
Abstract
Introduction
In the field of public health, lifestyle has been highlighted as an essential factor for maintaining and improving health for people of all age groups (Bryndin & Bryndina, 2017). Unhealthy lifestyle behaviors, regardless of demographic factors such as age and gender, contribute to the rising incidence of non-communicable diseases (World Health Organization, 2017; Kibria et al., 2019). Such lifestyles have increasingly been recognized as key determinants of individual health and quality of life (Nari et al., 2021). The lifestyle choices made in adulthood are pivotal in determining health and quality of life in old age, underscoring the importance of understanding adult lifestyles for effective health promotion (World Health Organization, 2022a, 2022b).
The concept and definition of lifestyle remain diverse and are interpreted variably across disciplines. From a psychological perspective, lifestyle encompasses an individual’s personality, values, and beliefs (Adler & Porter, 1931; Diener & Biswas-Diener, 2011), whereas from a sociological perspective, it is shaped by social status, class, and cultural capital (Lazer, 1963; Weber, 1978). Recent studies in the field of public health propose that lifestyle is formed by habitual activities based on personal needs and values, influenced by the given environmental context (J. H. Park et al., 2023).
Key lifestyle factors that determine health include physical activity, dietary habits, alcohol consumption, smoking, and social relationships, as well as engagement in work (J. H. Park et al., 2023; Wu, 2021). These factors are subject to change depending on individual identity, value systems, and the choices made in response to opportunities provided by society, community groups, and cultural contexts (Cockerham, 2017; World Health Organization, 2021). Given the ability to address health issues through lifestyle, it is essential to have an in-depth understanding of the context in which different behaviors and habits are chosen (Balwan & Kour, 2021).
To comprehensively understand the multidimensional aspects of lifestyle within the public health domain, standardized assessment tools have been developed and utilized. These include the Health-Promoting Lifestyle Profile II (Walker et al., 1995), Yonsei Lifestyle Profile (K. H. Park & Park, 2020), and the International Physical Activity Questionnaire (IPAQ; Craig et al., 2003). Such tools quantitatively measure the frequency, intensity, and exposure to risk factors associated with lifestyle behaviors that affect health (Lim & Park, 2022). Although these tools allow for an understanding of characteristic behavioral patterns, they are limited in their ability to capture the personality traits that influence behavior, cognitive processes, and properties (W. T. Anderson & Golden, 1984; Garcia et al., 2015; Piksa et al., 2022).
Existing studies have rarely attempted an exploratory analysis of the subjectivity behind decisions regarding personal health lifestyles, which are shaped by core values rather than just individualized behavioral patterns. Therefore, this study is necessary due to the lack of research exploring and understanding healthy lifestyles formed by daily activities and habits based on personal core values. In the absence of foundational academic information, an exploratory study aimed at identifying individual subjectivity and the perception structure of healthy lifestyle activities and patterns is considered appropriate (Rubin & Babbie, 2016). Q-methodology, which objectively analyzes subjective views and attitudes, is well-suited for exploring the perspectives and opinions that shape individual lifestyles (Stephenson, 1935). Such exploratory research is expected to contribute academically to promoting health and improving the quality of life by understanding the subjective perspectives on healthy lifestyles among individuals from diverse sociocultural contexts.
Therefore, to explore the subjective differences and diverse lifestyles formed by daily activities and patterns, Q-methodology was applied to explore the perspective of their subjectivity and to examine the characteristics of lifestyles types.
Methods
Study Design
This was an exploratory study that applied the Q-methodology of a mixed method research design to analyze the perception structure and types of subjective opinions and attitudes toward healthy lifestyles in adults.
Q-Methodology
Q-methodology can analyze the different subjectivities of humans (Stephenson, 1935). This methodology combines quantitative and qualitative approaches and can scientifically analyze subjectivity, reflecting individual opinions, attitudes, and values, by focusing on intraindividual significance rather than interindividual differences (Kim, 2008). The R-method, a quantitative research methodology, identifies population characteristics and analyzes differences through correlation analysis between variables, while the Q-method examines differences in the meanings of human subjectivity related to specific phenomena (Watts & Stenner, 2012). Therefore, Q-method is the most effective approach to grasp the perception structure and type characteristics of subjectivity among the healthy lifestyles of adults, reflecting different personal values and attitudes.
Steps in Q-Methodology
In this study, data collection (Q-sample, P-sample) was done from adults aged 19 or older living in the community. All participants in the study included those who voluntarily consented after understanding the purpose of the study, scope of collection, and privacy guidelines. This research has been reviewed and approved by the Institutional Review Board of University (Approval No .1041849-202201-SB-011-01, 1041849-202205-SB-091-01).
Q-Sample (Development of the Statement)
Q-sampling is a process of collecting subjective subjectivities about adults healthy lifestyles in the form of statements. For this study, data were collected online from approximately 1.6 million panelists registered with Macroville Embrain using non-probability sampling. Panelists voluntarily responded to open-ended questions about “healthy lifestyles that are important in daily life” between March 30 and April 4, 2022. Before participation, an online information sheet outlined the study’s purpose, procedures, data protection, anonymity, and the right to withdraw. Informed consent was obtained via an online agreement checkbox. All data were anonymized by Macroville Embrain prior to being provided to the researcher, ensuring that no identifiable or sensitive information was accessible. Panelists were compensated through Macroville Embrain’s point system; no additional incentives were provided by the researcher (Approval No. 1041849-202201-SB-011-01).
Among the 237 statements expressed, sentences with duplicate meanings and insincere answers were excluded and the expression method was reviewed and modified into sentences with appropriate content. The statements were classified based on lifestyle factors such as physical activity, eating habits, activity participation, social activity, and mental health (Sowa et al., 2016). Thereafter, 48 statements were selected through consensus among the experiences in lifestyle research for the statements that were representative and meaningful. The final number of Q-samples was found to satisfy 40 to 80 suitable statements in the Q-methodology study (Watts & Stenner, 2012).
For the preliminary survey, three adults were selected as a purposive sample, and the reliability was confirmed by setting the time difference between the sort and re-sort processes at 5-day intervals. Consequently, the reliability of the Q-sample was found to have a correlation coefficient of
Reliability of the Q-sample.

P-Sample (Recruitment of Participants)
In the Q-methodology, P-sample follows the small-sample doctrine because it is sufficient to objectify the subjectivity of the research topic, unlike the R-method, which aims to generalize through the collection of many samples (Brown, 1993). The selection criteria for P-sample included non-disabled adults (aged over 19 years), those who could read and understand the text, and those who agreed to participate. A total of 34 P-samples were recruited, which satisfied the appropriate number of P-samples from 30 to 50 people in the Q-methodology (Brown, 1996).
P-sample was conducted through snowball sampling targeting adults living in the community. Data were collected from July 1 to September 29, 2022, using FLASHQ Offline v.1.0, which supports remote data collection in Q methodology research. The software was distributed and returned via email and included an information page detailing the study’s purpose, procedures, data protection, and the right to withdraw. Participants provided informed consent by checking an agreement box before proceeding. The task was completed individually on participants’ personal computers, allowing them to participate at their convenience and withdraw at any time. Data were anonymized, and no identifiable information was collected. No additional incentives were offered, and the task took approximately 15 to 20 min to complete (Approval No. 1041849-202205-SB-091-01).
The age range of the P-sample was 21 to 61 years, with an average age of 39.88 years. The proportion of women was higher than that of men and most participants had university education. Furthermore, 82.3% had paid jobs, and 67.3% managed their living expenses through earned income (Table 2).
Descriptive Statistics of the P-Sample (

Q-Sort (Data Collection)
Q-sort is a process in which participants of the P-sample classify the statements of the Q-sample according to their subjective opinions and viewpoints. The Q-distribution charts were set on an 11-point Likert-type scale (+5 to −5) in the form of a normal distribution, and forced distribution, which forcibly sorted Q-samples as much as a given number, was applied (Brown, 1980).
In Q-sort, after the P-sample participants read and understood the statement of the Q-sample, each statement was classified into three categories: agreed, neutral, and disagreed. Then, it was classified as both extremes of agreed (+5 points) and disagreed (−5 points) of the distribution chart, followed by a sequential classification as neutral (0 points; Figure 1).

An example of a Q-sort for the data collection (FLASHQ offline).
Data Processing and Analysis Methods
The Q-sort data sorted from the P sample were analyzed using the PQMethod (ver. 2.35) program. Q-factor analysis was performed using a principal component analysis (PCA). Factor extraction was conducted based on the following criteria: a factor with an eigenvalue of 1.0 or higher (Guttman, 1954; Kaiser, 1970, that satisfies the significance level of factor loading (0.01), and loaded with two or more significant samples (=2.58 × [1/√
The varimax rotation method was applied to increase the variance difference and the explanatory power of the major factors (Brown, 1980). Recognition type characteristics were analyzed based on significant factor loadings and
Results
Formation of Perception Factors for Lifestyle
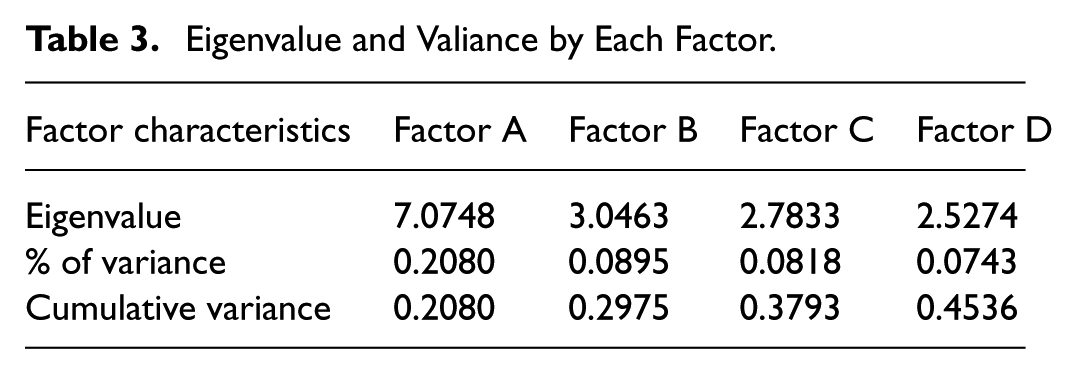
Four factors suitable for the extraction criteria were selected after analyzing the subjectivity of 34 people on healthy lifestyle. The four selected factors were included in the final factor as they were judged to be suitable for interpreting the meaning of the subject of this study. The cumulative variance of the final four factors had an explanatory power of 45.36%. In Q-methodology, if the level of explanatory power is 35% to 40%, it is judged to be at an appropriate level (Kline, 1994; Table 3).
Eigenvalue and Valiance by Each Factor.
Factor A (variance = 20.80%,
Interpreting Healthy Lifestyle Factors
The subjective perception type of lifestyle was interpreted with name, focusing on three statements, top and bottom, and based on the
Top and Bottom Statements of Each Type and

Factor A; Interpersonal and Emotional Well-Being
Factor A showed a clear perspective on forming and maintaining positive interpersonal relationships by focusing on relationships with others in their daily lives (Q-Statement 31,
Therefore, Factor A emphasizes social exchanges with people in social networks, values relationships, and aims to stabilize emotions.
Factor B; Happiness and Daily Management
Factor B focused on leisure and hobbies and pursued happiness in daily life (Q-Statement 33,
Therefore, Factor B focuses on the enjoyment and mental and life satisfaction gained from leisure and hobbies in daily life and prefers nutritional supplements and walking activities for incidental health effects.
Factor C; Emotional Well-Being and Cultivation
Factor C was found to value religious activities and pursue spiritual well-being (Q-Statement 35;
Therefore, Factor C was found to prefer spiritual and emotional well-being through religious activities and prefer interaction through social gatherings that fit with others.
Factor D; Regular Life Practice
Factor D pursued regularity in daily life (Q-Statement 37,
Therefore, factor D emphasizes the regularity of daily life along with eating habits and physical activity, whereas risk factor management is not preferred.
Discussion
Human lifestyles are shaped by behaviors and habits that reflect individual values and subjectivity, which in turn influence health. An exploratory approach is needed to understand how these lifestyles are formed and reflected in daily life. Therefore, this study aimed to explore the types of perceptions of healthy adults by focusing on individual subjectivity in various behaviors and patterns of lifestyle with a core value on health care.
Factor A emphasizes interpersonal relationships formed through social networks and the pursuit of emotional stability. Relationships, stress, and emotions in this factor are known to affect mental health (Cain et al., 2012; Martínez et al., 2019). Neuroscience research has shown that social connections are closely linked to mental and brain health (Krueger & Meyer-Lindenberg, 2019). Improving the mental health of individuals in this group can be achieved through interventions like social support (Lindfors et al., 2014), physical activity (Tamminen et al., 2020), and leisure activities with mediating effects (Belo et al., 2020).
Factor B emphasized the pursuit of happiness and a meaningful daily life, with basic health maintenance through nutritional supplements and physical activities. Happiness positively impacts a healthy lifestyle and helps prevent illness (Bagheri & Gharehbaghi, 2019). Generally, people who seek pleasure are proactive in their healthcare and engage in activities and social networks to improve their health (Veenhoven, 2008). While happiness can be associated with behaviors like smoking and drinking, this study highlights the importance of healthier hobbies and leisure activities that mediate the relationship between happiness and health (Steptoe, 2019).
Factor C emphasizes religious activities, focusing on emotional well-being and personal growth through social interactions. These interactions among individuals with shared beliefs enhance social participation, internal satisfaction, and collective identity. From a spiritual healing perspective, they positively affect feelings of defensiveness, hopelessness, and happiness, contributing to mental health (Schroder, 2003). However, conflicting findings exist (Bakhtiari et al., 2019), indicating that misguided values in some religious communities can lead to unhealthy lifestyles (Anshel, 2010). Religion, therefore, can be both a motivator for healthy living and a potential source of unhealthy habits (Anshel, 2003). This study suggests the need for further exploration into the dual impact of religious activities on health and quality of life.
Factor D focused on actively practicing health management through regular life patterns, physical activity, and eating habits, highlighting these as modifiable behaviors (Sakaniwa et al., 2022). These practices are effective in managing chronic diseases and obesity-related conditions (E. Anderson & Durstine, 2019; Barbaresko et al., 2018; Lambrinou et al., 2019). However, continuous lifestyle improvement is needed, as individual values and subjectivity influence the importance of healthy behaviors (World Health Organization, 2022a, 2022b). Transforming unhealthy habits requires professional knowledge and expert guidance (Riekert et al., 2013). Thus, professional support is essential for promoting and maintaining effective health management practices.
The recognition types of healthy lifestyles identified in this study appear to be influenced by the contexts to which the participants were exposed. Lifestyles that emphasize health have been shaped by the expansion of regulations related to public health guidelines and community initiatives, which focus on physical activity, emotional well-being, and dietary habits (WHO, 2022). Public health programs that highlight lifestyle factors in various national and regional contexts likely contributed to the relative importance or prioritization of these factors among individuals. Additionally, subjective preferences toward daily health management may have been shaped by health promotion programs offered through educational curricula and workplaces, influencing participants’ attitudes. This suggests that aligning personal values and subjective priorities with public health and health promotion strategies is a critical aspect of successfully fostering healthy lifestyles (Steptoe, 2019; Veenhoven, 2008).
This study focused on understanding lifestyle subjectivity in the context of individual situations, rather than from a medical perspective. This approach helps to interpret diverse lifestyle behaviors, beyond merely verifying their health impacts. In today’s context, where health programs and policies are increasingly important (Williams & Fullagar, 2019), the findings can inform personalized health strategies and public health policy development. By categorizing health lifestyles based on subjectivity, we gain deeper insights into individual and group behaviors, which can guide the creation of tailored health policies. Approaches based on subjective perceptions consider both psychological and social factors, enabling the development of comprehensive health promotion strategies. This method respects individual differences while enhancing the effectiveness of public health interventions and driving meaningful change.
However, the purpose and methodology of this study are limited in generalization because they focus on exploratory research. The P-sample included only 34 healthy adults, a relatively small group. To improve generalizability, future research should include individuals with disabilities, chronic illnesses, and the elderly, reflecting the multidimensional aspects of human health. It should also consider social, cultural, and environmental factors affecting health (Furman et al., 2019; Ladak et al., 2020). Expanding the sample will provide a deeper understanding of diverse health behaviors and needs, forming a stronger foundation for developing effective, broadly applicable health interventions and policies.
Conclusion
This study aimed to understand the characteristics of reflecting individual values and subjectivity using Q-methodology for health-related lifestyles. Healthy lifestyle perceptions were categorized into interpersonal and emotional well-being, happiness and daily management, emotional well-being and cultivation, and regular life practices. These findings offer valuable insights into the prioritization of different healthy lifestyles, which can guide the development of targeted programs and policies aimed at improving health and quality of life. The results provide subjective perspectives, reflecting diverse individual contexts and expanding the scope of services. This study highlights the need for expert approaches to understanding individual characteristics and fostering behavioral change. However, due to the study’s sample size and characteristics, future research should include a more diverse population in terms of health, cultural, social, and environmental factors to validate these findings. Such research would offer a broader perspective and contribute to resolving public health issues by guiding policy and program development.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251376752 – Supplemental material for Subjective Factors of Healthy Lifestyle: Q-Methodology
Supplemental material, sj-docx-1-sgo-10.1177_21582440251376752 for Subjective Factors of Healthy Lifestyle: Q-Methodology by Young-Myoung Lim and Ji-Hyuk Park in SAGE Open
Footnotes
ORCID iDs
Funding
Declaration of Conflicting Interests
Data Availability Statement
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.