Concussion in Sport Zurich 2012’. 15 In a direct statement of concordance to the above, the guidelines also state that: ‘the rider should immediately be excluded from competition for at least the rest of the event’ if a concussion is diagnosed. Return to race is then dictated by documented formal assessment of resumption of: ‘normal neuro-psychological function’, where the use of ImPACT or functional MRI is advised. AMA ProRacing similarly advises ‘passing’ of an ImPACT assessment prior to returning to competition, 35 a stance which is replicated by Indy Car.
The UK Motor Sports Association (MSA) introduced its first concussion guidelines into the MSA Yearbook in early 2016 (Table 2), advising removal from competition for 14–21 days after a diagnosis of concussion. 36 Similarly, Speedway New Zealand mandates a 22-day stand down period for any driver diagnosed with concussion, which can be reduced to an absolute minimum of 15 days, pending formal medical assessment and Board approval. 37 There are no formal published guidelines from NASCAR or the FIA. Regarding the latter, concussion seems only to be loosely covered by Article 1.5.3 of Appendix L to the International Sporting Code: ‘any health problem that might, because of its nature or the treatment required, result in consequences that are harmful to participation in motor sport including in case of an accident’. 38
The first MSA concussion guidelines, published in the annual update of the Yearbook, on 1 March 2016. 36
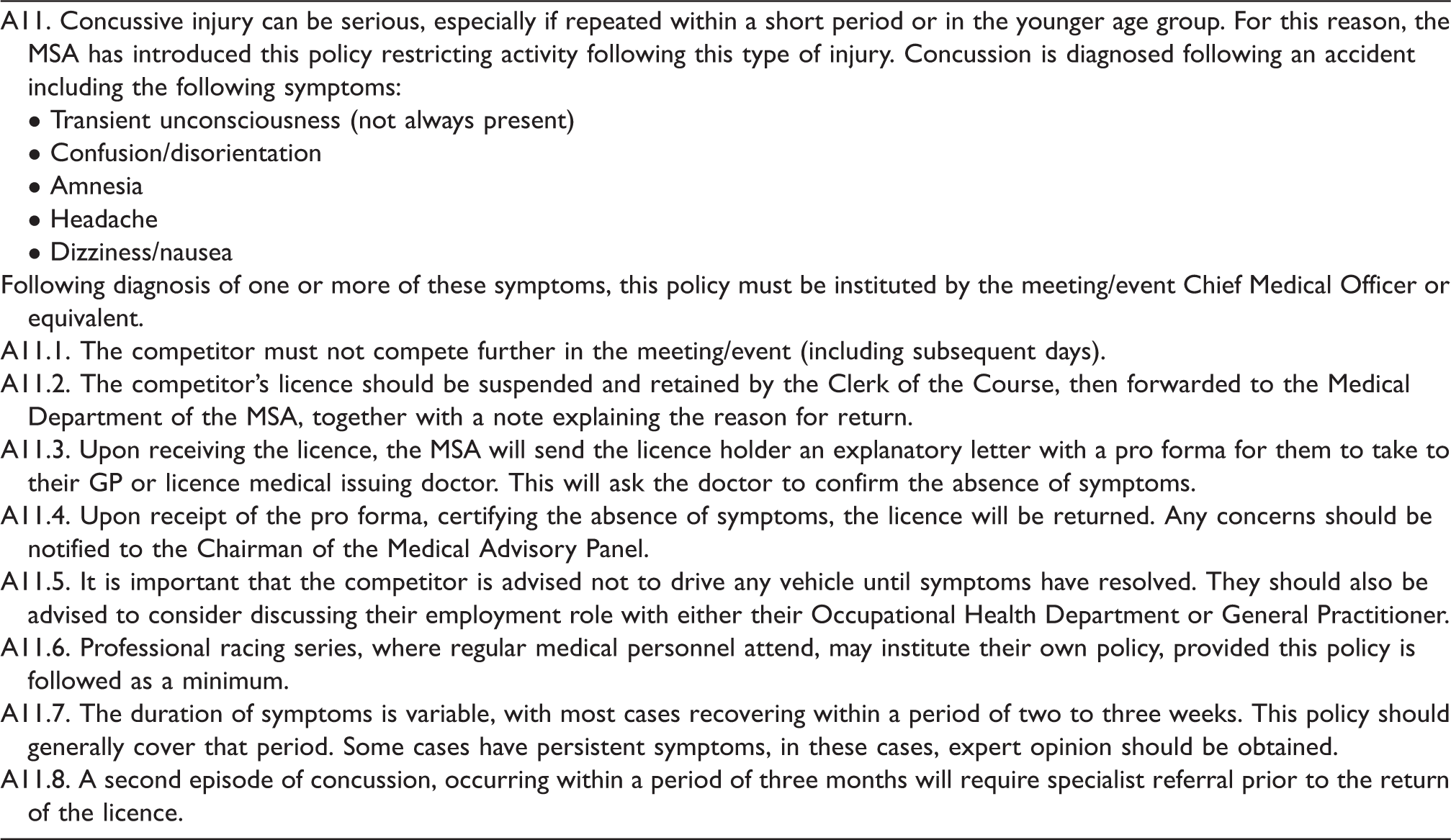
Source: MSA Yearbook 2016, reproduced with permission from the MSA, 28 February 2017.
MSA: Motor Sports Association.
Areas for research and development
The medical management of concussion
Frontiers in the medical management of concussion in motor sport are broadly two-fold. The first is clinical and relates to the trackside diagnosis of concussion and the return to race decision; the second involves collaboration with engineering colleagues and relates the mitigation of translated forces during impacts.
As elucidated in a systematic review of the ImPACT assessment, new directions for objective assessment in concussion include balance testing (such as the sensory organisation test), ocular-motor assessment (visual ocular motor screening) and cognitive-balance dual tasks paradigms.
16
These tools must be utilised carefully however with stringent normative values, since research has proven that motor sport athletes attain superior visual performance when compared to controls.
39
Furthermore, accurate diagnosis of concussion requires competitor engagement and education; a recent survey described previously from
The notion of incident analysis informing technological advances in motor sport was proposed by Olvey et al. 40 as early as 2004 and has recently been translated to the use of simulated driving studies. 41 The latter is supported by evidence from 2006, which concludes that simulated driving is comparable to road use but lacking the emotional component. 42
Engineering a reduction in concussion
Driver safety has become a cornerstone of motor sport regulation, embraced by engineers and medical professionals alike. However, the requirement for championship-winning vehicles with potentially higher longitudinal and lateral accelerations has to be carefully mitigated by driver protection systems, which in themselves can add extra mass, cost and other unforeseen effects. The relationship between medical and engineering professionals was concisely summarised by Lippi et al. 43 Andy Mellor, Senior Research Engineer at the Global Institute for Motor Sport Safety provides insight into these technical challenges.
Head protection in motor sport is of vital importance and can be lifesaving. A serious incident will not only impart considerable accelerations to the vehicle chassis and directly to the competitor but also cause significant relative velocities between the head and the in-car environment. A head protection system must therefore be designed to manage these forces. The primary aim of this equipment is to absorb significant amounts of energy, whilst ensuring that the loads, pressures and accelerations imparted to the head do not exceed injury thresholds. From an engineering perspective, the greatest challenge in motor sport lies in mitigating the relatively high change in velocity together with the very short stopping distance available on track. Currently, helmets used in motor sport are typically homologated to absorb energy at acceleration levels of up to 300
An important future contribution to the technical aspect of motor sport will come from the analysis of racing incidents. The preferred data capture method in professional motor sport currently is the deployment of in-ear accelerometer systems which are used in Formula 1 and Indy Car. The Formula 1 system can measure 0 to ±400
Conclusion
The most influential medical professional in the field of motor sport was undoubtedly the late Neurosurgeon Professor Sid Watkins, former President of the FIA Institute for Motor Sport Safety. In addition to revolutionising driver safety in motor sport, Professor Watkins assessed all injured competitors in FIA Formula 1 and the BTCC during his extended career. This singular approach to concussion is now not possible in motor sport as a result of ever-increasing race team pressures and fierce commercial interests, on a background of more prolific litigation and high-profile medico-legal rulings in other sports. In fact, there now exists a significant knowledge gap for concussion in motor sport specifically.
Extensive review of the published literature has established that motor sport has a relatively high rate of concussion when compared to other sports, but the data are variable depending on the vehicle, class/championship, country, level of competition and terrain. Furthermore, it is difficult to interpret these data since a significant proportion of the published literature is descriptive or observational. In addition, the most informative studies are retrospective and frequently rely upon emergency department attendance figures or nationally collected data, which are not specific to motor sport. Therefore, it is possible that the data presented may misrepresent the actual incidence or prevalence of concussion in motor sport. This latter idea is supported by the recent finding that the majority of competitors have historically failed to seek medical advice following a concussive episode.
In contrast, the published data for professional motor sport appear to indicate lower rates of concussion. However, there are few studies which investigate this sector of motor sport specifically, and the diagnostic criteria are disparate, largely attributable to variation in publication date. Superficial analysis of the small amount of published data indicates that American series, such as Indy and NASCAR, have lower rates of concussion than in competitive activities utilising similar vehicles in other countries. In particular, rates of concussion in the BTCC and its support series appear to be increasing; a fact which requires further investigation. Lastly, there is a growing representation of adolescents in professional motor sport, however this group remain under-represented in the published literature. Studies investigating non-professional competitive motor sport indicate that repetitive head injuries are problematic; a significant cause for concern in the developing brain of a professional motor sport athlete. However, regardless of professional or amateur racing status, there are a growing number of adolescent participants in motor sport globally, and medical professionals must recognise the significant contribution of this cohort to concussion, especially when cognisant of the second impact syndrome.
Review of the medical literature exploring the protective measures employed to reduce head injury/concussion highlight that partnerships with engineering colleagues have been employed successfully in recent years to reduce rates of concussion. This collaborative approach may be an efficient way in which the competitive nature of the sport can be maintained in the safest manner. Furthermore, it will be vital to extend such collaboration to incident analysis where a knowledge gap exists for the threshold values for concussion. The field of motor sport, with its close links to frontiers in technology, is a fertile ground for multi-disciplinary collaboration, and this provides an excellent opportunity to elucidate the non/-impact-related causative factors of concussion and the relative contribution of linear versus rotational forces.
Perhaps the most influential decision made by a medical professional is that of a competitor returning to race after a concussive episode. Currently, competitors appear to be relatively poorly informed regarding the diagnostic criteria for concussion, with the ideology that LOC is a necessary component being perpetuated even in professional series. Additionally, there is no established ‘safe period’ in the literature for return to driving in general, not least for competitive activity. The 2016 Berlin update of the CISG guidelines are eagerly awaited by the medical community. Their adaptation and incorporation into readily accessible formal motor sport-specific concussion guidance is a necessity.
The current challenges in the medical management of concussion in motor sport could be mitigated by prospective, large scale, international studies of high scientific standards designed to accurately define the exact incidence and prevalence of concussion in motor sport, which remain unclear. The need for motor sport-specific studies also extends to the assessment and diagnosis of concussion; ImPACT remains the only CNT commonly utilised in the field, yet has never been formally validated for motor sport. Finally, return to race decisions could be augmented by simulated driving scenarios supplemented by eye-tracking technology and measurement of reaction times. Such studies would allow competitors to be more aggressive in their driving style, without compromising their safety, or that of other competitors, and indeed a similar approach could be utilised for specialised onward rehabilitation. The applicability of new objective diagnostic tools for concussion to highly specialised motor sport athletes could also prove invaluable.
From an engineering perspective, the current technical challenges of concussion in motor sport centre around the need to balance driver safety against race team success. Despite this difficult task, there remains a significant potential to greatly improve knowledge of the physical mechanisms and thresholds for concussion by investigating and analysing motor sport incidents. The deployment of in-ear accelerometers to a broader range of championships would provide a much-needed increase in the amount of data available worldwide. The use of additional technology, such as micro rate-sensors and high-speed video, may prove valuable tools to support this analysis. These tools are limited currently only by team, championship or regulatory body engagement. Caution must continue to be employed in the interpretation of these data, however, since helmet motion may not translate to that of the head, the brain or its microarchitecture. Even with such caveats, the data from these tools may be combined to develop improved performance targets for future head protection systems, applicable not only to motor sport but also to road users.
Despite the popularity of motor sport in the lay domain and the vast amount of financial investment in the engineering aspect of the sport, there remains a mismatch of resources to medicine and a resultant paucity of medical research in the field. Concussion is an evolving problem which appears to be more prolific in some series as compared to others, yet the causative forces remain largely undefined. There exists a real progress in the global assessment and diagnosis of concussion and the prospect of new objective diagnostic tools could revolutionise the field. However, the challenge for motor sport will lie in incorporating these advances into guidelines applicable to the vast array of national and international motor sport governing bodies, across a range of amateur and professional competition.