
Abstract
Keywords
Introduction
Universal Neonatal Hearing Screening (UNHS) is well established within the health-care system in the United Kingdom and in many other countries across the world. The introduction of UNHS has successfully reduced the median age at diagnosis of permanent childhood hearing impairment (PCHI) to 3 months or less from 2.75 years (Kennedy, Kim, Campbell, & Thornton, 1998; Uus & Bamford, 2006; Watkin & Baldwin, 2012). The Hearing Outcome Project (Kennedy et al., 2006) reported that UNHS was associated with better language scores for hearing-impaired children. The early management of hearing loss through hearing aid fitting is considered an essential initial step for improving the communication and auditory abilities of children born with PCHI (Yoshinaga-Itano & Sedey, 1999). However, speech and language outcomes still vary widely for these children due to a number of child and family factors (Ching, Dillon, Marnane, Hou, & Day, 2013). Child factors include nonverbal intelligence, educational input, additional disabilities, the etiology and severity of deafness, and the age at which amplification (hearing aids or cochlear implant [CI]) was provided. Sininger, Grimes, and Christensen (2010) reported that the age at fitting of amplification had the single largest effect on outcomes. The quality of hearing aid provision in the United Kingdom was transformed by the Audiology Modernisation project (Bamford, Ankjell, et al., 2005; Bamford, Skipp, et al., 2004). However, delays for hearing aid provision and CI referral remained, although many researchers have highlighted the importance of early cochlear implantation in children to improve speech and language outcomes (Ching et al., 2013; Geers & Nicholas, 2013; Ostojić, Djoković, Dimić, & Mikić, 2011).
Family factors include participation in rehabilitation, mother–child interaction, maternal education level, socioeconomic status, and communication mode. Watkin, Baldwin, and Laoide (1990) demonstrated that parents often had difficulties recognizing the impact of hearing impairment through observation of their infants in the home, especially for mild or moderate impairments. They concluded that the delays in hearing aid fitting and consistent use could in part be attributable to the lack of parental awareness of the hidden difficulties their infants have in hearing speech. Further support should be provided to demonstrate difficulties and improve parental understanding.
Cortical auditory evoked potentials (CAEPs) give an objective measure of a response to auditory stimuli, including speech sounds. The responses originate from neurons at the level of the primary auditory cortex and from the auditory association areas in the temporal lobe (Cone-Wesson & Wunderlich, 2003). The latency and amplitude characteristics of CAEP responses are determined primarily by the acoustic parameters of the stimulus and the integrity of the primary auditory pathway. There are three major components in the recorded response referred to as the P1-N1-P2 complex (Cone-Wesson & Wunderlich, 2003). The response can be recorded in infants who are too young to respond behaviorally both unaided and also with hearing aids on to assess improved detection of speech stimuli (Barnet, 1971; Dillon, 2005; Glista, Easwar, Purcell, & Scollie, 2012; Korczak, Kurtzberg, & Stapells, 2005; Purdy et al., 2005). The assumption is that if a CAEP response is present for a specific sound, then it must be audible (Purdy & Kelly, 2008; Stapells, 2009). CAEP responses have been recorded in cases of auditory neuropathy spectrum disorder (ANSD) when early latency electrophysiological responses (auditory brainstem responses [ABRs]) are absent (Pearce, Golding, & Dillon, 2007). Rance, Cone-Wesson, Wunderlich, and Dowell (2002) showed CAEP responses to be present in children with ANSD who had open-set speech perception ability and benefit from amplification.
CAEP responses are not always consistently present in hearing-impaired children. Van Dun, Carter, and Dillon (2012) showed that around 25% of hearing-impaired children do not evoke a response to speech stimuli presented at 10 dB sensation level (SL) or 10 dB above the auditory threshold. This may indicate that late latency evoked potentials are less stable than the early evoked potentials (Carter, Golding, Dillon, & Seymour, 2010). However, the infant’s state of arousal is known to affect the morphology and detection of a CAEP response (Suzuki, Yamamoto, Taguchi, & Sakabe, 1976), and therefore, they are not always detectable even at low and medium SLs when it would be expected that the sounds are audible. This highlights the importance of normative data, carefully controlled recording conditions, and confidence measures for intensity levels and different types of stimuli. With this, CAEPs may have a role for systematically evaluating aided and unaided responses. Research undertaken by National Acoustic Laboratories used short speech sounds with low-, mid-, and high-frequency content, presented in the free field, to record unaided and aided hearing in infants as part of their clinical assessment (Chang, Dillon, Carter, Van Dun, & Young, 2012; Dillon, 2005; Pearce et al., 2007).
Audiologists face a challenge when recommending hearing aids for milder degrees of hearing loss (Bagatto & Tharpe, 2013; Fitzpatrick, Whittingham, & Durieux-Smith, 2014), and it can be difficult to confidently prescribe hearing aids without behavioral testing which is typically conducted from around 6 months of age. The CAEP response to speech sounds can be recorded from 3 months and therefore potentially offer earlier confirmation of an infant’s access to speech sounds.
The implementation of CAEP using the HEARLab® device began in Australia in 2011. Punch, Van Dan, King, Carter, and Pearce (2016) report a retrospective review of 83 infants with PCHI, fitted with hearing aids using evoked potential tests and prescriptive targets according to their national protocol. In addition, aided CAEP responses were recorded within 8 weeks of the initial fitting. CAEP results were used to confirm unaided hearing capability and to modify the initial hearing aid fittings. Their findings indicated that CAEP testing influenced the effectiveness of rehabilitation and that CAEP testing was well received by parents. This led to the integration of CAEP testing into their routine infant fitting program.
In recognition of the potential contribution of CAEP testing, CAEP recordings were incorporated into the infant audiology pathway at one of the London Hospitals. CAEP recording was undertaken for infants after a PCHI had been confirmed by diagnostic ABR or auditory steady state response (ASSR) assessments but before hearing aids were fitted.
The goal of the current research was to determine the impact on patient management of introducing CAEP assessments into the audiological pathway for infants. Specifically, the age for hearing aid fitting and CI referral were analyzed and influential factors of family engagement, audiologist decision-making, and extent of hearing loss were explored.
Methods
Research and Development Approval
The study was registered as a clinical service evaluation with the NHS Trust in East London research and development department: registration number 1275. It was a cohort comparison study comparing a retrospective group, Cohort A, and a prospective group, Cohort B, and following the preschool audiological management.
Participants
The study was undertaken in a pediatric audiology service in East London. Data were analyzed from children who were referred from the Newborn Hearing Screening Programme (NHSP) hearing screen and who were identified with a PCHI between 2008 and 2015. A review of data from diagnosis of PCHI to school entry (at 5 years) was conducted. At the time of the analysis, the youngest child in the study with PCHI had reached 2.3 years of age. Children from all ethnic backgrounds and all spoken languages were included. Children with a primary diagnosis of ANSD, those with long-term mixed hearing loss due to otitis media or with additional learning or sensory disabilities, and comorbidities were excluded from the current analysis. This was to remove cases with known progressive or fluctuations in hearing loss following the recording of CAEP results. The study sample was divided into two separate cohorts based on the date of their audiological assessments. Cohort A consisted of babies born between January 2008 and August 2011 when the clinical pathways did not include the recording of CAEP measurements, and Cohort B consisted of babies born between September 2011 and April 2015 when CAEP recordings were included in the audiological pathways. The infants with PCHI were identified from the Easy Screening Programme database (British Society of Audiology, 2007; Stevens, Sutton, & Wood, 2013). The severity of hearing loss was categorized using the British Society Audiology descriptors (British Society of Audiology, 2011) as mild (20–39 dB HL), moderate (40–69 dB HL), severe (70–94 dB HL), and profound (>95 dB HL), using the average of hearing thresholds across 500, 1000, 2000, and 4000 Hz. This four-frequency average hearing loss (4FAHL) was derived from detection thresholds assessed with visual reinforcement audiometry (VRA) using warble tones through inserts to obtain ear-specific thresholds at 6 to 8 months.
Enrolled Participants
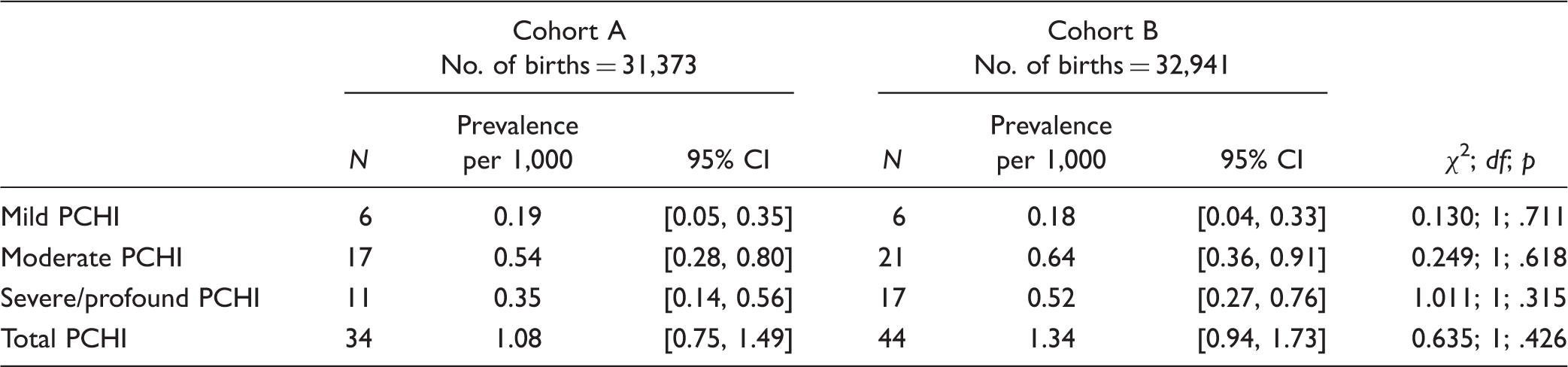
Cohort A consisted of 34 children with PCHI who were identified from the cohort of 31,373 babies born during the period from January 2008 to August 2011. There were 21 female and 13 male participants. In this cohort, 24 children had English as the second language and 10 had English as their first language. The United Kingdom follows the NHSP guidelines to diagnose children with hearing loss. These guidelines were the same for children prior to and post 2011.
Cohort B consisted of 44 children with PCHI identified from a cohort of 32,941 babies born between September 2011 and April 2015. There were 21 female and 23 male participants. Of the 44 children, 33 children had English as the second language and 11 had English as their first language.
Prevalence of PCHI by Degree of PCHI in the Two Cohorts.
Procedures
With both cohorts, the only change that was introduced in the patient pathway was the use of CAEP. Staff and clinical facilities remained the same, and the follow-up procedures were conducted according to the NHSP guidelines.
All the infants who were referred from the neonatal hearing screen followed a postscreen diagnostic test protocol which included ABR/ASSR, high-frequency tympanometry and otoacoustic emissions. This test battery was established and delivered by experienced audiologists (Baldwin & Watkin, 2014). Identification of PCHI prompted immediate referral for both peer to peer and educational support for families. The support was undertaken both within the home and in a center run by the Early Support Team for families of deaf and hearing-impaired children. This support was established in 2008 and remained unchanged throughout the period. From 2011, an unaided CAEP recording was offered within 6 to 8 weeks of the PCHI confirmation and those with a more severe loss were seen by 4 weeks, followed by hearing aid fitting. Aided recording of CAEP was offered within 4 to 8 weeks of the hearing aid fitting to determine the effectiveness of the amplification. Throughout the period of the study, all the children identified with a PCHI were regularly offered follow-up appointments with continued assessment using behavior observation audiometry, VRA, and eventually conditioned play audiometry. Multidisciplinary input was given by the teacher of the deaf and the peer-to-peer support worker. Figure 1 shows the flow chart summarizing the patient pathways for the two cohorts.
The patient pathway for Cohort A and Cohort B. ABR = auditory brainstem response; ASSR = auditory steady state response; CAEP = cortical auditory evoked potential; NHSP = Newborn Hearing Screening Programme; OAE = otoacoustic emission.
Cortical Auditory Evoked Potential
All cortical measurements and calibrations were made in a sound-treated and electrically screened test room using the HEARLab® system (Frye Electronics, 2013). The stimuli were the speech tokens /m/ (duration of 30 ms), /g/ (duration of 20 ms), and /t/ (duration of 30 ms), which were presented at nominal intensity levels of 55, 65, and 75 dB SPL, respectively, from a sound field speaker. These speech sounds have been described and justified in detail in research publications (Golding, Dillon, Seymour, & Carter, 2009; Carter et al., 2010; Chang et al., 2012). The speech tokens were presented with an interstimulus interval of 1,125 ms, as described in Munro, Purdy, Ahmed, Begum, and Dillon (2011) using the HearLab® system.
The speech tokens were analyzed to determine the spectrum and energy peaks of each sound (see Figure 2). Stimuli were recorded using a B&K reference microphone 4192 and a B&K nexus amplifier. The speech tokens were analyzed using the Audacity 2.0.6. software package.
Spectra of the three HEARLab® stimuli.
Automated calibration of the HEARLab® system was performed at 75 dB SPL in the sound field before each testing session (in accordance with manufacturer’s recommendations; Frye Electronics, 2013). Electroencephalography (EEG) bandpass filter settings and artifact rejection levels were set to 0.2 to 30 Hz and ±150 µV, respectively. The child’s vertex, forehead, and right mastoid were prepared using Nuprep gel to ensure good contact between the skin and the electrode. Snap-on disposable electrodes were positioned at the vertex as positive, right mastoid as negative, to keep consistency and reduce any experimental bias, with the forehead as ground with electrode impedance below 5 kΩ. A headband and surgical tape were used to stop the electrodes from slipping. Children were seated on their carer’s lap, 1 m from the loudspeaker. Responses were collected while the infants were alert, awake, and quiet throughout testing and while watching a subtitled DVD with the sound disabled or using visual toys to engage the child. The child’s EEG was recorded, and the residual electrical noise was minimized to optimize the signal to noise ratio. The residual noise was displayed by the HEARLab® software using a traffic light indicator method. The color red appeared when residual noise voltage in the average waveform was >3.6 µV and green when the residual noise was <3.2 µV and orange when in between. Testing was paused if the residual noise was >3.6 µV and testing recommenced when the child had settled. Speech token stimuli were initially delivered at 65 dB SPL, and if no response was recorded, the presentation level was increased to 75 dB SPL. If a CAEP response was evident at 65 dB SPL, the presentation level was decreased to 55 dB SPL. This procedure was performed for each of the three speech stimuli for all the infants tested at both the initial unaided appointment and the subsequent CAEP hearing aid fitting evaluation. For each speech stimulus tested, a total of 150 artifact-free epochs were recorded from each child with an epoch of −200 to 600 ms (Munro et al., 2011). The decision-making criterion for determining the presence of the cortical response was made objectively by the HEARLab® using the Hotelling’s T2 statistical method (Chang et al., 2012; Flury & Riedwyl, 1988). The Hotelling’s T2 statistical analysis divides each accepted response into nine 50 ms time bins starting from 101 ms. All the samples within each bin are averaged to produce a single value, and the Hotelling’s T2 calculation determines if the response is significantly different from noise, that is, that an evoked response is present (significance level set at alpha = 0.05 for rejecting the null hypothesis that the amplitude of the response and noise are not different).
The Clinical Implementation of the CAEP Tests
The initial unaided CAEP measurement appointment lasted between 90 and 120 min. The CAEPs were explained as for all tests and measurements, and the parents observed the CAEP responses to the speech sounds. Following unaided CAEP recordings, early aiding was not recommended for children with a PCHI who had CAEPs responses at 55 dB SPL for speech tokens /g/ and /t/. Early hearing aid fitting was recommended if there was an absent response for /g/ or /t/ at 55 dB SPL if this was consistent with the diagnostic ABR/ASSR assessment. Although responses to /m/ were recorded and considered alongside the /g/ and /t/ speech tokens, the absence of an isolated response confined to the /m/ speech token did not prompt a recommendation for early hearing aid fitting. Van Dun et al. (2012) reported a lower detection sensitivity for the /m/ speech token with a sensitivity of 63% at a 20 dB SL, and the early aiding in infancy of isolated low-frequency PCHI was not considered clinically necessary. All the children, for whom early hearing aid fitting was not recommended, were subsequently followed up with further assessment of their PCHI by behavioral testing. This prompted the audiologists to counsel parents when speech needed to be amplified and a hearing aid fitting appointment was made. If parents agreed to this, a hearing aid was fitted. A second CAEP assessment was undertaken 4 to 8 weeks after the hearing aid fitting to assess the benefit of the amplification for speech sound detection to the parents. When the CAEP was absent at 75 dB SPL in children optimally fitted with hearing aids, and if there were no contraindications, referral for CI assessment was recommended.
Hearing Aid Fitting
Throughout the study period, hearing aids were fitted following recommendations from the NHSP guidelines (British Society of Audiology, 2007; Feirn et al., 2014). The department followed the required NHSP protocol which was to use ABR to obtain two frequencies and added the additional procedure of using ASSR for the other two frequencies. ABR is a lengthy procedure compared to ASSR, and there is a time limitation in testing with infants. The ABR thresholds for 1000 and 4000 Hz and ASSR thresholds for 500 and 2000 Hz were used to predict hearing levels for each child. This combination gave four frequency thresholds for more accurate hearing aid fitting. Correction factors for both ASSR and ABR were applied according to the NHSP guidelines (Stevens et al., 2013). The estimated behavioral threshold values were entered into the Audioscan Verifit real ear measurement system (Audioscan, 2014). Target gain values were generated using the Desired Sensation Level (DSLv5) hearing aid prescription method (Scollie et al., 2010; Seewald, Moodie, Scollie, & Bagatto, 2005). Hearing aid outputs were verified using Real Ear Aided Response measures and individually corrected using Real-Ear-To-Coupler Difference or normative values for Real-Ear-To-Coupler Difference for a child of the same age. Hearing aid outputs for 55, 65, and 75 dB SPL speech input were adjusted to match prescription targets (Bagatto, Scollie, Seewald, Moodie, & Hoover, 2002; British Society of Audiology, 2007). The amplification was matched to targets within ±5 dB at frequencies of 500, 1000, and 2000 Hz, and of ±8 dB at 3000 and 4000 Hz, in accordance with the national guidelines.
Regularity of hearing aid use was recorded at postfitting assessments using the data logging facility in the hearing aids. For Cohort A, data logging was measured retrospectively from the fitting sessions at their first VRA appointment. For Cohort B, the data logging was recorded at the appointment after the CAEP hearing aid fitting evaluation but before the VRA assessment. The data logging represented the duration of aid use that was achieved following the CAEP evaluations and before behavioral assessments had reinforced the need for amplification.
Data Analysis
Demographic data were obtained from individual patient records and from the Easy Screening Programme to ensure that all eligible children diagnosed were included. Age at confirmation of PCHI, age at hearing aid fitting, and age at referral for CI assessment were recorded. Following the unaided CAEP assessment, decisions about the rehabilitative process were made through discussions between the audiologists and the parents. The children were categorized into one of the three decision groups (Figure 3).
Children who had an early hearing aid fitting (children fitted with hearing aids without any delay and at the appropriate age) undertaken as a result of the Children for whom hearing aid fitting was delayed as a result of the Children for whom hearing aid fitting was delayed as a result of The management pathway following the unaided CAEP recording. CAEP = cortical auditory evoked potential; MDT = multidisciplinary team; VRA = visual reinforcement audiometry.

Distribution of data for age at hearing device fitting violated the assumptions of normality (Shapiro–Wilk;
Results
The Age of Confirmation of PCHI
The 34 children in Cohort A had PCHI confirmed at a median age of 1.3 months (IQR = 0.9–2.6). The 44 children in Cohort B had PCHI confirmed at a median age of 0.9 months (IQR = 0.7–1.5). The median ages of confirmation of PCHI were not significantly different in the two cohorts (Mann–Whitney
The Unaided CAEP Recording
All 44 children in Cohort B had recording of unaided CAEP responses. Eight children had a second appointment because of illness or because they were not sufficiently settled for testing. They were seen for unaided CAEP recording at a median age of 3.5 months (IQR = 2.5–4.6) with a median delay of 8.8 weeks (IQR = 5.1–14.9) after diagnostic confirmation of PCHI.
The Age of Hearing Aid Fitting
Of the 34 children enrolled from Cohort A, 31 (91%) were fitted with hearing aids by the age of school entry. In Cohort B, 43 of the 44 children (97%) had been fitted with hearing aids by the time of this analysis. The single child who had not been fitted with hearing aids from Cohort B was aged 2.4 years at the time of the analysis. Figure 4 shows the median age of hearing aid fitting and the IQR for children in the two cohorts. By 52 weeks, 56% of children in Cohort A had been fitted with hearing aids compared to 90% from Cohort B. The outlier in Cohort A, number 23, was a child with a moderate PCHI whose parents chose to delay the use of hearing aids until the age of 53 months. There were five outliers in Cohort B. Outlier 40 was a child with an asymmetrical PCHI with a 70 dB HL high frequency loss at 4 kHz in his better hearing ear and 80 dB HL 4FAHL in his worse hearing ear. He was fitted at 25 months. Outlier 77 had a severe PCHI and was fitted at 23 months. Both children had been identified by the CAEP recording as requiring hearing aids but their parents chose to put off the fitting until a delay in their child’s speech and language prompted them to accept the audiologist’s recommendation for hearing aid fitting.
Box-and-whisker plots of age of hearing aid fitting for Cohort A (
Outliers numbered 35, 36, and 37 were children who had two or more CAEP responses at 55 dB SPL. The initial audiologist recommendation at the unaided CAEP recording for each of these children was to continue monitoring their hearing but not to undertake hearing aid fitting in infancy and they were eventually fitted at 39, 42, and 46 months, respectively. All three children showed delay in their speech and language which was reported by the Teacher of the Deaf. The 39-month-old child was showing a delay of 13 months, and the other two children were showing a delay of 11 months. At this point, hearing aid fitting was advised to the family.
Median Age of Hearing Aid Fitting and IQR in the Two Cohorts by Degree of Hearing Loss.

Delays in the Fitting of Hearing Aids
PCHIs in Cohort A and Cohort B, Grouped by the Severity of the Hearing Impairment and Decision Group Categorization.

Those infants whose hearing aid fitting followed the audiologists’ recommendation were grouped together. They included those where the fitting was undertaken early in infancy and those where fitting was delayed because of the audiologists’ recommendation. In all, 22 of the 31 aided children (71%) in Cohort A were fitted as recommended by the audiologists. For nine children, hearing aids were fitted at an age determined by parental choice. In Cohort B, 37 of the 43 aided children (86%) were fitted in accordance with the audiologists’ recommendation with 6 children having hearing aids fitted at an age delayed by parental choice. The median and IQR for the age of hearing aid fitting as grouped by the reason for the delay and by cohort are presented in Figure 5. In Cohort A, the median age of hearing aid fitting by the audiologist’s recommendation was 4.6 months (IQR = 2.9–16.6 months). The median age of the children fitted by parental choice was 19.8 months (IQR = 14.0–37.1 months). In Cohort B, the median age of fitting with hearing aids by audiologist recommendation was 3.2 months (IQR = 2.0–4.6 months) and age at fitting by parental choice was 9.4 months (IQR = 7.7–22.1 months).
Box-and-whisker plots of those children with PCHI in Cohort A (left panel) and Cohort B (right panel), showing the age at which hearing aid fitting occurred based on the audiologists’ recommendation (Cohort A, 
A Comparison of Unaided and Aided CAEPs for Hearing Aid Fitting Evaluation and Hearing Aid Use
All 34 infants with hearing aid fitting following the unaided CAEP test attended for a repeat CAEP recording to evaluate the fitting. The median age of aided CAEP was 5.0 months (IQR = 3.9–6.2 months). This represented a median delay of 7.1 weeks from the unaided CAEP (IQR = 3.0–8.9 weeks). Twelve infants (35%) demonstrated an improvement of ≥10 dB in CAEP thresholds for all three speech tokens when wearing hearing aids, with 11 (32%) showing an improvement for two speech tokens, and 5 (15%) for a single token. No responses were recorded at 75 dB HL to any of the three tokens in six of the infants (18%) wearing functioning hearing aids with a high gain. This indicated that hearing aids were not providing sufficient amplification for sound to be audible at 75 dB HL suggesting that hearing levels were insufficient for good speech development. The aids may have provided information about environmental sounds at higher levels, but they were just inadequate for effective amplification of speech, so the infants were referred for CI.
For Cohort A, hearing aid usage demonstrated median usage of 4 hr 6 min each day and 22% of infants wearing the hearing aids for 7 hr and longer. Cohort B data logging demonstrated a median usage each day of 4 hr 25 min with 25% of the infants wearing the hearing aids for 7 hr 9 min or longer. This shows an improvement in duration of use from Cohort A to Cohort B (Mann–Whitney
Behavioral Audiological Assessments
Categorization of Hearing Impairment for Children With Mild or Moderate PCHI Based on Early Estimates From ABR/ASSR Thresholds and the Behavioral VRA Examination Undertaken at 6–8 Months.

The 18 infants with a mild or moderate PCHI in the early hearing aid fitting group had a median 4FAHL of 58 dB HL (
The Age of Referral for CI Assessment in Cases of Profound Hearing Loss
Median Age of Confirmation of Hearing Loss, Fitting of Hearing Aids, and Referral for CI Assessment in Cohort A and Cohort B.

The Aided and Unaided CAEP Responses in the Children Who Were Referred for Cochlear Implant.

Discussion
This study demonstrates a significant reduction in the age at hearing aid fitting in children with a PCHI following the inclusion of speech sound CAEP measurements within the audiology pathways. This analysis compared the age of hearing aid fitting in sequential cohorts before and after the CAEP assessment had been introduced. The median age of hearing aid fitting for children with all degrees of PCHI was reduced from 9.2 months in Cohort A to 3.9 months in Cohort B with a marked reduction from 19.0 to 5 months in those with a mild or moderate PCHI. In the earlier cohort (Cohort A), even though the presence of a mild or moderate PCHI had been confirmed by the neonatal diagnostic tests, the audiologist recommended delaying the hearing aid fitting for 40% of the infants until behavioral tests were available. However, for Cohort B, the recording of CAEP in response to short speech sounds enabled the audiologist to evaluate hearing detection for low-, mid-, and high-frequency speech sounds. In the later cohort, this resulted in a recommendation for hearing aid fitting in early infancy in 88% of children with mild or moderate hearing losses. The observation that CAEP responses to speech sounds were absent influenced the parents who were able to hear the stimuli themselves. The CAEP evaluation was used as an educative process, and the percentage of parents of infants with a mild or moderate PCHI who chose to defer hearing aid fitting fell from 40% to 19%. Even when they elected to wait, the delay in hearing aid fitting was reduced with the median fitting age of 26.9 months for Cohort A falling to 8.0 months for Cohort B. In 82% of cases, aided CAEPs demonstrated hearing benefit for detecting the speech tokens; this motivated the parents to support their child’s consistent use of hearing aids. As well as reducing the age of fitting of the hearing aids, hearing aid use average increased, where 25% of the infants were wearing the hearing aids for 7 hr or longer, in Cohort B. This compares favorably with median data logging of 3.7 hr in children aged 7 to 35 months reported by Muñoz, Preston, and Hicken (2014). These findings are similar to the children in Cohort A who showed hearing aid use on average of 4.6 hr each day. The absence of responses to short speech sounds of 75 dB SPL prompted further behavioral assessment and discussion about referral for CI assessment. The age of CI referrals reduced from a median age of 20.2 to 8.2 months from Cohort A to Cohort B, respectively.
The age at hearing aid fitting is recognized to be an important factor on the outcomes of children with hearing loss (Moeller, 2007). The early studies supporting the need for UNHS in the United States reported higher language scores when neonatal identification was accompanied by the early provision of hearing aids and enrollment into particular, well-developed intervention programs (Calderon & Naidu, 1999; Moeller, 2000; Yoshinaga-Itano & Sedey, 1999). A subsequent longitudinal study of children with mild to profound hearing loss reported by Sininger et al. (2010) reported that age at hearing aid fitting had the largest effect on auditory-based communication outcomes. Despite the importance of early fitting and consistent hearing aid use, this does not necessarily follow early identification.
Difficulties have been encountered when providing optimal hearing aid intervention for some populations. The New York State Universal Neonatal Hearing Screen Programme reported variation in the age at which children who were identified neonatally were fitted with hearing aids (Dalzell et al., 2000). The median age at diagnosis of PCHI was 3 months for the entire group of 85 infants, but only 36 were fitted with hearing aids, and this minority was fitted at a median age of 7.5 months. The challenges encountered were delays in obtaining parental agreement for early intervention, noncompliant parents, milder hearing losses, and audiologist uncertainty that amplification was required. The difficulties encountered in New York mirrored the findings from an earlier cohort in East London. Watkin et al. (1990) reported that because children with a mild-to-moderate hearing loss responded to broadband environmental sounds, parents often found it difficult to recognize the impact of a hearing impairment by observing behaviors in the home. Unsurprisingly, if the effect of hearing loss is not apparent, the motivation for parents to use hearing aids is lower. Sjoblad, Harrison, Roush, and McWilliam (2001) found that 65% of parents questioned hearing aid benefit and 30% of them emphasized the need for better education on hearing aid use. The value of providing hearing aids is reliant upon parents understanding how hearing aids can benefit their child (Ching et al., 2013; Muñoz et al., 2014). In the reported cohorts, the inclusion of CAEP recording in the clinical pathways offered a novel opportunity to inform parents. CAEP testing facilitated discussion about the hearing impairment and the benefit of hearing aids in a pragmatic and audio–visual, heuristic manner.
The educative value of CAEP was recognized by the introduction of HEARLab® into the Australian Hearing infant clinical pathways in 2011 (Punch et al., 2016). There were some initial concerns about the routine introduction of CAEP recording because sensitivity studies had demonstrated that in around 25% of cases CAEP responses were not detectable even when the sounds were audible. This reinforced the need to interpret results across a test battery within the infant pathways. The CAEP-aided assessment within 8 weeks of the initial hearing aid fit was used to check or guide modifications of the fitting or to confirm that despite optimal aiding, hearing responses to speech presentations were absent. The absence of recordable responses helped parents and professionals to consider the need for CI evaluation including children with ANSD. Our study adds evidence that CAEP can be a useful assessment and counselling tool both to reinforce the need for aiding and when no responses are observed, to consider the need for progressing to CI assessment.
Despite the concerns that absent CAEP responses may not always signal inaudibility of sound, no infant for whom hearing aid fitting was recommended was found at the later behavioural tests to have been incorrectly aided. It is important to note that CAEP alone was not used, and ABR/ASSR assessment was used to derive hearing thresholds. In cases where absence of responses to speech tokens at 55 dB SPL had prompted the audiologist to recommend early aiding, average hearing thresholds were 58 dB HL. In cases where the audiologist recommended delaying the fitting because unaided CAEP responses were present at 55 dB SPL, the median hearing levels were 41 dB HL compared to a median of 55 dB HL in the group where aiding was recommended, suggesting that greater uncertainty was present for infants with lower levels of hearing impairment. CAEP responses at 55 dB SPL speech sound may have a 10 dB SL when the hearing threshold is 45 dB HL and therefore predictably those with an average hearing loss of 41 dB HL would have shown responses to speech tokens of 55 dB SPL, and those with a loss of 58 dB HL would not (Punch et al., 2016). Those with an average loss of 41 dB HL did eventually require hearing aid fitting, and it is important that the presence of unaided CAEP responses in infancy does not offer false reassurance that hearing aid fitting will not be required during the preschool period. However, for the majority of infants, the introduction of unaided CAEP assessment had offered additional information both to the audiologist and to the parents for audibility of short speech sounds and the benefit of using hearing aids. This presented an opportunity for counselling the parents which was considered pivotal in the marked reduction in the age when hearing aids were fitted to those children who were identified neonatally and who had anything less than a severe PCHI.
Limitations of the Study
In this study, one of the cohorts was historical, and this poses inherent problems. Changing attitudes of audiologists, the hearing support team, and the parents over the period of the study may have been a contributory factor in reducing the age at hearing aid fitting. In the United Kingdom, Cross (2011) looked at trends in the age of referral for CI between 2001 and 2010 which had significantly decreased over this period. However, although a culture of earlier referral for CI evaluation had been nationally fostered, the CAEP test provided a clinical rationale to support both parents and audiologists in the need to make such referrals. Such changing attitudes had also influenced the age at hearing aid fitting following the establishment in England of the NHSP. Wood, Sutton, and Davis (2015) reported this national trend in children with moderate and worse hearing impairment, and this is likely to have contributed to the reduction in age at hearing aid fitting found in the current study. Nonetheless, the staff and clinical facility had remained constant over the period reported, and the single major difference in the clinical pathways between the two sequential cohorts had been the introduction of the CAEP recording. The CAEP test had provided a means of demonstrating the clinical need for hearing aid fitting to both parents and audiologists, and it was considered a significant factor especially in those with milder impairments. Unfortunately, there is the potential for missing mild hearing losses which cannot be addressed through testing in the free field. In order to assess levels below 55 dB SPL, insert earphones or similar are necessary; however, this would not allow comparison between aided and unaided measures. The use of sequential cohorts imposed some limitations on follow-up. The early cohort consisted of children born between January 2008 and August 2011, and it was followed up until all the children had entered primary school. The later cohort consisted of children born between September 2011 and April 2015, and at the time of analysis, one child remained unaided and had not reached primary school age so had the potential to still receive a hearing aid; however, this one child had a minimal effect on the findings. The moderate sample size, single center, and narrow demographics represented in the sample limit generalizability of the findings. However, optimizing hearing aid management is the foundation for improving auditory-based communication, and use of CAEP recording can provide information about speech sound detection and the benefit of hearing aid use encouraging timely parental engagement. The reason for this will be further explored with the families via questionnaires and focus groups (Mehta, Marriage, Mahon, & Vickers, 2017).
Conclusion
This study has shown that CAEP recording has the potential to be an important tool for inclusion in the clinical pathways for infants with a confirmed PCHI. In a comparison between two consecutive cohorts, where the difference was that the latter followed an audiological pathway containing CAEP recording, it was shown that the cohort receiving CAEP testing had a lower age of hearing aid fitting. Interestingly, the most dramatic difference was observed for infants with mild or moderate hearing losses. It is postulated that this occurred because the CAEP is an educative tool for parents to understand their child’s hearing impairment and for audiologists to have an additional objective tool to increase confidence in their assessments. This study also indicated an earlier age at referral for cochlear implantation for those in the group receiving CAEP testing; however, this is in line with the national trend. Further research is required to assess the speech and language outcomes of the children receiving hearing aids at a younger age. Also, further evidence is needed to evaluate the theories that CAEP testing within the audiological pathway influences parental and audiological decisions about infant hearing aid provision.