
Abstract
Keywords
Introduction
High tibial osteotomy (HTO) is an effective surgical procedure for medial component osteoarthritis (OA) or osteonecrosis of the knee. 1 –12 Opening wedge HTO (OWHTO) avoids most issues associated with lateral closing wedge osteotomy (CLWO) such as the need to perform fibula osteotomy, the risk of compartment syndrome, and the risk of injury to the common peroneal nerve. 5,13
Obtaining correct postoperative lower limb alignment is an important factor in achieving a successful clinical outcome after HTO. 5,10,14 However, undercorrected or overcorrected knees have been reported after OWHTO. 5,10,15 Undercorrection can cause recurrence of the varus deformity with subsequent development of medial arthritis, while overcorrection can cause cosmetic problems and later development of lateral arthritis. 5,15 OWHTO was mainly performed for patients with a femorotibial angle (FTA) of <185° in past reports. 10,13 Fixation devices and navigation systems have been developed to obtain long-term satisfactory clinical outcomes after OWHTO. 5,11,16,17
We have performed OWHTO for patients with a preoperative FTA of ≥185° and advanced medial component OA who were reluctant to undergo total knee arthroplasty (TKA). The limitation of the correction angle (CA) on OWHTO and the reasons for undercorrected or overcorrected knees after OWHTO have not been sufficiently reported. In the present study, we retrospectively evaluated the preoperative lower limb alignment and the CA with respect to their influence on postoperative lower limb alignment and clinical results. The purpose of this study was to clarify the indication for OWHTO in terms of lower limb alignment to achieve satisfactory clinical results.
Materials and methods
Ninety-two patients (98 knees) with medial compartment knee OA were investigated in this study. The patients comprised 62 women and 20 men. The average follow-up period was 34 months (range, 24–68 months). The average age of the patients at the time of surgery was 63 years (range, 41–77 years).
The CA was determined based on a postoperative FTA of 170° and a postoperative 70% percentile of the lower limb mechanical axis on the tibial plateau (%MA; the medial margin of the tibial plateau was 0% and the lateral margin was 100%) using the preoperative anteroposterior full-length radiographs of the lower limbs in the supine position.
Knee arthroscopy was performed on all patients to evaluate the extent of cartilage degeneration. The lateral compartment was confirmed to be almost normal in all knees. Assessment of the medial compartment was based on the condition of the medial meniscus and cartilage, and debridement was performed according to the degree of degeneration and damage. Microfracture was additionally performed in the medial compartment when the cartilage on the medial femoral condyle or surface of the tibia was severely worn and the subchondral bone was exposed. All surgical procedures were performed using the method described by Lobenhoffer and Agneskirchner. 18 The superficial medial collateral ligament and pes anserinus were dissected from the medial cortex of the tibia, and an osteotomy was performed. The lower limb alignment was confirmed under an image intensifier during the operation. Beta-tricalcium phosphate blocks were inserted into the osteotomy gap, and the osteotomy site was fixed with a locking compression plate (Figure 1). Muscle strength and range of motion (ROM) exercises were started on the first day after surgery. Partial weight bearing was permitted from 1 week after surgery, and full weight bearing was permitted from 4 weeks after surgery. However, partial weight bearing was not permitted until 3 weeks after surgery in patients with microfractures. 9,13 The locking plates and screws were removed about 18 months after OWHTO.

Anteroposterior radiographs of knee before and after OWHTO. (a) Preoperative radiograph of a 76-year-old woman with medial compartment OA of the right knee. The OA was determined to be Kellgren–Lawrence grade III. (b) Postoperative radiograph of the right knee at 12 months after OWHTO. Beta-tricalcium phosphate blocks were inserted into the osteotomy gap, and the osteotomy site was fixed using a locking compression plate. OWHTO: opening wedge high tibial osteotomy; OA: osteoarthritis.
The radiological and clinical results were investigated from preoperatively to the final follow-up. The preoperative and postoperative FTA and %MA were evaluated using anteroposterior full-length radiographs of the lower limbs while weight bearing (Figure 2). The patients were divided into the following two groups by the preoperative FTA on anteroposterior full-length radiographs of the lower limbs while weight bearing. This grouping was performed with reference to a report on the performance of OWHTO using a navigation system.
10
However, a navigation system was not used in the present study, and the accuracy and intelligibility of the measurements were considered. Twenty-nine knees with a preoperative FTA of ≥185° were defined as the severe varus knees (S group), and the remaining 69 knees with a preoperative FTA of <185° were defined as mild varus knees (M group).The OA stages were evaluated by the Kellgren–Lawrence grading system.
19
The details of patients in the two groups are shown in Table 1. The patients’ knees were also classified by the postoperative FTA as follows: those with a postoperative FTA of >175° were defined as undercorrected, those with a postoperative FTA of 165–75° were defined as ideally corrected, and those with a postoperative FTA of <165° were defined as overcorrected. The FTA, %MA, CA, ROM, and Lysholm score were also compared between the two groups. The proportions of ideally corrected, undercorrected, and overcorrected knees were compared between the two groups. The Mann–Whitney

Evaluation of lower limb alignment. The anteroposterior full-length radiograph of the left lower limb while weight bearing after the locking plate and screws had been removed is shown in this figure. (a) FTA. The FTA was defined as the lateral angle between the FASA and the TASA. (b) %MA. The medial margin of the tibial plateau was 0% and the lateral margin was 100%. %MA = B / A × 100. FTA: femorotibial angle; FASA: femoral anatomical shaft axis; TASA: tibial anatomical shaft axis; %MA: percentile of the lower limb mechanical axis on the tibial plateau.
Patients’ characteristics.

S: severe varus; M: mild varus; F: female; M: male; BMI: body mass index; FTA: femorotibial angle; %MA: percentile of the lower limb mechanical axis on the tibial plateau; K-L: Kellgren–Lawrence.
This study was approved by the authors’ institutional review board (approval number 16-11-09).
Results
The FTA and %MA were significantly improved in both the S and M groups postoperatively (

Postoperative lower limb alignment. (a) The postoperative FTAs were significantly larger in the S group than in the M group. (b) The postoperative %MAs were significantly smaller in the S than M groups. FTA: femorotibial angle; %MA: percentile of the lower limb mechanical axis on the tibial plateau; S group: severe varus group; M group: mild varus group.

CAs. The CAs were significantly larger in the S group than M group. CA: correction angle; S group: severe varus group; M group: mild varus group.

ROM of knees after OWHTO. (a) The postoperative flexion angles of the knees were significantly smaller in the S group than in the M group. (b) The postoperative extension angles of the knees were significantly smaller in the S than M groups. ROM: range of motion; OWHTO: opening wedge high tibial osteotomy; S group: severe varus group; M group: mild varus group.

Postoperative Lysholm scores. The postoperative Lysholm scores were significantly lower in the S group than in the M group. S group: severe varus group; M group: mild varus group.
The frequencies of undercorrection, ideal correction, and overcorrection are shown in Table 2. More undercorrected knees were observed in the S than M groups (
Frequencies of undercorrected, ideally corrected, and overcorrected knees.a
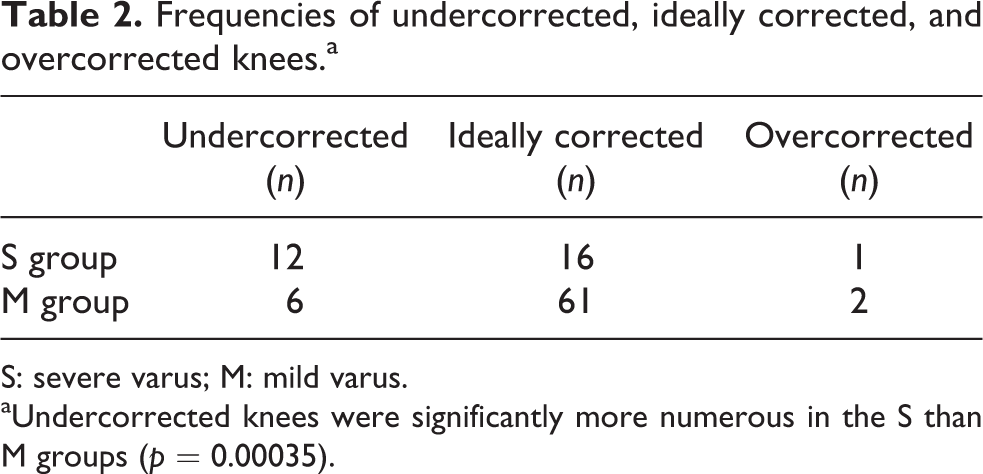
S: severe varus; M: mild varus.
aUndercorrected knees were significantly more numerous in the S than M groups (
Discussion
Lower limb alignment and the clinical results after OWHTO were evaluated in this study. The S group tended to include more undercorrected knees after OWHTO than the M group, although the difference in the postoperative average FTA was only 1.1° between the two groups. Additionally, a high proportion of knees with severe varus preoperatively were undercorrected after OWHTO, although their CAs were comparatively large. Creation of the necessary gaps to achieve lower limb alignment consistent with the preoperative plan might be difficult because of the tightness of the soft tissue around knees affected by advanced OA and severe varus. The soft tissue including the deep medial collateral ligament and knee joint capsule, which were basically left untreated during OWHTO, were thought to produce relatively strong resistance against the knee valgus correction in patients with S group. Alternatively, correction loss might occur just after insertion of beta-tricalcium phosphate blocks into the osteotomy gap. The blocks might be slightly compressed before the osteotomy site is fixed with a locking compression plate. The reasons for overcorrection of the lower limbs after OWHTO in the present study, especially knees with severe varus, remain unclear. Overcorrection might also be influenced by the condition of the soft tissue around the knees. A preoperative evaluation of the soft tissue might be needed. The postoperative clinical results were generally excellent and significantly improved in both groups, although the scores were better in knees with mild varus than severe varus. The postoperative ROM was more restricted in those with severe than mild varus. The reason for this is that the OA stages were relatively advanced in knees with severe varus.
A preoperative FTA of <185° is generally included as a criterion for OWHTO. 5,10,17 However, no reports have described the detailed reasons for adopting this criterion. The results of the present study showed that achieving the ideal lower limb alignment and satisfactory clinical results after OWHTO was difficult in knees with severe varus. In principle, OWHTO should be performed in knees with a preoperative FTA of <185°.
The clinical results in the present study were better than those after HTO when the postoperative FTA was about 170°. 11,20,21 The CA was, therefore, determined based on a postoperative FTA of 170° in several reports. 5,10,16 Bito et al. 10 used a navigation system and reported that the ideal lower limb alignment after OWHTO was an FTA of 168–172°. A navigation system was not used in the present study. The accuracy and intelligibility of the preoperative, perioperative, and postoperative measurements were considered. We therefore defined ideal, undercorrected, and overcorrected lower limb alignment as a postoperative FTA of 165–175°, >175°, and <165°, respectively. The range of ideal lower limb alignment in the present study was comparatively wide. The number of ideal lower limb alignments using FTA after OWHTO decreased when the range employed by Bito et al. 10 was used. The criteria must be stricter or the surgical technique, including the procedures involving soft tissue, should be further developed to more accurately attain the ideal lower limb alignment after OWHTO. Satisfactory clinical results of CLWO have also been reported. 9,16,22 The cases described in those reports included knees with severe varus.
Evaluations by patient-based scores were not performed in the present study. Therefore, the degree of the patients’ satisfaction was unclear. Based on our results, however, the satisfaction of patients with severe varus was predictably inferior to that of patients with only mild varus. Actual activities including the walking speed should also be investigated to determine whether OWHTO is truly beneficial in knees with severe varus. Patients with severe varus who are active and reluctant to undergo TKA should be advised that OWHTO is improper for knees with severe varus because postoperative lower limb alignment should be undercorrected to cause recurrence of the varus deformity with subsequent development of medial arthritis. A new device that can rigidly fix the osteotomy site for knees with severe varus deformity should be developed to improve the surgical quality of OWHTO along with the treatment of soft tissue. For example, locking plates of more than one size corresponding to the CA are thought to be needed. Alternatively, other osteotomy procedures such as CLWO could also be considered. One advantage of CLWO is a greater potential for correction. 22
Conclusion
A high rate of knees with severe varus preoperatively were undercorrected after OWHTO. A preoperative FTA of <185° should be included as a criterion for OWHTO alone, or a more effective technique for the treatment of soft tissue and new devices such as rigid fixing plates should be developed for OWHTO in patients with severe varus. Another osteotomy procedure such as CLWO can also be fitting for knees with severe varus.