
Abstract
Objective:
The objective of this study was to determine the elasticity of sternocleidomastoid muscle (SCM) in patients with congenital muscular torticollis (CMT).
Methods:
In all, 41 patients and 22 controls were included in the study, and the elasticity of the patients’ SCM was measured. Echogenicity, thickness, and strain values of the SCM were also obtained.
Results:
The thickness and strain values of the SCM were higher in the patient group than in the control group (
Conclusions:
The strain elastography technique can be used in the diagnosis of CMT.
Keywords
Congenital muscular torticollis (CMT) is a congenital muscle disease that causes contralateral rotation of the face and jaw as a result of asymmetric contraction and shortening of the sternocleidomastoid muscle (SCM). 1 Although the true cause of CMT is unknown, there are theories based on chronic recurrent micro-trauma such as muscle trauma at birth or prolonged poor fetal positioning. Endomysial fibrosis is considered pathologically, with collagen deposition and migration of fibroblasts around single muscle fibers. Although the abnormal and excessive proliferation of extracellular matrix (ECM) components is defined as muscle fibrosis, it causes loss of muscle function. The increased percentage of fibrous tissue in muscle fibrosis is quite similar to the contracture in SCM.
Restricted rotation of the neck with a palpable mass on the SCM is a characteristic sign. CMT can be divided into three groups: tumor-induced fibromatosis in the SCM, torticollis by tightening the SCM, and postural torticollis without the mass or tightness of the SCM. 2 The diagnosis of this condition is usually based on clinical findings and physical examination. Most of the cases recover without any treatment. However, surgical treatment is indicated in cases that do not improve until 1 year of age. The prevalence varies between 0.3% and 2.0%, and most of them are idiopathic.3,4
In addition to clinical findings, ultrasonography (USG) is the preferred imaging method in the diagnosis of torticollis. USG is the preferred method because it is inexpensive, easily available, and does not contain ionizing radiation. 5 Also, USG allows for a dynamic examination of the patient. Sonoelastography (SE) is an ultrasound technique that enables real-time evaluation of tissue flexibility. This technique is based on the principle that tissue compression creates less strain (displacement) in hard tissue than in soft tissue. Compression SE has recently been used to evaluate pathologic tissues affected by various muscle disorders and is a useful method for evaluating the stiffness of SCM. The SCM’s homogeneity, transverse and longitudinal length, and the presence of a possible mass or hematoma can be evaluated with gray-scale sonography.4,6 In SE, the elasticity of the muscle can be evaluated using an external force; however, with newer technologies such as shear wave elastography, no external force is required.7–10
Our aim of this study was to determine the possible benefits of SE findings in the diagnosis of torticollis by comparing with the literature. In addition, the study aim was to determine the diagnostic efficacy of strain elastography in evaluating patients with torticollis.
Materials and Methods
The findings of 50 infants who underwent USG for CMT, between May 2018 and March 2020, were evaluated retrospectively. Patients who were being followed as a result of CMT between May 2018 and March 2020 were evaluated retrospectively. The findings of 50 infants in total were examined. The inclusion criteria for the study were (1) congenitally palpable neck masses or limited neck movement, (2) obstructions in the rotational movements of the face and chin, and downward bending with movement, and (3) cases with normal neurologic examination. The cases excluded from the study are cases with retrospective lack of SE images, inadequate image quality, or cases with bilateral congenital torticollis. A total of 41 patients, meeting the criteria, were included in the study. There were cases of bilateral congenital torticollis in six of nine patients, and three patients did not achieve optimal quality. Therefore, they were excluded from the study. In addition, 22 healthy volunteers were included in the study as a control group. There was no restriction on neck movements in the patients in the healthy volunteer group. The study was approved by the local ethics committee of the hospital.
All USG examinations (elastography and gray-scale sonography) were performed by a single pediatric radiologist, with 5 years of clinical experience. He used a Hitachi ultrasound system (Hitachi Hi Vision, Stuttgart, Germany). The SE and USG were performed using a 6-16 MHz linear probe. Patients undergoing neck USG were placed on their back, and the contralateral side was evaluated after slight rotation of the head.
Both short-axis and long-axis images of the SCM were scanned for gray-scale examination. The purpose of the gray-scale sonographic examination of masses was to detect the presence of hematoma within the SCM. After the muscle images were obtained, an SE evaluation was performed. At this stage, the required external force was applied from outside. After applying the external force, the region of interest (ROI) box was placed to include the whole muscle to measure the SCM.
The SCM was also divided into three types according to the color scale. Regarding elasticity, soft/hard tissues demonstrated high elasticity. Correspondingly, medium hard tissues were represented mostly by green and a few small red areas, and medium elasticity textures were represented by green. The harder tissues were represented by blue. This color scale was used to understand the hardness of the tissues. These values were not used in the evaluation because they were measured subjectively. The colors represented the relative stiffness of the tissues in the ROI and ranged from red (soft, high elasticity) to blue (hard, low elasticity) in a continuous spectrum. After obtaining the ROI, the strain value was calculated.
In the USG evaluation, the echogenicity of the SCM was also evaluated and divided into the following groups: isoechoic, hypoechoic, or hyperechoic. The thickness and echogenicity of the SCM were also compared with the contralateral side. In addition, the difference in thickness between the pathologic and contralateral SCMs and the ratio between the corresponding and contralateral SCMs were calculated.
Statistical Analysis
The Mann–Whitney
Results
This study consisted of 41 patients. Within this cohort, 21 were male and 19 were female. The median age of the patients was 5 months (1–9 months). Eight patients had a preterm history of oligohydramniosis. As a control group, 22 healthy babies were included in the study. The median age of the control group was determined as 4 months. There was no difference between groups regarding median age (
Characteristics of the Study Population.

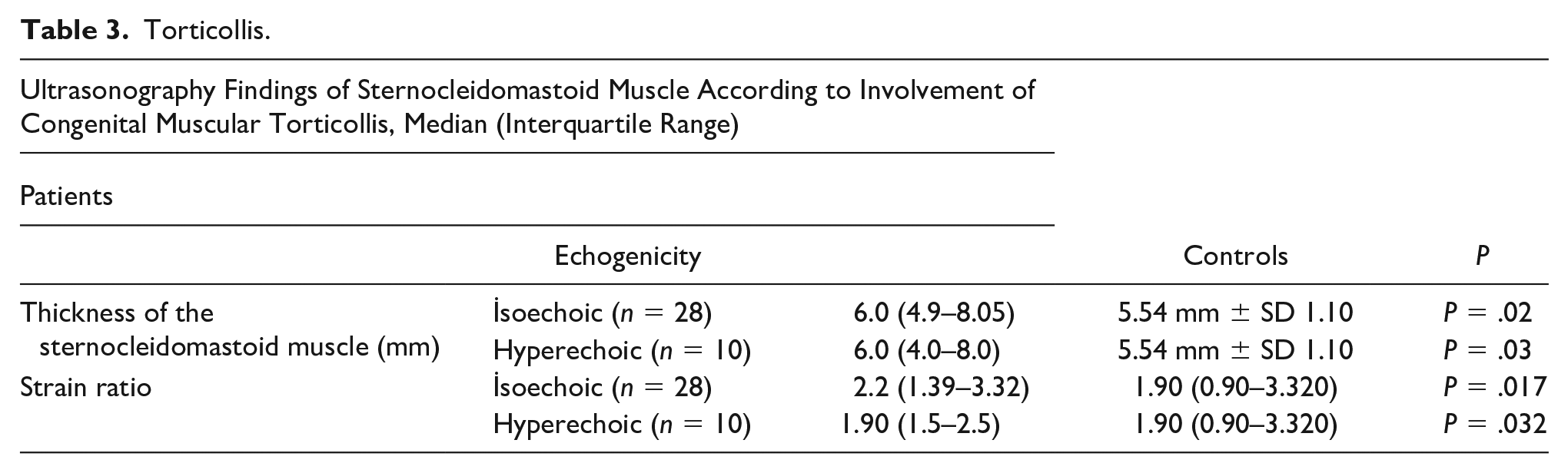
The echogenicity of SCM in 41 patients was as follows: isoechoic in 28, hyperechoic in 10, and heterogeneous in 3 patients. In the control group, isoechoic and homogeneous echogenicity were detected in all patients.
The SCM thickness was found to be higher in the patient group (6.26 mm ± SD 1.17) compared with the control group (5.54 mm ± SD 1.10) (
When comparing strain levels of SCM thickness, a significant difference was found between the patient group and the control group (
In this study, no significant difference was found in comparing the strain levels in the different echogenicity groups. Tables 2 and 3 show the strain values for different echogenic muscle groups.
Torticollis.

Torticollis.
In the strain elastography evaluation, the receiver operating curve (ROC) for muscle echogenicity in the isoechoic muscle group had a specificity and sensitivity of 100% and 22%, respectively, for the area under the curve (AOC) value of 0.558 (95% confidence interval [CI], 0.424–0.6686), and the cutoff value was <1.4. In the hyperechoic muscle group, the ROC for AUC values was 0.542 (95% CI, 0.411–0.6686) and had a cutoff value of >1.4. Again, there was 100% sensitivity and 20.75% specificity (see Figure 1A and B).

(A) The graph depicts the AUC for isoechoic muscle thickness. (B) The graph depicts the AUC for hyperechoic muscle thickness. AUC, area under the curve.
Discussion
The specific etiology of CMT is uncertain.3,11 Venous compression of the neck, fibrous hemorrhages in the peripartum period, and primary myopathy during the intrauterine period may have pathologic linkage. 12 Histologic examination of surgically resected materials has revealed atrophy and fibrosis in cases developed due to intrauterine venous compression.7,13
Cases of torticollis, which developed as a result of SCM spasm and thickening, usually resolve within the first year without treatment. SE is one of the accepted examination methods in the evaluation of tissue fibrosis. There are publications in the literature in which torticollis cases are evaluated by SE.1,10,11,14 This study has the potential to contribute to the evidence of strain elastography being conducted within this patient population.
SE techniques are used to evaluate tissue stiffness. 15 Although USG has been regarded as the gold standard for the diagnosis of CMT, its role seems to be limited to predict the prognosis of CMT. This may be due to the fact that the basic pathologic finding in CMT was muscular fibrosis, and this cannot be assessed using USG. In the strain elastography technique, tissue stiffness is measured by proportionating to a certain point of the muscle. In strain tissue elastography, the harder tissues have higher tissue stiffness.16,17 In this study, patients with torticollis have higher SCM elastography score than the control group. In summary, in patients with torticollis, the SCM was stiffer and harder to move due to increased muscle stiffness. The effect of SCM, in these torticollis cases, was similar to other studies in the literature.10,11,14
In this study, muscle echogenicity was found to be isoechoic in most of the recruited patients. Isoechoic patient cases were followed by hyperechoic example. Homogeneous and isoechoic echogenicity and decreased elasticity found in our study were due to the response of muscle to torticollis.
In this study, no significant difference was found between AUC values in comparison with isoechoic and hyperechoic muscle echogenicity. AUC values for both echogenicity groups are determined to be approximately 0.542 and 0.558, whereas the cutoff value of strain is determined to be 1.4.
This cutoff would help to diagnose CMT; however, larger cohorts and more robust studies are needed to raise the level of scientific evidence.
Limitations
This study has some limitations. The most important limitation of the study is its retrospective study design. In addition, there is a lack of understanding of the effects of treatment, since the patients who received treatment were excluded. Increasing the number of patients would increase the accuracy of the results.
Conclusion
Strain elastography is a noninvasive diagnostic method that could be used in the assessment of torticollis in pediatric patients. There is a need for more robust studies to further advance the use of SE for this specific clinical indication.