
Abstract
Keywords
Introduction
Sub-Saharan Africa continues to experience the most severe impact from the global HIV epidemic. Current estimates indicate that this region is home to approximately 25.6 million individuals living with HIV, accounting for over two-thirds of all cases worldwide. 1 Countries in Eastern and Southern Africa bear particularly heavy disease burdens, with adult prevalence rates frequently exceeding 10% in several nations. 2 Within Ghana, HIV/AIDS remains a critical public health concern, with national prevalence currently estimated at 1.8%. By the conclusion of 2024, national surveillance data documented 334,721 people living with HIV across the country, with an additional 15,290 newly diagnosed cases reported during that year. 1 Among Ghana's sixteen administrative regions, the Volta region ranked seventh in terms of disease burden, recording 19,078 HIV/AIDS cases in 2024. 1
HIV/AIDS counselling has help to improve treatment outcomes among people living with HIV (PLHIV). Research has shown that counselling services in HIV/AIDS management has led to increased medication adherence among PLHIV, ultimately leading to improved viral load outcomes.3–6 Also, counselling services have helped PLHIV to better understand their illness, including symptoms and treatment plans and participate actively in the design of their treatment regimes. 7 Despite the importance of HIV/AIDS counselling, Africa, including Ghana, faces a significant shortage of trained HIV counselors. 8 This has placed a significant burden on the few counselors available.
In Ghana, HIV/AIDS counselors face significant challenges, with up to 47.7% of them not formally trained in the delivery of counselling services. 9 Moreover, negative attitude of HIV/AIDS clients, denial of their status, defaulting from treatment, lack of cooperation and some myth clients hold about HIV/AIDS have all been major challenges that HIV/AIDS counselors face.10–14 This has led to high levels of burnout, fatigue, traumatic stress and emotional exhaustion among HIV/AIDS counselors, compromising their psychological well-being.15–18 Hence, there is a need to identify the contextual psychological challenges that HIV/AIDS counselors face in in Ghana for prompt redress to enable them provide effective counselling services. Thus, identifying the psychological well-being challenges of HIV/AIDS counselors could help inform interventions to improve the health outcomes of HIV/AIDS counselors leading to improved service delivery. 19 This is paramount as Ghana aims to attain the 95-95-95 target of the United Nations by 2030. Thus, 95% of the population should be tested for HIV/AIDS by then of which 95% of those tested positive should be on antiretroviral therapy (ART) and of which 95% should achieved viral load suppression. 20
In Ghana's Volta Region, HIV prevalence ranks seventh nationally, with over 19,000 individuals living with HIV. 1 The region faces service delivery constraints such as limited psychosocial support staff and high client-counselor ratios, heightening the psychological strain on counselors.
Moreover, while numerous studies have focused on various aspects of HIV care and treatment in Ghana,21–27 research specifically addressing the psychological well-being of HIV/AIDS counselors is limited, necessitating the need for empirical evidence to elucidate the plight of HIV counselors in the country concerning their psychological well-being. Hence, we aimed to contribute to the literature by providing a descriptive phenomenological account of the self-reported psychological challenges, coping mechanisms, and suggested mitigation strategies of HIV/AIDS counselors in the Volta Region of Ghana, as depicted in Figure 1, by adopting the qualitative reporting guidelines of O’Brien et al. 28

Conceptual framework of the study.
Methods
Study Site Description
The research took place in five designated HIV/AIDS sentinel sites within Ghana's Volta Region. The region hosts 749 health facilities in total, comprising 29 hospitals, 156 health centers, 44 clinics, 4 polyclinics, 14 maternity homes, 452 CHPS compounds, and 50 private facilities. 29 Among these, the Volta Regional Hospital, Ho Teaching Hospital, Bator Catholic Hospital, Adidome Hospital, and Torgorme Hospital function as sentinel sites staffed with certified HIV/AIDS counselors. These five institutions were purposively chosen as the study locations.
Study Design
A qualitative descriptive phenomenological design was employed to explore psychological well-being challenges, coping mechanisms and suggested mitigation strategies of HIV/AIDS counselors in the Volta Region of Ghana. Thus, we aimed to comprehend the lived experiences of HIV/AIDS counselors in relation to the contextual psychological burden they face. 30 The reporting of this study conforms to the Standards for Reporting Qualitative Research (SRQR), a comprehensive framework for transparent reporting of qualitative studies across diverse paradigms and methodologies. 28 The completed SRQR checklist documenting adherence to all 21 reporting items is provided as Supplementary File 1.
Researchers’ Characteristics and Reflexivity
The study was carried out by a team of researchers which consist of a postgraduate public health student (FD), a senior lecturer (EM), and two lecturers (MA & VC), all with qualitative research experience. In order to bracket our biases, we documented our thoughts, feelings, and reactions in detail throughout the research process, allowing for ongoing reflection during the data collection process. 31
Study Population
HIV/AIDS counselors at the five (5) HIV/AIDS sentinel sites in Ghana's Volta region participated in the study. At the time of the study, there were twenty-five (25) trained HIV/AIDS counselors working at these locations, according to the Volta Regional Health Directorate's data. Out of these twenty-five (25) trained counselors, eighteen (18) fulfilled the requirements for inclusion, which included having been HIV/AIDS counselors for at least three (3) years. Nevertheless, at the time of data collection, two of these qualified counselors were not accessible for interviews.
Sample Size Determination and Sampling Procedure
When data saturation is achieved in qualitative research, the sample size is established. The research suggests that by the thirteenth interview, data saturation may be achieved. 32 However, because there were only 16 participants in the entire sample, we interviewed every eligible and accessible individual. 16 interviews were therefore thought to be adequate for the study, given that data saturation could be achieved by the thirteenth interview. All possible participants who were on duty and satisfied the inclusion requirements were contacted in order to conduct interviews for the study. Therefore, in order to find eligible volunteers for the study at the various sentinel locations, the census approach was used.
Data Collection Tool and Procedure
We conducted interviews using a semi-structured interview guide that focused on the core research questions while allowing participants the flexibility to express themselves freely. This approach also enabled the researchers to probe for deeper insights. The guide covered four thematic areas: the sociodemographic characteristics of participants, the psychological challenges they encountered, their coping mechanisms, and their recommended strategies for mitigating these challenges as HIV/AIDS counselors.
Before the main data collection, we pre-tested the guide with two HIV/AIDS counselors from the Oti Region, which shares similar demographic characteristics with the Volta Region. This pre-test helped us identify and refine questions that required revision. We conducted the actual interviews between June 10 and July 17, 2023.
Under the direction of the team lead (EM), the Principal Investigator (FD) and an experienced team member (MAA) moderated all interviews. Each session lasted an average of 45 minutes and was conducted in English. We held the interviews in private rooms within the medical facilities to ensure confidentiality. We used a Sony voice recorder to capture the discussions, while a team member (MAA) simultaneously took handwritten notes to document nonverbal cues. The Principal Investigator (FD) managed the recording process, and the handwritten notes were later integrated into the transcripts to provide contextual depth.
Data Analysis
We transcribed each interview and compiled the transcripts into Microsoft Word files. Using ATLAS.ti version 7.5, we developed codes, subthemes, and themes from the data. Two members of the research team (FD and EM) analyzed the data following Colaizzi's descriptive phenomenological analytical framework. 33 The analysis involved the following steps: (1) reading the transcripts multiple times to gain a holistic understanding of the content; (2) identifying and documenting key statements related to the phenomenon under study; (3) deriving meanings from these statements; (4) grouping the meanings into clusters, subthemes, and overarching themes; (5) integrating the results into a comprehensive description of the phenomenon; (6) formulating the fundamental structure of the experience; and (7) conducting member checking with seven participants to validate the descriptive findings.
We held regular meetings within the research team to discuss and confirm the authenticity of the emerging themes and subthemes. An impartial reviewer served as an arbitrator to resolve any disagreements during analysis. The team approved a theme only when full consensus was reached. We used participants’ direct quotations to support and strengthen the study's conclusions.
Rigor
Using Lincoln and Guba's criteria, 34 we made sure our results were credible by doing the following. Before the study started, we first built rapport with the participants and encouraged them to freely give important but sensitive information. Additionally, we sought advice from colleagues with experience in qualitative research, who helped with the study design right away. The inclusion of qualified qualitative researchers on the research team and their assessment of our procedures, transcripts, and results to reduce bias ensured the reliability of the study's conclusions. By giving a thorough explanation of the procedures, the findings’ transferability was guaranteed and they could be repeated in comparable contexts if necessary. In order to validate the accuracy of the researcher's interpretations and make sure the conclusions were based on the experiences of the participants, seven of the participants reviewed the transcripts and the results for approval. This ensured confirmability.
Results
Sociodemographic Characteristics of Participants
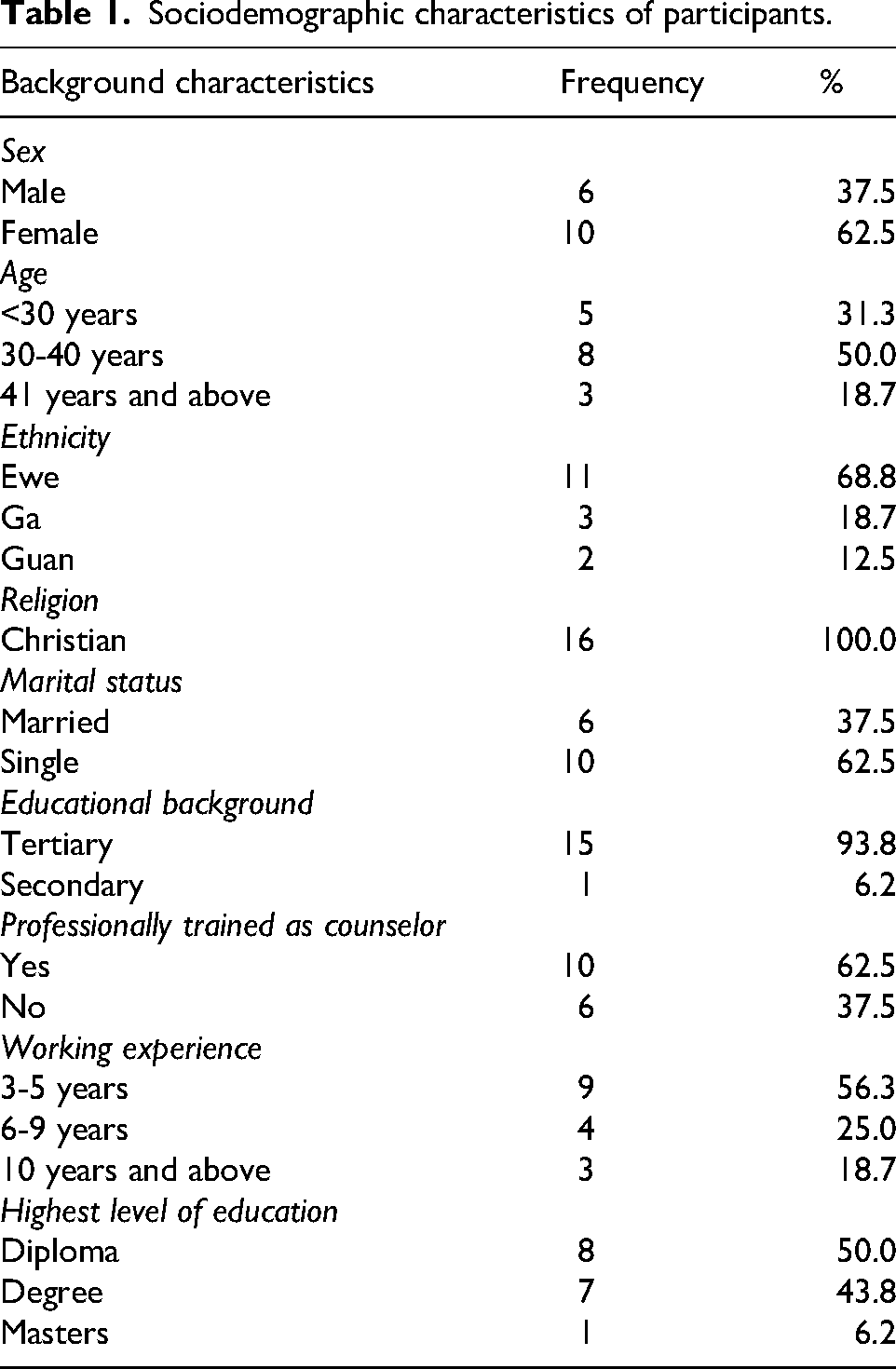
A total of sixteen (16) counselors took part in the study. Women formed the majority, representing 62.5% of the participants. Half of the group (50%) were aged between 30 and 40 years, while more than two-thirds (68.8%) identified as Ewe. All respondents (100%) were Christians, and most (62.5%) were single. Almost all of them (93.8%) had attained tertiary-level education, and more than half (56.3%) had at least three years of counseling experience (Table 1).
Sociodemographic characteristics of participants.
Thematic Findings
Three (3) global themes (psychological well-being challenges of HIV/AIDS counselors, coping mechanisms and recommendations for addressing these challenges were identified. Their accompanying themes, subthemes and sample quotes are presented in Table 2.
Thematic findings.

Psychological Well-Being Challenges of HIV/AIDS Counselors
The study ascertains the psychological well-being challenges faced by HIV/AIDS counselors in the Volta region of Ghana. Four subthemes emerged. These includes Stress, depression, anxiety, and anger.
Stress
Majority of the respondents indicated that their psychological well-being challenge as an HIV/AIDS counselor were stress. The quotations below summarize what participants had to say; So personally, I have not had any psychological challenge aside me been stressed up and sometimes feeling burnouts. (R12, Male, 28 years) I also feel stressed too in a way. This stress is caused by clients when they failed to cope with the counselling service you have given to him or her. Also, when I take a very long hour talk to a client over and over the same thing, I feel stress out. (R3, Male, 26 years)
Depression
Few of the respondents said their psychological well-being challenge as an HIV/AIDS counselor were depression. This sentiment was expressed in narratives such as; Sometimes I hear people's story and then you will become depressed and you will be like how can a person goes through difficulties like this. I have my own problems from home then you come to work then you come and hear another person problem and then you feel so bad. (R8, Female, 32 years) Yes, personally I will say I also experience in a way a mild depression. This is because handling a client who is all day crying, I feel emotional so in a way I feel depressed. (R7, Male, 37 years)
Anxiety
A few participants described experiencing fear of accidental exposure during HIV testing. As one counselor stated. The quotations below summarize what participants had to say; Also, I experience anxiety. Which is the fear that I will be pricked. For instance, when we are doing a test for somebody that is reactive first response and the last one you are to confirm and accidentally you pricked yourself. So, there is that fear because already you can sense that the person is positive and there is that fear that so me too am I coming to be an HIV positive client whiles trying to care for somebody. (R12, Male, 28 years) Sometimes anxiety sets in due to what the patient goes through. (R13, Female, 29 years)
Anger
Participants said their psychological well-being challenge as an HIV/AIDS counselor is been angry at clients and other healthcare workers. The quotation below summarizes what participants had to say; With the Psychological well-being challenge, I have not faced any as such but apart from maybe me getting angry. But on the normal day I get angry and displaced the cause on someone who is not the cause. The anger sometimes stems from the stuffs and sometimes is from the clients as well because if they fail to cooperate with us. (R10, Female, 29 years)
Coping Mechanisms of HIV/AIDS Counselors
The study identified two coping mechanisms adopted by HIV/AIDS counselors to cope with their psychological well-being challenges. This includes personal coping mechanisms and social/societal coping mechanism.
Personal Coping Mechanisms
Counselors described several personal strategies to help manage emotional strain. These included listening to music, meditation, yoga, taking time to rest, being fully conscious during testing procedures, accepting the nature of their work, and, routinely testing themselves for HIV for reassurance.
Recreational and Spiritual Activities
Most participants emphasized on recreational and spiritual activities as a personal coping mechanism with regards to the psychological well-being challenges they faced. The quotation below summarizes what participants had to say; I use music to cope with any psychological well-being challenge I experienced. I like music a lot. Sometimes I do meditation and YOGA once in a while but it is mainly the music. So, when I am stress, I listen to music then I am able to distress or get a better shape and then continue my work. (R8, Female, 32 years) Also, for the stress, I sleep perform YOGA and listen to music to distress myself. (R10, Female, 29 years)
Creating Conducive Working Environment
Another described creating moments of rest during stressful days. The quotations below summarize what participants had to say; As for the coping mechanisms I develop my own thing so sometimes if its overwhelming like that, I go out myself and sit at a place where I feel I will be okay. Not to go and drink alcohol but to relax myself. (R15, Female, 40 years) For my personal coping mechanisms, I make sure that I create a conducive environment to rest when I am stressed up. (R6, Female, 45 years)
Conscious in Conducting HIV Tests
Also, been conscious when conducting HIV test were identified as a personal coping mechanism. The quotations below summarize what participants had to say; But for the fear or the anxiety, the coping mechanism is to be very conscious with what you are doing and not to make a mistake to be pricked because it can psychologically worry you. So anytime I am doing a test for somebody, my focus is very conscious and do whatever I’m supposed to do. (R12, Male, 28 years)
Acceptance of Nature of Work
Another coping mechanism adopted by participant was acceptance of nature of work.
She narrated that; I have come to accept that during my cost of work, these are the people I will see so it's not really a problem. If not every day, every other day you see someone like that and every day you talk to them. Because of the information they had before coming to you, whatever you are saying they don’t want to let go of the old one and take the new one. (R2, Female, 35 years)
Routine Self-HIV Testing
Participant recounted that, conducting a routine self-HIV testing has been a personal coping mechanism adopted by her. This exemplified what she had to say; I sat down and realizes that in a health environment as a counsellor you will face challenges. So, for me not to let my client pass away again, I have decided that any patient we admitted here will be tested. So now the coping mechanism is that, the HIV testing is a routine activity in the hospital. (R1, Male, 35 years)
Social/Societal Support
The study also identified the social/societal support HIV/AIDS counselors in the Volta region of Ghana receive. Responses that emerged under this theme include: Motivation from family, motivation from clients, assistance from superiors at work, and assistance from key stakeholders.
Motivation from Family
Participants mentioned that, they receive motivational support from family members which enables them to be able to work effectively. The quotation below summarizes what a participant said; My wife always tells me that, you know the kind of work you are doing and at least you will face challenges. So, I should always relax because if I am stress out how can I provide counselling to my clients. So, I should always calm down. Sometimes too my co-workers motivate me and my matron. (R1, Male, 35 years) The family support has always been there because anytime I faced some any kind of challenges and discuss it with my people, they also try their possible best encourage me and tell me whatever they have to tell me and I become okay. (R10, Female, 39 years)
Motivation from Clients
Participant highlighted that HIV/AIDS counselors derive social support from client-driven motivation in their professional practice. The quotation below summarizes what participant said; Also, sometimes the clients give us incentives as a form of thanking us and motivating us for what we have done for them. (R12, Male, 28 years)
Assistance from Superiors at Work
When participants were asked to share the kind of support they received, some participants mentioned that they receive assistance such as refresher training from superiors. They shared; They take us through refresher training. The old things we are doing is exhausted, people are used to it so once a while they call for refresher training to refresh our minds, maybe bring new things on board. (R2, Female, 35 years) The coping mechanisms was that, I kept on passing enough information and also ask other colleges who are also a counsellor to come in. so we share the burden together and it really reduced the stressed on me. At a point in time the nurse manger was also instrumental and a lot of people come on board and it releases me the burden of stress alone. (R4, Male, 42 years)
Assistance from Key Stakeholders
Few participants mentioned that one of their social/societal support HIV/AIDS counselors were assistance from key stakeholders such as nongovernmental organizations (NGOs) and models of hope. The quotation below summarizes what a participant said; The societal support is that, the key stakeholders within the society makes the work easier for us sometimes. Initially the key stakeholders were very instrumental especially the chiefs. So, every festival you will see that the chiefs make sure in their speech they talk about it to their community. (R4, Male, 42 years) On the NGO side hope for future generation, they do organize training, workshops on HIV so it also helps to learn more about how to deal and cope with them. (R14, Female, 30 years)
Recommendations to Address Psychological Well-Being Challenges
Another theme that emerged from the study was measures to address psychological well-being challenges of HIV/AIDS counselors in the Volta region of Ghana. Again, five (5) subthemes were identified under this theme. These include; assigning clinical psychologists to counselors, Education on HIV/AIDS, Cooperation from clients, Employing more HIV/AIDS counselors, and Provision of incentives to counselors.
Assigning Clinical Psychologists to Counselors
Most of the respondents said that, assigning clinical psychologists to HIV/AIDS counselors is a way to address the psychological well-being challenges faced by HIV/AIDS counselors in the Volta region of Ghana I think at least having a clinical psychologist at the all the ART units will help a lot because with this though they are going to assess our client as well but with the stuffs anything that you have relating to the psychological well-being can be discuss with them and they can show you a coping mechanism or some ways dealing with it. (R10, Female, 29 years) Also, a clinical psychologist must be employed in every health facility that is rendering this service so that they will be playing part in HIV/AIDS counselors Psychological well-being challenges because they have gone through a lot and deeper and have much experience than compare to us that have been train as an HIV/AIDS counselors. (R4, Male, 42 years)
Education on HIV/AIDS
Majority (9) of the respondent suggested that, educating client, society and health workers can address the psychological well-being challenge faced by HIV/AIDS counselors. The quotations below summarize what participants had to say; There should be more awareness and education to HIV/AIDS counselors on Psychological well-being. Even sometimes what we considered it not to be psychological well-being problem is rather a psychological well-being issue. (R8, Female, 32 years) There should be more education to both health workers and HIV/AIDS counsellors. Also, there must be more encouragement and support from the government both financially, physically and mentally. As a counsellor, you need a sound mind before you can carry on your daily working activities. So, if you are hungry, how can you be sound minded. (R1, Male, 36 years)
Cooperation from Clients
Few respondents suggested that, client cooperating with them will address the psychological well-being challenge faced by HIV/AIDS counselor Our clients should be more cooperative; they should come on their scheduled dates as appointed because when you meet your appointment you are out of medications. With them being cooperative reduces my work load and reduces my stress so it will help. (R14, Female, 30 years) I think for the client they should comply and cooperate with whatever we tell them and this will help us to reduce the stress and the burnout or any other form of psychological well-being challenge. This is because when they are happy then we are also happy. (R6, Female, 45 years)
Employing More HIV/AIDS Counselors
Most of the respondents said that, to address the psychological well-being challenge faced by HIV/AIDS counselors, the government should employ more HIV/AIDS counselors. The quotation below summarizes what participants had to say; Also, more health personnel should employ in the care of clients and to impedes the progress of the work. The counselors to client ratio are high so there is much workload in the system which increases stress among us. (R3, Male, 26 years)
Provision of Incentives to Counselors
Participants proposed that offering incentives to HIV/AIDS counselors could serve as an effective strategy to alleviate their mental health challenges. The quotations below summarize what participants had to say; Moreover, intermittently there should be an incentive in a form of motivation and encouragement to improve upon our Psychological well-being challenges. (R15, Female, 40 years) HIV care is a project on it own that is been funded by donors so as they planned for the client they should think of the counselors or we the health workers too because it has the highest risk. So, as they planned for the client, they should be planned for those who are engaged with the clients too. (R15, Female, 40 years)
In summary, the findings show that HIV/AIDS counselors experience a range of interconnected psychological well-being challenges, including stress, anxiety, depression, and emotional exhaustion, arising from the demands of their work and interactions with clients. Counselors rely on a combination of personal coping strategies, such as rest, music, meditation, and conscious awareness during testing, as well as social support from family, colleagues, and supervisors to manage these challenges. They also proposed several practical recommendations for strengthening their well-being and improving service delivery, including increased staffing, access to clinical psychologists, refresher trainings, and greater community education. Together, these insights highlight the need for more structured institutional support to enhance the resilience and effectiveness of HIV/AIDS counselors.
Discussion
This study aimed to ascertain the psychological challenges and their associated coping mechanisms of HIV/AIDS counselors in the Volta region of Ghana. From the data, three (3) global themes were generated. These themes are: psychological well-being challenges of HIV/AIDS counselors, coping mechanisms as an HIV/AIDS counselor, recommendations to address these challenges.
Stress, depression, anxiety, and anger were the psychological challenges identified among HIV/AIDS counselors in the Volta region of Ghana. With regards to stress as a psychological wellbeing challenge among HIV/AIDS counselors, a similar assertion has been made in Uganda, where HIV/AIDS counselors were found to experience high levels of job-related stress, 35 and has also been widely reported in the literature globally.36–38 The high levels of stress faced by HIV/AIDS counselors could be as a result of long working hours, high caseloads, and inadequate support, leading to poor job performance, burnout, emotional exhaustion and reduced productivity.39,40 Implementing a support system for HIV/AIDS counselors could go a long way to reduce the stress-related challenges that HIV/AIDS counselors face in the Volta region of Ghana.38,39 With regards to depression, it has been reported that HIV/AIDS counselors who had been in the profession for longer periods of time are more likely to experience depression.41,42 This could be due to their constant provision of emotional support to people living with HIV/AIDS,43,44 conflicts with colleagues and clients, lack of support from superiors. 45 It is recommended that HIV/AIDS counselors receive regular training and support to help them cope with the emotional demands of their work, which often leads to depression. 35
Anxiety is another common psychological challenge faced by HIV/counselors as found in this study. 46 This, could be as a results of the fear of being living with HIV with HIV in the line of duty and the repeated exposure to the death of a client.19,37,47–49 Accidental exposures to bodily fluids, despite the low risk of transmission in a counselling setting could also cause anxiety among HIV/AIDS counselors, 50 and could make them may struggle to provide optimal support and services to clients. 36 Establishing peer support networks where counselors can share experiences, seek advice, and receive support from colleagues who understand the unique challenges of their work could help HIV counselors better cope with anxiety. 44
Anger was also reported as a psychological well-being challenge faced by HIV/AIDS counselors. Anger can stem from the frustration of dealing with systemic challenges, such as a shortage of staff and communication issues with management and clients. 51 HIV/AIDS healthcare providers witnessing or experiencing stigma and discrimination related to HIV/AIDS evoke anger directly toward the individuals perpetuating the stigma or toward societal structures that contribute to discrimination. 36 Sometimes the lack of resources for effective service delivery could lead to frustration and anger among HIV/AIDS counselors,15,52,53 which could have a negative impact on the quality of care given to clients. 54
The study also ascertained how HIV/AIDS counselors coped with the psychological challenges they faced. Two themes were identified under this global theme, personal coping mechanisms and social/societal support systems. With reference to personal coping mechanisms participants mentioned their indulgence in recreational and spiritual activities (listen to music, performance of YOGA and meditation), creating conducive working environment, being conscious in conducting HIV tests, acceptance of the nature of work, and routine self-HIV testing as some of the methods they adopted.
Music, YOGA and meditation are widely recognized as effective coping strategies for managing stress and improving psychological well-being in general. 55 Also, meditation has been reported in the literature as psychological well-being-related coping mechanism among HIV/AIDS counselors. 56 A similar assertion has been made 57 indicating that HIV counselors adopt coping strategies such as listening to music. Some may also engage in prayer, meditation, or other spiritual practices to find comfort and guidance as they recognize the importance of the mind-body connection in managing stress and improving psychological well-being. 58 Thus, engaging in activities that combine physical and mental aspects, such as yoga and meditation, can contribute to a holistic approach to coping. 59
Another individual psychological well-being-related coping mechanism adopted by participants was the creation of a conducive environment to rest. The use of adaptive coping strategies, such as creating a conducive environment for rest. Research has shown that rest and quality sleep is essential for preventing burnout, maintaining cognitive function, and sustaining mental resilience among HIV lay counselors. 15 Adequate rest contributes to stress reduction, emotional regulation, and overall well-being. 60 This finding could be that creating a conducive space for rest allows HIV/AIDS counselors to escape from the demands and pressures of daily life, providing a sense of calm and tranquility. 37 Hence, encouraging HIV/AIDS in the Volta region of Ghana to have enough rest through sleep could afford them the psychological strength needed to assist their clients. 61
Being conscious when conducting HIV tests was another coping mechanism reported by participants. This heightened awareness, which involves paying deliberate attention to each step of the testing process, has been recognized across healthcare settings as an important approach in caring for clients with infectious or highly contagious conditions.22,62 HIV/AIDS counselors often maintain this state of focused attention to avoid errors that could expose them to infection, ensuring both their own safety and that of their clients. 63 This idea of “being conscious” closely aligns with the concept of mindfulness, which is increasingly emphasized in the health professions literature as a beneficial strategy for managing stress and improving clinical performance. Mindfulness involves intentionally maintaining moment-to-moment awareness of one's actions, emotions, and surroundings, and has been shown to enhance emotional regulation, reduce anxiety, and support better decision-making among healthcare workers. By remaining consciously attentive during testing procedures, counselors in this study appear to engage in an intuitive form of mindful practice. This approach not only helps reduce their stress and anxiety but also contributes to a safer and more supportive environment for individuals undergoing HIV testing. 64 A mindful, fully present counselor can foster trust, encourage openness, and enhance the quality of the counseling interaction, suggesting that incorporating structured mindfulness-based interventions could further strengthen the psychological well-being of HIV/AIDS counselors.
Moreover, participants accepted the nature of their work in order to help them cope better with psychological challenges they faced. Acceptance, in this context, means acknowledging the emotional impact of the work without judgment. HIV/AIDS counseling often involves delivering difficult news and navigating emotionally charged situations and the recognition of this allows them to process and coped with their emotions more effectively14,65 Sowell & Phillips 66 stated that healthcare workers including HIV/AIDS counselors often work in an environment of uncertainty, where outcomes are not always predictable, and emotions can be intense. Therefore, accepting the work as it enables counselors to let go of undue stress related to uncertainty and establish and maintain healthy emotional boundaries, preventing emotional exhaustion.67,68
Another coping mechanism reported by HIV/AIDS counselors was making HIV testing a routine activity. Routine HIV testing involves offering testing to all individuals as a standard part of medical care, regardless of their perceived risk. 69 Undergoing a routine HIV testing as a counselor provides an opportunity to engage with clients in a proactive and supportive manner, fostering a culture of openness and awareness and ought to be encouraged among all counselors in the region as it align with the concept of “treatment as prevention” in healthcare. 70
Also, various social support systems were found to aid HIV/AIDS counselors in coping with the psychological challenges they faced. These systems include motivation from family and clients, assistance from superiors at work, and assistance from key stakeholders such as NGOs. It has been reported that family members can play a significant role in motivating counselors by understanding them and encouraging them to seek help when necessary.71,72 Family support can also enhance counselor's sense of self-efficacy and overall well-being 73 as family understanding and empathy toward HIV counselor help them feel validated and supported in their work. 21 Clients were also found to be a key source of motivation in dealing with psychological challenges that HIV/AIDS counselors faced. The finding sheds light on the reciprocal nature of support within the client-counselor relationship. 74 Clients have been found serve as a source of inspiration for HIV/AIDS counselors enhancing their and dedication to work37,50,75 The praise counselors receive form their clients motivates them and serve as a source of emotional nourishment for their work. 74 Such form of motivation make counselors recognize the important role they play in providing support and care for their clients. 76 Hence, clients should be encouraged to recognizing and celebrate their caregiver when necessary to contribute to to creating a positive work environment and reduce the risk of burnout among counselors. 77
Furthermore, counselors discussed their psychological challenges with their head of departments (in-charges) as a form of coping mechanism. Supervisors and in-charges play a crucial role in setting the tone for workplace culture and promoting open communication, therefore by actively engaging with their supervises and providing a safe space for discussions contribute to a more resilient and emotionally healthy workforce. 80 It serves as a form of debriefing and emotional release for counselors, allowing them to express their thoughts and feelings in a supportive environment. 50 Thus, heads of HIV/AIDS counseling units should be encouraged to be discussing issues with their subordinates to help mitigate the emotional burden associated with their work and prevent burnout. 78
Refresher training courses were identified as another layer of coping with psychological challenges among HIV/AIDS counselors. Refresher training serves as a valuable tool for counselors to enhance their professional competencies, stay updated on best practices, and address the emotional demands of their work. 79 The field of HIV/AIDS care is dynamic, with new research, treatment modalities, and best practices constantly emerging, hence refresher training served as a platform for counselors to engage in self-care and emotional well-being activities. 40 Thus, managers of health facilities in the region, the Ghana AIDS Commission and the Ghana Health Service need to constantly organize refresher training programs for HIV/AIDS counselors in the country to constantly improve their skills and knowledge on the disease.
In addition, key stakeholders such as religious groups and NGOs that assist HIV/AIDS counselors to make their work easier was identified as a crucial social support system. These key stakeholders play a crucial role in the social fabric of a community affected by HIV/AIDS. 80 When influential key players of a community are engaged in supporting the work of HIV/AIDS counselors, it sends a powerful message of acceptance and understanding, 80 ultimately reducing the workload and stress HIV/AIDS counselors go through. 65 Hence, community mobilization and support for HIV should be promoted by the Ghana Health Service in the region.
Participants also suggested various ways through which the psychological challenges they experience could be better managed. Five key suggestions were made. These include assigning clinical psychologists to counselors, education on HIV/AIDS, cooperation from clients, employing more HIV/AIDS counselors, and provision of incentives to counselors.
Assigning clinical psychologists to work alongside with HIV/AIDS counselors had provides them professional support and guidance that help them cope with their emotional and psychological demands of their work and prevented burnout. 14 The presence of clinical psychologists can also contribute to a more comprehensive approach to client care, 48 as clinical psychologists has undergone thorough training, possess sufficient expertise in handling psychological well-being issues, and can offer guidance on self-care practices for counselors. 81
Moreover, participants recommended educating the client, the society and the health workers on HIV/AIDS, as it can help address the psychological well-being challenged faced by HIV/AIDS counselors. To this end, Stockton et al 71 opine that education is an important tool in the HIV prevention treatment and care continuum, especially when focused on providing training and knowledge about the condition psychological well-being of those living with disease and care providers, including counselors. This can help reduce stigma and increase understanding and empathy toward counselors by providing accurate information about the condition.75,82 Hence, community and tailored education on HIV/AIDS should be intensified by the Ghana Health Service in the region to improve knowledge and understanding on the condition.
Also, cooperation from clients was revealed as a potential way to address the psychological well-being challenge faced by HIV/AIDS counselors in the Volta region. This assertion is in accordance with a study conducted by Karki et al 83 in India, who found that cooperation from clients is a key factor in addressing psychological well-being challenges among HIV/AIDS counselors. Thus, when clients actively engage in the counselling process and show willingness to participate in their own care, it can have a positive impact on the mental well-being of HIV/AIDS counselors. 41 Positive client cooperation creates a supportive and trusting environment, which is crucial for effective counseling. 84 Client cooperation is assured when they are not stigmatized by the society, including healthcare workers. 85 Hence, efforts should be made by the Ghana Health Service and the Ghana AIDS commission to ensure that HIV/AIDS-related stigma is reduced to the barest minimum.
Also, employing more HIV/AIDS counselors to add to the existing workforce was mentioned as another means of addressing the psychological well-being challenges faced by HIV/AIDS counselors in the Volta region. The demand for HIV/AIDS counselors is high, and employing more counselors can help alleviate the workload and reduce stress among existing counselors leading to the provision of quality care to clients.59,86 By increasing the number of counselors, the workload can be distributed more evenly, allowing counselors to provide more focused and individualized support to their clients. 87 The Ghana Health Service should thus prioritize the recruitment of HIV/AIDS counselors to augment the meager numbers in the system.
Finally, incentive as a form of motivation was mentioned as a potential measure to address the psychological well-being challenges faced by HIV/AIDS counselors. Incentives can serve as a form of motivation, encouraging counselors to continue their valuable work and maintain their own psychological well-being. 14 A study conducted by Kim et al 38 revealed that, providing incentives can help attract and retain qualified professionals in the field of HIV counseling. For instance, NGOs can provide funding for psychological well-being support programs, organize training workshops and peer support groups, and advocate for better working conditions for counselors and ensure that they have access to the resources they need. 44 Thus, specialized incentive packages should be designed for HIV/AIDS counselors in the region and the country as a whole to help improve the psychological well-being of HIV/AIDS counselors in the region leading to better service delivery outcomes.
In interpreting these findings, it is important to consider the broader political and funding climate surrounding HIV/AIDS programming in Ghana. Recent reductions in donor funding and budgetary allocations for HIV prevention, treatment, and support services have increased operational pressures on healthcare facilities and frontline staff. These constraints may intensify the psychological burden experienced by counselors, as limited resources, staff shortages, and increased caseloads create a more demanding work environment. The study was conducted before these recent funding cuts, suggesting that the challenges reported by counselors may now be even more pronounced. Acknowledging this context underscores the urgency of strengthening mental health support systems and ensuring sustainable investment in HIV/AIDS services to protect both counselor well-being and the quality of care delivered to clients.
Table 3 summarizes actionable recommendations and their potential impact on improving counselors’ psychological well-being and HIV treatment outcomes.
Summary of key recommendations for policy and practice.

Strengths and Limitations of the Study
This study is limited by its relatively small sample size and the fact that it was conducted in only five sentinel sites in the Volta Region. Although data saturation was achieved, the findings may not fully represent counselors in other regions. As with all qualitative research, the results reflect the subjective experiences of participants and may be influenced by recall or social desirability bias. While member checking strengthened internal validity, external validity remains limited due to the context-specific nature of the study. However, the detailed description of the setting and methodology enhances the transferability of the findings to similar contexts.
Conclusion
This study aimed to identify the different psychological well-being concerns that HIV/AIDS counselors in Ghana's Volta area encountered, along with their different coping strategies and the methods they used to deal with these issues. These results underscore the need to prioritize counselor well-being to enhance HIV counseling efficacy and support Ghana's 95-95-95 targets by 2030. The Ghana AIDS Commission and the Ghana Health Service must contextualize and address the psychological well-being challenges faced by HIV/AIDS counselors nationwide, taking into account their suggested mitigation strategies and recommendations, such as capacity-building training and psychosocial support, to mitigate challenges and improve service delivery across the country.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251414813 - Supplemental material for Psychological Well-Being Challenges and Associated Coping Mechanisms of HIV/AIDS Counselors in the Volta Region of Ghana: A Descriptive Phenomenological Study
Supplemental material, sj-docx-1-jia-10.1177_23259582251414813 for Psychological Well-Being Challenges and Associated Coping Mechanisms of HIV/AIDS Counselors in the Volta Region of Ghana: A Descriptive Phenomenological Study by Veronica Okwuchi Charles-Unadike, Festus Dwomoh, Mary Akua Ampomah and Emmanuel Manu in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251414813 - Supplemental material for Psychological Well-Being Challenges and Associated Coping Mechanisms of HIV/AIDS Counselors in the Volta Region of Ghana: A Descriptive Phenomenological Study
Supplemental material, sj-docx-2-jia-10.1177_23259582251414813 for Psychological Well-Being Challenges and Associated Coping Mechanisms of HIV/AIDS Counselors in the Volta Region of Ghana: A Descriptive Phenomenological Study by Veronica Okwuchi Charles-Unadike, Festus Dwomoh, Mary Akua Ampomah and Emmanuel Manu in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We acknowledge the contributions of our study participants for the realization of this study and its publication thereof.
Ethical Approval and Informed Consent
Ethical approval for this study was obtained from the Ethics Review Committee of the University of Health and Allied Sciences (UHAS-REC A.10 [041]22-23). Written informed consent was obtained from all participants before interviews commenced. All participants were informed of their right to withdraw at any time. Confidentiality and anonymity were strictly maintained.
Consent for Publication
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
FD and EM conceptualized the study. FD, VOC, and MAA collected the data. FD and EM analyzed the data and drafted the manuscript. All authors reviewed and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.