
Abstract
Introduction
Down syndrome (DS) and fragile X syndrome (FXS) are two genetic disorders with overlapping behavioral phenotypes including intellectual disability and communication impairments (Bax & Gillberg, 2010; Rogers, Wehner, & Hagerman, 2001). Despite the overlap, individuals with DS and FXS demonstrate differences in their communicative abilities, including differences in social communication (Abbeduto et al., 2006; Finestack, Sterling, & Abbeduto, 2013; Roberts et al., 2007). Nevertheless, studies have reported that both DS and FXS have an increased rate of autism spectrum disorder (ASD) compared to the general population (Cohen et al., 2005; DiGuiseppi et al., 2010; Levy et al., 2010). Although, several studies have identified ASD symptoms in children with DS and FXS, it is unclear what additional impact these symptoms have on communication, and more specifically, on gesture use. Gestures are a particularly meaningful area to examine in individuals with ASD symptoms since gesture use is a significant weakness in ASD (Mastrogiuseppe, Capirci, Cuva, & Venuti, 2015; So, Wong, Lui, & Yip, 2014), but a strength in DS (Caselli, Monaco, Trasciani, & Vicari, 2008; Iverson, Longobardi, & Caselli, 2003; Stefanini, Caselli, & Volterra, 2007). To date, few studies have investigated gesture use in FXS (Flenthrope & Brady, 2010; Marschik et al., 2014; Roberts, Mirrett, Anderson, Burchinal, & Neebe, 2002). Comparing individuals with DS and FXS allows for in depth investigations into the extent to which ASD symptoms uniquely influence these genetic disorders. Given the dichotomy in communication skills in DS and ASD, and the scarcity of research on this topic in FXS, this study focused on gesture use in individuals with DS and FXS and examined the impact of ASD symptoms on this aspect of communication.
Communication and gesture use in ASD, DS, and FXS
Gestures are one of the first forms of communication in a child’s life and support language development (Capirci & Volterra, 2008; Luyster, Kadlec, Carter, & Tager-Flusberg 2008; McDuffie, Yoder, & Stone, 2005). Within the first year of life, children with typical development (TD) use gestures to regulate behavior, interact socially, and initiate joint attention (Shumway & Wetherby, 2009). The development of gestures is important because gestures predict language development in children with TD (Capone & McGregor, 2004; Goldin-Meadow, 2015). Gestures not only predict the occurrence of first words, but also word combinations and vocabulary size. Gestures are critical for early communication as well as functional communication throughout development, particularly in the case of children with expressive language deficits, such as for children with ASD, FXS, or DS.
Autism spectrum disorder
ASD is a pervasive neurodevelopmental disorder characterized by deficits in social communication and interaction as well as restricted and repetitive behaviors and interests (American Psychiatric Association, 2013). Deficits impact communication, not just in terms of social reciprocity, but also eye contact, facial expressions, and both the use and comprehension of gestures (American Psychiatric Association, 2013). Previous research has shown deficits in quantity and quality of gesturing among preschool and older children with ASD (Mastrogiuseppe et al., 2015; Shumway & Wetherby, 2009). Quantitatively, both younger and older children with ASD gesture less often than children with TD and children with other developmental disabilities, including DS (Bartak, Rutter, & Cox, 1975; Mastrogiuseppe et al., 2015; Shumway & Wetherby, 2009; So, Lui, Wong, & Sit, 2015). Qualitatively, children with ASD show different patterns of gesturing compared to TD peers. Specifically, children with ASD use gestures primarily to regulate behavior rather than for the purpose of joint attention (Bean Ellawadi & Ellis Weismer, 2014; Loveland & Landry, 1986; Maljaars, Noens, Jansen, Scholte, & van Berckelaer-Onnes, 2011). This body of research consistently shows that children with ASD are not using gestures to communicate for social means or to initiate joint attention, but rather for the purpose of requesting and meeting their own needs. Investigation into gesture use is important given that gesture use predicts both receptive and expressive language abilities in children with ASD (Luyster et al., 2008; McDuffie et al., 2005). The research on gesture use in ASD has primarily focused on children with idiopathic ASD, therefore excluding those with syndromic ASD.
Down syndrome
DS is the most common chromosomal cause of intellectual disability, occurring at a rate of one in every 691 live births (Parker et al., 2010). Beyond cognitive deficits, individuals with DS demonstrate lifelong deficits in communication (Martin, Klusek, Estigarribia, & Roberts, 2009). Children with DS have historically shown a relative strength in nonverbal communication over and above other aspects of communication (Caselli et al., 2008; Iverson et al., 2003; Stefanini et al., 2007). When matched to children with TD based on overall language ability, children with DS use gestures and produce gesture–word combinations at comparable rates, although their skills fall behind TD peers in terms of producing two-word combinations (Iverson et al., 2003). Another study reported a “gesture advantage” in children with DS between the ages of 10 and 49 months compared to TD peers matched on word comprehension (Caselli et al., 1998). Specifically, the authors found that the children with DS had significantly better word comprehension compared to production and their use of gestures was commensurate with their word comprehension abilities. Despite the identified strength in gesture use, it is important to note that social gestures in particular may be a relative strength, whereas requesting gestures, or gestures used to regulate behavior, are not necessarily a strength in DS (Fidler, Philofsky, Hepburn, & Rogers, 2005). Nevertheless, the asynchronous pattern of development between gestures and expressive language is a unique clinical feature of this population.
Historically, researchers believed that children with idiopathic ASD and children with DS had distinctly different communicative strengths and weaknesses and the co-diagnosis was rare (Attwood, Frith, & Hermelin, 1988; Gibbs & Thorpe, 1983). However, recent studies have estimated rates of ASD in children with DS ranging from 5% to 39%, with the majority of studies reporting rates between 5% and 20%, which is significantly higher than the general population (for a review see Moss & Howlin, 2009). It is unclear whether the presence of ASD symptoms has a significant impact on gesture use, given that studies either exclude children with a co-diagnosis (Caselli et al., 1998; Fidler et al., 2005), or do not report the presence or absence of ASD symptoms (Caselli et al., 2008; Iverson et al., 2003; Wright, Kaiser, Reikowsky, & Roberts, 2013). The only study to date to address gesture use in children with DS and ASD is a study by Hepburn et al. (2008), which included case descriptions of two young children with DS and ASD. The study investigated children with DS between 24 and 45 months of age and the authors reported that neither child with DS and an ASD co-diagnosis used any gestures during the Autism Diagnostic Observation Schedule – Generic (ADOS-G; Lord, Rutter, DiLavore, & Risi, 1999). The study by Hepburn et al. (2008) provides preliminary information that gesture use may be an area of weakness for children with DS and a co-diagnosis of ASD.
Beyond gesture use, individuals with DS are often characterized as having relative strengths in social communication, whereas social communication is a core deficit in ASD. Despite this difference, studies have found variability in social communication in DS, particularly for children with DS and ASD (DiGuiseppi et al., 2010; Dressler, Perelli, Bozza, & Bargagna, 2011). While children with DS and ASD often have more severe intellectual disability compared to children with DS without ASD (Capone, Grados, Kaufmann, Bernad-Ripoll, & Jewell, 2005), one study found that when controlling for IQ, children with DS and ASD continued to have significantly lower scores on measures of social interaction, expressive language, receptive language, and restricted, repetitive and stereotyped behaviors compared to their peers with DS-only (Molloy et al., 2009). Therefore, intellectual disability does not appear to fully explain the presence of ASD symptoms in this syndrome. Understanding the contributions and overlap of intellectual ability, genetics, and ASD symptoms on functioning continues to be a critical area of research in DS as well as other intellectual and developmental disabilities.
Fragile X syndrome
FXS is the most common inherited cause of intellectual disability, occurring in approximately one in 3,600 males and one in 8,000 females (Kooy, Willemsen, & Oostra, 2000; Turner, Webb, Wake, & Robinson, 1996). FXS occurs when there are 200 or more CGG repeats on the
While FXS is the most common known single gene cause of ASD, males and females have different estimated rates of co-diagnoses (Hagerman, Hoem, & Hagerman, 2010). Recent estimates of rates of ASD in males with FXS using the ADOS and ADI-R in combination range from 27% to 81% (Clifford et al., 2007; Hall et al., 2008; McDuffie et al., 2012; Rogers et al., 2001). In females, studies report rates from 11% to 45% (Hall et al., 2008; Klusek et al., 2014; Wheeler et al., 2015). FXS and ASD share a similar behavioral phenotype, characterized by eye gaze avoidance, repetitive behaviors, and difficulty with change (American Psychiatric Association, 2013; Budimirovic & Kaufmann, 2011; Hagerman, 2002). There is currently a debate in the literature about whether ASD in FXS represents “true ASD” (Abbeduto, McDuffie, & Thurman, 2014; Hernandez et al., 2009). Abbeduto et al. (2014) argue that the presence of a more severe intellectual disability results in increased symptoms of ASD, and in some studies is closely related to the degree of ASD severity (Hatton et al., 2006; Kover, Pierpont, Kim, Brown, & Abbeduto, 2013). Others have argued that FXS and ASD are two separate disorders and when co-occurring have an additive and unique impact on development (Bailey et al., 2001; Hernandez et al., 2009). If FXS and ASD are unique disorders, then communication, including gesture use, may present differently in FXS based on the severity of ASD symptoms. On the other hand, gesture use may not vary based on ASD severity given the phenotypic overlap in FXS and ASD.
To our knowledge, three studies have examined gesture use in children with FXS (Flenthrope & Brady, 2010; Marschik et al., 2014; Roberts et al., 2002). One study included boys with FXS-only between ages 21 and 77 months, and found that gesture use was a relative weakness compared to verbal and vocal communication abilities based on the Communication and Symbolic Behavior Scales (Roberts et al., 2002). A retrospective study using seven family videos with both male and female children with FXS between nine and 12 months found that only one of the seven children used any gestures in the videos (Marschik et al., 2014). Only one study to date has examined gesture use in FXS taking into account ASD symptoms (Flenthrope & Brady, 2010). This longitudinal study by Flenthrope and Brady (2010) included 25 children with FXS between ages two and five. They grouped the participants based on high (>30;
Comparing DS and FXS
The similarities (i.e., intellectual disability and language impairment) and differences (i.e., social communication) in DS and FXS have led to comparative studies between the two syndromes (Abbeduto et al., 2006; Finestack et al., 2013; Roberts et al., 2007). Examining gesture use in this way is particularly useful given that gestures are a relative strength compared to expressive language ability in DS, yet a relative weakness compared to expressive language skills in FXS. Investigating gesture purpose over and above the quantity of gestures produced is important given that social communication is an area of deficit in FXS but a relative strength in DS (Martin et al., 2009; Roberts et al., 2007). Identified deficits in social communication in FXS, such as in perseverative language (Belser & Sudhalter, 2001) and eye gaze avoidance (Budimirovic et al., 2006), may extend to gesture use. Comparing individuals with DS and FXS within the context of ASD symptoms provides insight into how ASD symptoms uniquely influence these genetic disorders and the impact that ASD symptoms have on gesture use. Taking ASD symptoms into account when evaluating communication skills in individuals with DS or FXS is important not only in terms of clinical implications but also from a theoretical perspective. Examining phenotypes provides a way to investigate the genetic influence of DS or FXS as well as the unique contribution of ASD. The comparison of these two syndromes sheds light on what characteristics are syndrome specific or more broadly characterize individuals with intellectual and developmental disabilities.
Purpose of the present study
Gestures are a critical aspect of early communication and lay the foundation for later word learning (Capirci & Volterra, 2008; Luyster et al., 2008; McDuffie et al., 2005). Children with DS tend to demonstrate a gesture advantage over spoken language. Limited research in FXS has shown that gesture use may be impaired. However, no quantitative research exists on the impact of ASD on gestures in DS, and the studies in FXS have been restricted to very young children. Both groups of children struggle with expressive language beyond the early years making this question important in older children and adolescents (Finestack et al., 2013). Given the significant deficits in both gesture quantity and quality in children with ASD, it is important to extend this work to populations like DS and FXS, two syndromes with relatively high estimated rates of co-occurring ASD. Studying the impact of ASD symptoms on gesture use in DS is of particular interest given the dichotomy in gesture ability in DS compared to ASD (Caselli et al., 2008; Iverson et al., 2003; Mastrogiuseppe et al., 2015; Shumway & Wetherby, 2009; Stefanini et al., 2007). We addressed the following questions.
Quantitative differences
Are there quantitative differences in gesture use between individuals with DS and FXS? Are there within syndrome differences in quantity based on ASD severity? Qualitative differences
Are there qualitative differences in gesture use in individuals with DS and FXS? Are there within syndrome differences in quality based on ASD severity?
We hypothesized that the participants with DS would gesture more overall and produce a larger proportion of gestures for joint attention/social interaction compared to the group with FXS. We based this hypothesis on the strength in the use of social gestures in DS noted in the literature, and the limited research on FXS. We hypothesized that an increase in ASD symptom severity would negatively impact gesture quantity and quality in both DS and FXS. More specifically, we hypothesized that in both DS and FXS, ASD severity would be significantly and negatively related to gesture rate, and that individuals with more ASD symptoms would also produce a larger proportion of gestures to regulate behavior compared to those with fewer ASD symptoms.
Methods
Participants
Participant characteristics.
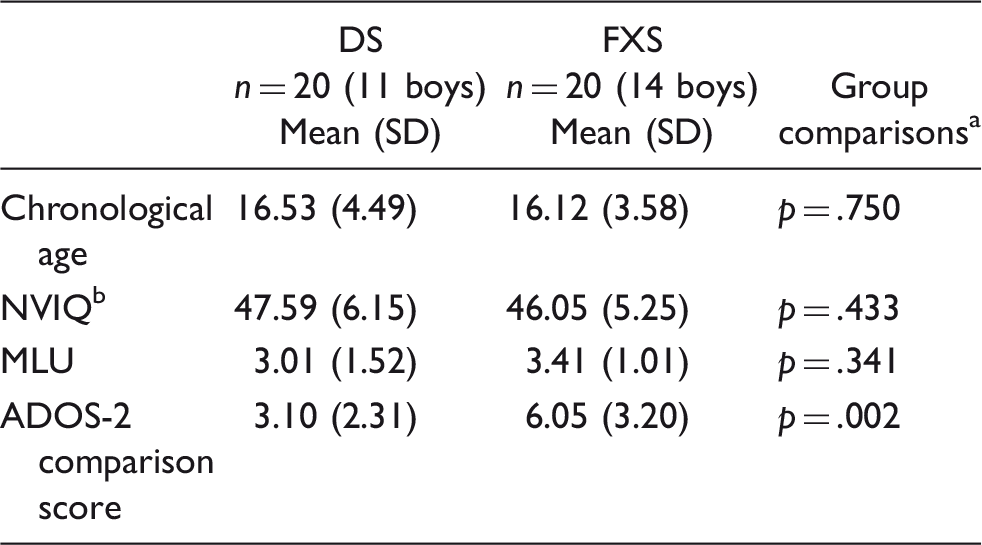
ADOS-2: Autism Diagnostic Observation Schedule – Second Edition; DS: Down syndrome; FXS: fragile X syndrome; MLU: mean length of utterance.
Independent sample
NVIQ measured from the Stanford-Binet Intelligence Scales –Fifth Edition (SB-V).
Group matching
Participants were matched at the group level on chronological age,
Procedure
The university’s institutional review board approved the study protocol. Written parental or legal guardian consent was obtained for each participant prior to testing. Each child also provided verbal and/or written assent. The visit consisted of a one-day assessment at the Waisman Center in Madison, Wisconsin. Participants completed cognitive and language assessments as well as an ASD assessment. Participants were offered breaks as needed.
Study measures
Nonverbal IQ
The Stanford-Binet Intelligence Scales – Fifth Edition (SB-V) was used to measure nonverbal IQ scores (Roid, 2003). The SB-V provides a standard score with a mean of 100 and standard deviation of 15. Reliability for the nonverbal IQ portion of the SB-V is considered excellent at .95. Validity based off of correlations with other tests of cognitive ability is also high.
Expressive language measure
Each participant also completed a 10-minute conversation language sample with a trained examiner using a standard set of prompts including open-ended questions about interests, school, family, vacation, pets, and sports (Berry-Kravis et al., 2013). Trained research assistants transcribed the audio files using the Systematic Analysis of Language Transcripts (SALT) software conventions (Miller & Iglesias, 2012). We obtained values for the mean length of utterance (MLU) for each participant (see Table 1).
ASD assessment
The ADOS-2 (Lord, Rutter, Risi, Gotham, & Bishop, 2012) was used to determine ASD severity using the ADOS-2 comparison score. The ADOS-2 examiner was either research reliable or training for research reliability with a research reliable examiner present for live scoring and coding. The ADOS-2 has been used in studies on children with FXS, DS, and idiopathic ASD to evaluate symptoms and determine ASD status (Hall et al., 2008; Martin et al., 2013; Price et al., 2008; So et al., 2015). The participants in this study completed either module 2 (Phrase Speech) or module 3 (Fluent Speech), depending on their language ability. According to the manual, interrater reliability for module 2 and module 3 is .96 and .94, respectively. ADOS-2 algorithm sensitivity for module 2 and module 3 is 94% and 82%, respectively (Lord et al., 2012). Specificity for module 2 is 100% and for module 3 is 92% (Lord et al., 2012).
Gesture coding
Description of the gesture coding.
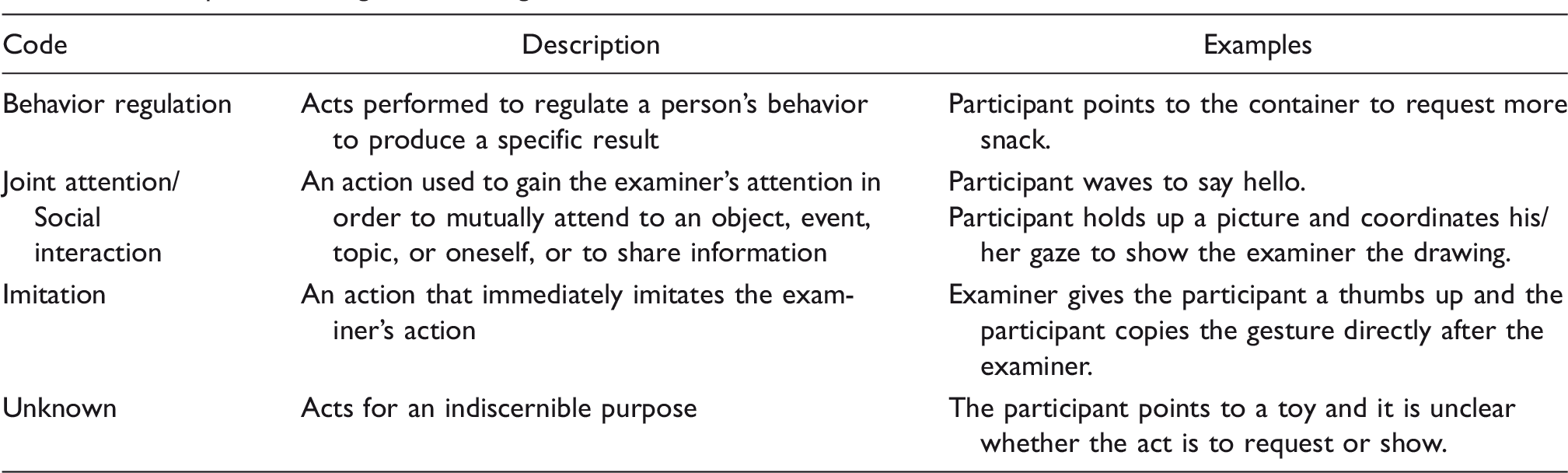
Note: Coding was adapted from multiple studies (Esplund, 2015; Flenthrope & Brady, 2010; Iverson et al., 2003).
For this study, we investigated quantity and quality of gesture use. Gesture quantity was defined by rate, or the number of gestures produced per minute. We used gesture rate to address research question 1 rather than the total number of gestures produced to account for time differences in the length of the ADOS-2. Quality included the purpose the gesture served, such as whether a gesture was used to regulate behavior or initiate joint attention/engage in social interaction. These are commonly studied metrics in children with typical and atypical development (Iverson et al., 2003; Mastrogiuseppe et al., 2015; Shumway & Wetherby, 2009). Gesture purpose (i.e., research question 2) was measured using proportions by taking the number of gestures for each purpose and dividing by the total number of gestures produced. Because the first research question focused on the quantity of gestures as measured by gesture rate, we used proportions to look at gesture purpose in the second research question to better understand the qualitative aspect of gesture use separate from the quantitative aspect. The use of a frequency measure (i.e., rate) and subsequent proportions or percentages to explore the quality of gestures is also consistent with previous work (Mastrogiuseppe et al., 2015). The use of proportions to compare qualitative gesture use between groups was previously used in two studies on gestures in children with DS (Iverson, Capirci, & Caselli, 1994; Stefanini et al., 2007).
Reliability
Two student coders independently completed all of the coding. Both coders were blind to participant diagnosis. Prior to coding participant files from the present study, coders reached a training criterion of at least 80% agreement on three different samples for both quantity and quality measures. Once criterion was met, the coders were randomly assigned ADOS-2 administrations to code (i.e., each coder independently completed approximately 50% of the files). Twenty percent of the videos were chosen at random and coded by a second coder independently to determine inter-rater reliability. Reliability was measured by calculating Cohen’s kappas. Cohen’s kappa for the total number of gestures was .91. Gestures coded as behavior regulation and joint attention/social interaction were .87 and .92, respectively. These values indicate near perfect agreement (Hallgren, 2012). Gestures coded as behavior regulation were less frequent, which likely contributed to the kappa value falling below .90. Therefore, two coders consensus coded all instances previously identified as behavior regulation for all 40 participants. During consensus coding, both coders agreed on whether the gesture purpose was behavior regulation or was instead an instance of joint attention/social interaction. After agreement, the proportions of gestures for each purpose were updated.
Data analysis plan
This study examined the differences in gesture use between participants with DS and FXS, as well as the impact of ASD symptoms on each syndrome. We did not include the imitation and unknown codes for gesture quality in the analyses since one percent or less of gestures received these codes. To analyze the data from this study, we utilized a general linear regression framework. All models included NVIQ as a covariate. We selected NVIQ given that the previous research on ASD in DS and FXS has argued that ASD severity is often closely related to intellectual ability (Abbeduto et al., 2014; Capone et al., 2005). Importantly, tests for multicollinearity were conducted between NVIQ and ASD severity and values were satisfactory for the group with DS,
Results
Research question 1: Quantitative differences
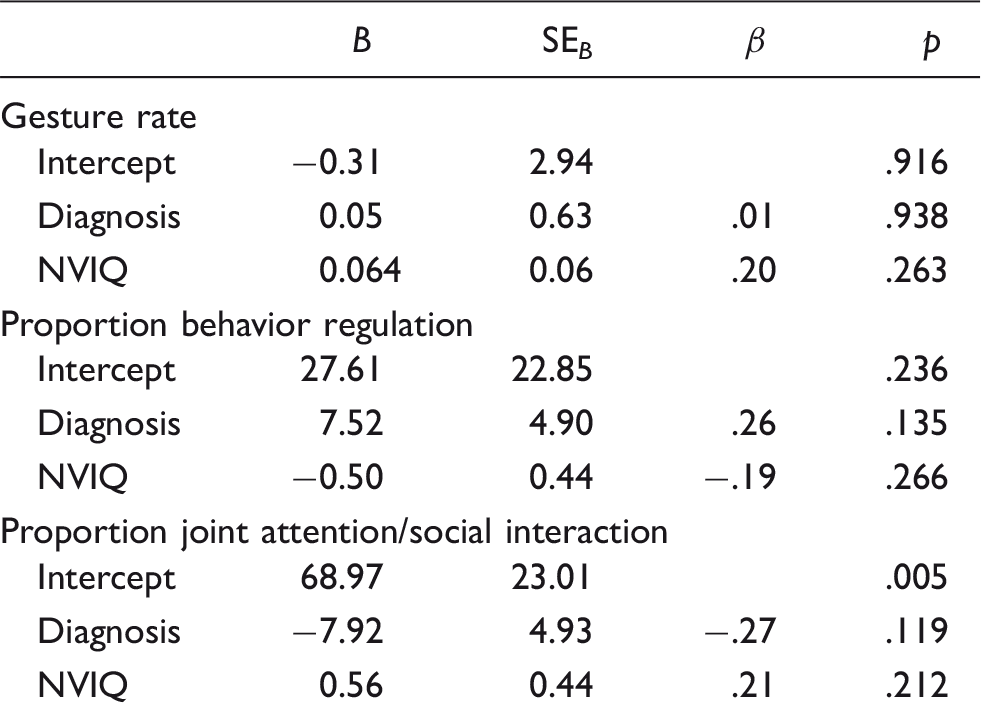
(1a) Between-syndrome analyses
Summary of the multiple regression analyses investigating group differences.
(1b) Within-syndrome analyses: DS
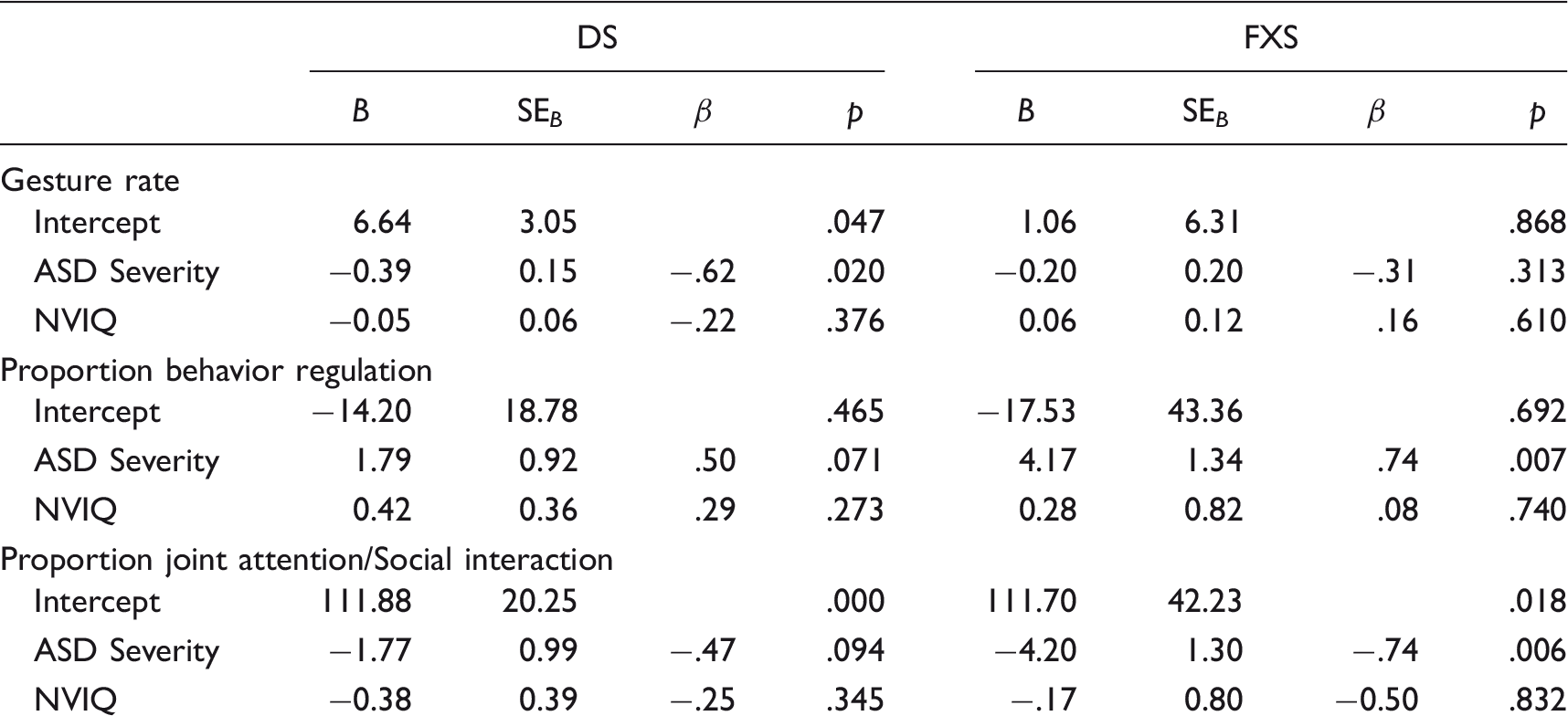
Summary of the multiple regression analyses predicting gesture rate and purpose in DS and FXS.
(1b) Within-syndrome analyses: FXS
The results of the multiple regression in FXS indicated that ASD symptom severity did not significantly predict gesture rate when controlling for NVIQ,
Research question 2: Qualitative differences
(2a) Between-syndrome analyses
The average proportion used for behavior regulation in the group with FXS was .21 (
(2b) Within-syndrome analyses: DS
Qualitative analyses were completed within DS based on ASD severity. The results of the multiple regression indicated that when controlling for NVIQ, ASD symptom severity did not significantly predict the proportion of gestures for behavior regulation,
(2b) Within-syndrome analyses: FXS
This study also examined the qualitative differences in gesture production in FXS based on ASD severity. NVIQ and ASD severity explained 48.2% of the total variance in the proportion of gestures used to regulate behavior,
Follow-up analyses included descriptive statistics to describe trends based on sex given the variability of the FXS phenotype in females as compared to males (Abbeduto et al., 2007). The average proportion of gestures used for behavior regulation for the females was .18 (
Discussion
Previous studies have identified gesture use as a strength in children with DS (Caselli et al., 1998; Iverson et al., 2003; Stefanini et al., 2007) and two studies found that gesture use was a relative weakness in children with FXS (Marschik et al., 2014; Roberts et al., 2002). However, the lack of information on the impact of ASD symptoms on gesture use in DS and FXS is a critical gap in the literature. Therefore, our study sought to provide information on this topic by examining the impact of ASD symptom severity on gesture quantity and quality in children and adolescents with DS and FXS. Overall, we found evidence suggesting no quantitative or qualitative differences in gesture use between the two genetic disorders. When examining gesture use in the individuals with DS, we found that as symptoms of ASD increased, individuals with DS gestured less often. Therefore, ASD symptom severity affects quantity but not quality of gesture use in DS. Further examination of gesture use in FXS showed that when ASD symptoms increased, individuals with FXS demonstrated qualitatively different gesture use with no significant changes in gesture rate. The significant effect of ASD symptom severity on gesture use in DS and FXS suggests important clinical considerations for individuals with DS or FXS demonstrating symptoms of ASD.
Research question 1: Quantitative differences
We examined quantitative differences between DS and FXS and the two groups did not significantly differ in gesture rate. This finding did not support our hypothesis but provided an additional similarity between two genetically distinct syndromes. The lack of differences may reflect how gestures develop beyond early childhood given that we based our hypothesis on research in younger children with DS and younger children with FXS. Perhaps gesture use develops as a tool that individuals with DS and FXS utilize later in childhood and extending to adolescence. No research to our knowledge describes how gesture use develops across the lifespan in DS or FXS. Alternatively, low power or the variability (i.e., relatively large standard deviations) within each genetic syndrome may have contributed to the null findings between groups.
In addition to the between group comparison, we were also interested in the impact of ASD symptoms on each group. As the children and adolescents with DS displayed more ASD symptoms, they gestured significantly less frequently than peers with fewer ASD symptoms. This finding mirrors preliminary qualitative findings of gesture deficits in young children with DS and ASD co-diagnoses (Hepburn et al., 2008). The differences found in this study of individuals with DS may be explained by the fact that children with DS typically have strengths in gesture use (Attwood et al., 1988; Caselli et al., 1998; Mastrogiuseppe et al., 2015), but ASD symptoms negatively influence quantitative gesture use to such an extent that it no longer functions as a strength. Although expressive language is an area of deficit in idiopathic ASD and DS, children with DS use gestures to compensate for language deficits while children with ASD do not (Mastrogiuseppe et al., 2015). In multiple studies, children with idiopathic ASD gestured significantly less than peers with other developmental disabilities (Shumway & Wetherby, 2009; Wetherby, Watt, Morgan, & Shumway, 2007). Therefore, social communication deficits in ASD seem to extend to gesture use. Since children with ASD have deficits in both expressive language and social communication, it is possible that this reduced frequency of gestures in DS found in individuals with more ASD symptoms, coupled with the underlying expressive language deficits, reflects a decreased motivation to use gestures or communicate.
In our study, the participants with FXS did not differ significantly in quantitative gesture use regardless of the degree of ASD symptoms. To our knowledge, only one study has provided preliminary information on quantitative gesture use in children with FXS (Marschik et al., 2014). However, the study by Marschik et al. (2014) did not include a comparison group or report the influence of ASD symptoms on gestures, but rather reported the presence or absence of gestures in seven young children with FXS. The two other studies on gesture use in FXS did not include quantitative measures of gesture use (Flenthrope & Brady, 2010; Roberts et al., 2002); therefore our study extends our understanding beyond qualitative gesture use as well as provides much needed knowledge on gesture use in older individuals with FXS. Additionally, the absence of significant differences may reflect that both FXS and idiopathic ASD present with deficits in gesture use; therefore, since quantitative gesture use would be similar between FXS and ASD, no quantitative differences would exist in individuals with FXS presenting with symptoms of ASD.
Research question 2: Qualitative differences
Overall, the children with DS and FXS were not significantly different on gesture purpose. These findings parallel the quantitative findings comparing the groups with DS and FXS. Thus, this overlap suggests that as a whole, older children and adolescents with DS and older children and adolescents with FXS are using the majority of gestures to engage in joint attention/social interaction rather than regulate behavior. Gesture use may be an area of growth in DS and FXS across childhood and into adulthood, particularly for children with FXS demonstrating few ASD symptoms, given the research showing gesture use as a relative weakness in young children with FXS (Roberts et al., 2002). Our findings may also reflect expressive and pragmatic language gains in individuals with DS and FXS which together give individuals the ability to communicate spoken messages for a range of functions outside of wants and needs, a skill not as well developed in young children with DS and FXS. It is important to continue tracking qualitative gesture use throughout the lifespan, as it might provide a tool to utilize during interventions when targeting social interactions and conversation skills.
When investigating within syndrome differences, the children with DS did not differ on qualitative gesture use based on ASD symptoms. Although Shumway and Wetherby (2009) did not include children with DS, our findings mirror their results. They found that the group with ASD did not significantly differ from the group with developmental delay in the use of gestures for behavior regulation and social interaction. Furthermore, our findings support previous work demonstrating that individuals with DS gesture more for joint attention and social interaction compared to requests (Fidler et al., 2005). This appears to hold true across individuals with DS regardless of ASD symptoms. Another possible explanation, although not specifically tested in this study, is that children with DS demonstrating more ASD symptoms overlap with both children with DS and children with idiopathic ASD but on different aspects of communication. Therefore, the children with DS displaying ASD symptoms may have a lesser degree of qualitative gesture deficits compared to the population with idiopathic ASD due to the influence of the DS phenotype. While no empirical data exists to support this explanation, previous research has found that children with DS and an ASD co-diagnosis sometimes perform more similarly to children with DS, such as on receptive language measures, while their behavioral profile is more in line with children with idiopathic ASD on measures of play and object use (Dressler et al., 2011). Even within gesture use, our results suggest that children with DS and more ASD symptoms are using gestures for the same purpose as their same age peers with DS and fewer ASD symptoms, but are overall using gestures less frequently. A next step would be to include a group with idiopathic ASD to determine if the participants with DS and ASD symptoms more closely mirror the group with DS or the group with idiopathic ASD regarding gesture purpose.
In this study, we found qualitative differences in the group with FXS based on ASD symptoms. Specifically, as the children with FXS presented with more ASD symptoms, they used a greater proportion of gestures for behavior regulation and a smaller proportion for joint attention/social interaction. These findings are consistent with the literature on idiopathic ASD, both with and without co-occurring intellectual disability, which found that children with idiopathic ASD use more gestures to regulate behavior than for joint attention compared to peers when matched on nonverbal mental age (Loveland & Landry, 1986; Maljaars et al., 2011). The fact that Shumway and Wetherby (2009) did not find the same differences in qualitative gesture use between individuals with ASD and individuals with developmental disabilities may indicate that both the specific syndrome and ASD severity play a role in qualitative gesture use. It is possible that some syndromes, such as FXS, show qualitative differences in gesture use when compared to children with ASD, whereas other syndromes may not show this difference. Specific group differences may not be captured when grouping together children with developmental disabilities resulting from different etiologies.
It is important to note that the groups with FXS included both males and females, and the females overall had fewer ASD symptoms. Although all the males and females with FXS in the current study had an intellectual disability, it is important to consider sex differences in studies including males and females with FXS. No studies to date have examined sex differences in gesture use in FXS. However, by including females in our sample, we are able to provide much-needed information on an understudied clinical group. We did not use inferential statistics to analyze females and males separately due to a lack of power. However, when looking at group means, we found the same trends in the female group as we did when examining the males. Based on descriptive statistics, gesture purpose does not seem to be distinctly different based on sex in individuals with FXS and intellectual disability. This study provides preliminary information on qualitative differences in FXS based on ASD symptoms, including both males and females, which may indicate that deficits in qualitative gesture use are specific to the ASD phenotype rather than FXS as a whole. Future studies should include individuals with broader verbal abilities and a group with idiopathic ASD to confirm these differences.
Clinical implications
Understanding what skills relate to gesture use may be key to identifying the underlying mechanism contributing to both learning and producing gestures. One skill that may contribute to gesture learning is visual–spatial ability. Previous research has identified gesture use and visual–spatial skills, in particular visual imitation, as a relative strength in DS (Fidler, 2005; Wang & Bellugi, 1994). Research on visual–spatial abilities in idiopathic ASD has mixed findings. While So et al. (2015) found visual–spatial abilities to be a relative strength on tasks of replicating specific actions, images or static tasks, other research has found a relative weakness on gestalt or dynamic visual–spatial tasks (Pellicano, Gibson, Maybery, Durkin, & Badcock, 2005). Additionally, children with idiopathic ASD have difficulty imitating gestures (Mostofsky et al., 2006) as well as imitating actions when objects are not used (McDuffie et al., 2005). While the visual imitation strength in DS has led to sign-based interventions for teaching receptive and expressive language, some children with DS do not make significant gains (Wright et al., 2013). The reduced rate of gesture use in the group with DS and increased ASD symptoms compared to those with DS and fewer ASD symptoms may indicate visual imitation deficits possibly associated with the deficits seen in idiopathic ASD. Therefore, it is possible that children with DS demonstrating ASD symptoms may not benefit from a traditional DS intervention involving sign language, although this is still unclear given that no literature exists on interventions for children with DS and ASD co-diagnoses.
Joint attention is another deficit in children with idiopathic ASD that is more specific to ASD rather than developmental disabilities in general (Maljaars et al., 2011). Understanding the joint attention skills of children with FXS and ASD co-diagnoses is important given that joint attention is a robust predictor of current and future language skills in idiopathic ASD (Luyster et al., 2008). Children with TD produce more gestures to initiate joint attention and fewer for behavior regulation whereas children with ASD display the opposite pattern (Maljaars et al., 2011; Shumway & Wetherby, 2009). A decrease in the initiation of joint attention, such as through the use of gestures, can reduce daily learning opportunities and chances for social engagement. Determining whether gesture use for joint attention/social interaction is a weakness in children with FXS and increased ASD symptoms is essential for identifying and addressing potential barriers to learning. Knowing how gesture production presents in individuals with FXS based on ASD symptoms is also clinically important for selecting goals, such as whether clinicians should target joint attention through gesture use or other modalities, such as eye gaze or speech.
Limitations and future directions
The present study added much-needed research on the different communication phenotypes in DS and FXS and how ASD symptoms can impact gesture use. However, the study did have several limitations. The sample did not fully represent the broad range of abilities in DS and FXS given that recruitment only included participants speaking in phrases, excluding children with minimal verbal abilities. This is an under-studied subgroup and represents an important future direction. We also did not control for sex and did not have the power to run analyses excluding females. However, including both males and females allowed for a better representation of DS and FXS. Previous research in DS did not find sex differences in gesture use (Fidler et al., 2005) but sex differences in FXS exist in other aspects of communication (Abbeduto et al., 2007). In addition to taking sex into account, including language ability as a covariate may help in determining the role of language ability in gesture use among these populations.
The sample size was small for the two groups. FXS is a relatively rare neurodevelopmental disorder, and therefore a sample size of 20 is in line with most published research (Finestack et al., 2013; Flenthrope & Brady, 2010; Roberts et al., 2007, 2002). However, our sample size restricted our ability to complete more sophisticated analyses and look more in depth at qualitative gesture use. In some of the analyses, significant findings were not detected, yet effect sizes were large, indicating the need for more power. We broadly characterized gesture rate and quality, but further investigation into specific gesture types (e.g., pointing) is warranted, especially given the dichotomy in the use of pointing gestures in DS and ASD. In addition, given our limited power, we were restricted to broad comparisons between DS and FXS. Future studies should also evaluate the differences between individuals with DS and FXS and ASD co-diagnoses to better understand the unique impact of ASD on each genetic disorder in greater depth. In addition, follow-up studies should investigate specific gesture types to better describe the gesture profiles of these populations.
Beyond gesture use, future research should investigate the visual-spatial skills of children with co-diagnoses. Previous studies have identified visual imitation as a relative strength in DS (Fidler, 2005; Wang & Bellugi, 1994). However, research on visual-spatial abilities in idiopathic ASD is mixed (Pellicano et al., 2005; So et al., 2015). We need to clearly understand visual-spatial skills and their connection to gestures to understand the mechanisms underlying gesture use. Additionally, very little is known about gesture comprehension. This study only focused on gesture production, so by including gesture comprehension, we can determine whether gesture deficits are specific to expressive communication or in conjunction with receptive deficits. It is also essential to understand other aspects of verbal and nonverbal communication in children with co-diagnoses, specifically the relationship among language, joint attention, and gesture use.
Conclusions
As we develop an understanding of the impact ASD symptoms have on DS and FXS, studies will be necessary to determine appropriate interventions for the different phenotypes. Since specific interventions exist for children with ASD, such as high intensity applied behavior analysis, it is essential to understand if children with DS demonstrating symptoms of ASD will benefit from this same type of intervention compared to naturalistic interventions typically used with children with DS, or whether a different, adapted intervention is most efficacious. Continuing to investigate the complex relationship between ASD and FXS, two syndromes with similar behavioral phenotypes, will help us understand the underlying causes and potential distinctions between the two disorders. Defining the characteristics of nonverbal communication and speech and language skills in individuals with DS or FXS and increased ASD symptoms is the first step to understanding these complex behavioral phenotypes, which is a necessary precursor to effective and efficient interventions.