
Abstract
Introduction
The anterior cruciate ligament (ACL) is the major intra-articular ligament of the knee; it is also the most commonly injured knee ligament. Each year in the United States there are between 100,000 and 250,000 ACL injuries, or 1 in 3,000 in the general population; approximately 50,000 ligament reconstructions are performed annually.1–3 The purpose of this ligament is to support and strengthen the knee while preventing extreme translation of the tibia relative to the femur. ACL injury is a growing problem; in a study of 17,397 people with 19,530 sport injuries, 37% of the patients had knee injuries. Of this 37%, 45.4% of these injuries involved the ACL with 33.9% of them requiring surgery. 4 A number of repair techniques are currently available, and the success rates for long term clinical outcome are 85%–90%.5–7
The ACL is a dense, highly organized, cablelike tissue composed of types I, III, and V collagen, elastin, proteoglycans, water, and cells. Ligaments have a hierarchical structure with increasing levels of longitudinal organization; collagen molecules form fibrils, multiple fibrils form fibril bundles, and fibril bundles combine to form fascicles, Figure 1. All of these structures are arranged parallel to the long axis of the ligament. 8 The collagen fibrils also display a crimp pattern, a periodic change in direction. In the ACL, the crimp pattern repeats every 45–60 nm.9,10 The fascicles contain collagen fibrils, proteoglycans, and elastin. The ligament is surrounded by an epiligament sheath. 11 The ACL is also has antromedial and posterolateral bands and is twisted approximately 180° from the femoral attachment site to the tibial attachment site. 10

A diagram of tendon/ligament organization. Reproduced with permission from Silver et al 2003. 32
The ACL is a viscoelastic tissue; its behavior is strain rate dependant. The combination of collagens, elastin, proteoglycans (such as decorin, hyaluronan, biglycan, fibromodulin, lumican, epiphycan and keratocan), and water and their arrangement in the tissue give ligaments their unique properties. Proteoglycans such as decorin organize and align the collagen fibrils during development. The presence of large charged proteoglycans allow ligaments to swell with water, imparting viscoelastic behavior to the tissue. The arrangement of proteoglycans along the collagen fibrils allows the fibrils to slide by each other during the application of strain, leading to viscous dissipation of stress at low strain.
The crimp pattern of the collagen fibers also plays a role in the behavior of the ACL. The presence of the crimp pattern allows ligaments to increase in length under low strains without straining the collagen molecules and plastically deforming the collagen fibers, Figure 2. This enables the tissue to respond to the presence of maintained stress and still recover (up to a certain amount of strain).

Schematic of a stress-strain curve for ligament or tendon displaying the toe, linear, and yield regions.
Due to the chemistry and arrangement of their components, ligaments display tri-phasic behavior when placed under tensile loads (as seen in Fig. 2). The first phase is the toe region, an area where the ligament exhibits a low amount of stress per unit strain (low slope). When force is first applied to the tissue it is transferred to the collagen fibrils, causing lateral fibrillar contraction, straightening of the crimp pattern, and stretching of the flexible regions of the collagen molecules and microfibers. 12 The next phase of tensile behavior is the linear region, which displays an increase in slope. Once the crimp pattern is straightened and flexible regions are stretched, the force is directly translated into collagen molecular strain.10,13 The collagen triple helix is stretched and interfibrillar slippage occurs between crosslinks leading to an increase in stress per unit strain.14,15 The yield and failure region is the last phase of the tensile behavior. This phase begins with a slight decrease in slope followed by a large drop in slope due to tissue failure. The failure region represents defibrillation of the ligament, 10 the collagen fibers in the ligament fail by defibrillation causing a decrease in slope and tissue failure.14,16 In order to successfully restore the functionality of the knee, an ACL replacement must display the same biomechanical behavior as normal ACL tissue.
Traditional ACL repair options, past synthetic grafts, and strain induced tissue growth
Traditionally, ACL injuries have been treated with biological based grafts (autografts or allografts).11,14 Both autografts and allografts possess good initial mechanical strength and promote cell proliferation and new tissue growth. However, they suffer from a number of disadvantages. Autografts, tissue from the patient, inherently require additional surgery and which has been known to cause donor site morbidity, increased recovery time, and possible pain at the harvesting site. 17 Autograft material for ACL repair is usually taken from the patient's hamstring, patella, or quadriceps tendons. The patella and hamstring tendon tissues are the most commonly used autografts. The patella tendon graft material is often utilized as a “bone-patellar-bone” graft; this is considered the gold standard of ACL autografts. In this graft the tendon is removed with a piece of bone from the patella and from the insertion point at the tibia. It is then fed through a tunnel drilled through the tibia, drawn across the knee, and anchored into a tunnel drilled through the femur. 8
Allografts, tissues obtained from cadavers could potentially transmit disease, bacterial infection, and may elicit an unfavorable immunogenic response from the host.1,17,18 The benefits of using allografts include the lack of a second surgery for tissue harvest. There is also no limit to the supply of graft tissue as experienced with autografts. Allografts are usually taken from cadaveric patella tendon, hamstring tendon, and achilles tendon.19,20
Many past attempts have been made to use non-degradable, synthetic materials as ligament replacements. 21 These grafts can be divided into the following categories: permanent replacements (which are not amendable to tissue ingrowth), augmentation devices (which protect biological grafts from loads during the early postoperative period), and scaffolds (which allow tissue ingrowth). Some of the non-degradable synthetic materials that have been used include carbon fibers, polyethylene terephthalate (PET), polypropylene (PP), and polytetrafluoroethylene (PTFE).11,14,22–25
The Leeds- Keio ligament is a woven porous tube composed of PET and attached to woven tapes.10,26 This device is designed to allow the ingrowth of new tissue. The Kennedy Ligament Augmentation Device is a cylindrical PP prosthesis with a diamond-braided construction. This device is implanted in conjunction with biological grafts such as patella tendon tissue.10,26 The Gore-Tex prosthesis is composed of an expanded PTFE fiber that is wound into loops, which are joined together to form a braid.27,28
Although these synthetic devices initially supply the function of the ligaments that they replace or protect the ligament that they augment, these devices fail over time because they cannot duplicate the mechanical behavior of the ligament over time. Permanent replacements are susceptible to long-term mechanical failure due to creep and fatigue. 21 Augmentation devices may shield the biological graft from stress, which leads to poor long-term neoligament formation. Repeated elongation of these devices leads to permanent deformation at the points of stress. 21 Contact with sharp edges of the bone tunnel can cause abrasions that weaken the implant and create debris that can cause synovitis in the joint. 21 Woven prostheses face the additional problems of axial splitting, low tissue infiltration, low extensibility, and abrasive wear. Eventually, these implants fail due to fragmentation, stress shielding of new tissue, fatigue, creep, and production of wear debris.24,29,30 None of these devices have been approved by the FDA for primary ACL repair, but some have been approved for augmentation. 31
In addition to biomaterials and growth factors the use of mechanical strain on cell seeded devices has also become a technique used for enhancing tissue regeneration. The organization of the cellular matrix and the strains that they are subjected to have been shown to have a significant effect on fibroblast behavior in tendons and ligaments. The orientation of nanofibers in a matrix has been shown to affect cellular orientation and shape. Mechanical interactions between cells and the underlying extracellular matrix play a critical role in cell regulation by regulating different gene products. 32 Cellular behavior can be altered by changing the magnitude of strain, strain rate, and type of strain (constant or cyclic).
The effects of mechanical forces have been studied on isolated fibroblasts and fibroblasts cultured on various surfaces. Breen studied fibroblasts cultured on flexible-bottom surfaces coated with fibronectin, laminin or elastin. 33 The cells were observed to align perpendicular to the force vector. 33 Mechanically loaded cells expressed higher levels of procollagen mRNA and incorporated more labeled proline into protein than unstressed cells. 33 In other studies fibroblasts cultured in 3-D collagenous matrices align themselves with the direction of principle strain.32,34,35
Studies by Hannafin et al show that the application of 5% strain for two hours that a significant increase in β3 expression in ACL and MCL cells grown on laminin. 36 Exposure to strain also increased α5 integrin expression in ACL and MCL cells grown on collagen. 36
Webb et al noted that fibroblast-seeded polyurethane constructs subjected to a regime of cyclic strain (10% strain, 0.25 Hz, 8 h/day) experienced a mechanical strengthening effect. 37 This was accompanied by increased type I collagen and fibronectin production, strain-induced increases in cytokine production, and significantly increased gene expression for type I collagen, TGFβ-1, and CTGF. 37
A successful ACL device must be designed to successfully support the mechanical loads experienced in the knee. Implanted materials will eventually fail due to fatigue, fragmentation, or other issues. Therefore a successful ACL device must be designed to promote or allow the growth of new tissue and degrade over time to prevent stress shielding. It should also take advantage of the fibroblasts' tendency to align with fibrous structure and strain. In light of these criteria and past device limitations a number of researchers have looked to tissue engineering as a new direction for ACL replacement and augmentation. Researchers have gone in a many different directions in order to develop devices have that fulfill each of these criteria; they vary in their material composition and structure. These devices can be classified as natural polymer based devices, synthetic polymer based devices, and natural tissue based devices and each has its own set of advantages and disadvantages. These are listed in Table 1 and discussed in more depth below.
A summation of all of the three basic types of ACL replacements, their advantages, and their disadvantages.

Natural polymer based devices
Among the materials used in biodegradable tissue-engineered grafts are type I collagen and silk.18,21,38–41 Some of the advantages of collagen are the capability of altering resorption rate and mechanical properties of scaffolds through crosslinking and its low antigenicity. These scaffolds experience an early decrease in mechanical strength followed by tissue remodeling between 10 and 20 weeks with a strength gain similar to autografts. Fibrous proteins such as silk or collagen are composed mainly of specific amino acid sequences repeated throughout the primary structure, this creates homogeneity in the protein's secondary structure (collagens exhibit triple helical structures and most silks display β-sheet conformations).18,38,39,42 The rigid, extended structure of these proteins also gives them the mechanical properties necessary for the replacement of load bearing materials making them excellent materials for ACL replacements.18,38,42
Dunn has studied the use of type I collagen fibers in potential ACL scaffolds.24,38 The grafts showed excellent biocompatibility and enhanced cell attachment, proliferation, and production of extracellular matrix. Unfortunately this scaffold did not fare well mechanically; the collagen scaffold is made from type I collagen fibers arranged in parallel (other scaffolds have been made with synthetic polymers coated with a collagen solution). Groups of aligned fibers lack structural reinforcement and do not prevent fatigue. The arrangement of the fibers in parallel with the direction of stress may cause long-term failure due to fatigue, creep, and abrasive wear.
Another natural polymer based tissue engineered structure is a matrix composed of twisted silk fibers developed by Altman et al.18,38,39 This structure combines the use of a three-dimensional, porous matrix with the use of isolated cells that have been allowed to proliferate

Photograph of one of the six silk fibroin cords used to generate the ACL replacement. Reproduced with permission from Altman et al 2002. 38
Biocompatibility tests with bone marrow stromal cells (BMSCs) show that the silk matrix is not cytotoxic.18,38,39 The twisted fiber architecture gives the scaffold mechanical properties that are similar to ACL. As the matrix is subjected to tensile load the twisting pattern straightens, creating a toe region; this is followed by a linear region. This behavior is important for the prevention of damage due to fatigue and creep. The matrices have a maximum load of 2337 ± 72 N, strain at failure of 38.6% ± 2.4%, and elastic modulus of 354 ± 26 N/mm, which are similar to ACL. The biocompatibility and ability of these matrices to elicit new tissue growth can been increased by coating the surface with RGD sequences. 39 The addition of RGD sequences has been shown to increase cellular attachment and proliferation. The presence of the RGD sequences on the silk fibers also increased extracellular matrix (ECM) by BMSCs which could lead to faster tissue regeneration.
Synthetic polymer based devices
In recent years, a variety of different materials and structures have been investigated for use in tissue engineered ligament replacements. Most of these are synthetic, biodegradable polymers; they include poly glycolic acid (PGA), poly lactic acid (PLA), their copolymers, polyurethane urea (PUU), 44 poly desaminotyrosyl-tyrosine ethyl carbonate (poly (DTE carbonate)), polydioxanone (PDS) and poly caprolactone (PCL).8,21,44 The use of synthetic biodegradable polymers has several benefits. There is no limit to the supply of grafts (as opposed to autografts) and there is no risk of disease transmission. These polymers are designed to degrade over time and therefore do not cause a long term foreign body response. The mechanical properties of the device may also be controlled by altering the degree of polymer crystallinity, changing the polymer molecular weight, or changing the ratio of each polymer in the copolymer.
A poly (DTE carbonate) scaffold developed by the groups of Dunn and Kohn has shown the ability to support fibroblast growth and display the necessary strength for use as an ACL graft. 44 The use of PDS as a potential material for scaffold construction has been slowed. Investigations have shown that the rapid loss of its mechanical strength due to degradation makes it a poor choice for use in ligament tissue engineering. 45 Once again, structure is a potential flaw in many of these matrices. The (poly (DTE carbonate)) and other PUU grafts were composed of polymeric structures arranged in parallel. The poly (DTE carbonate) matrix is made of parallel fibers and the PUU structure is a woven band. These designs may lead to sudden failure due to lack of structural reinforcement. The arrangement of fibers in parallel with the direction of stress may cause fatigue and creep.
Laurencin and his colleagues have developed a tissue engineered scaffold based on a cell seeded, degradable, three-dimensional (3-D) braided, poly L-lactic acid (PLLA) scaffold.2,46,47 PLLA is a degradable polymer which allows load to gradually shift from the implant to the neoligament over time. This scaffold uses 3-D braiding techniques to create a scaffold with controlled pore size, well integrated pores, resistance to wear and rupture, and mechanical properties comparable to the ACL (Fig. 4). The fibers in the 3-D braiding technique all reinforce one another increasing scaffold strength. The control of pore size and integration of pores are important for the distribution of nutrients throughout the scaffold, removal of waste from the scaffold, cell motility, and the development of new tissue throughout the scaffold. This braided scaffold also has a hierarchical structure similar to the ligament. It is composed of PLLA fibers (similar in diameter to collagen fibers) which are arranged into bundles and woven throughout the scaffold thickness.
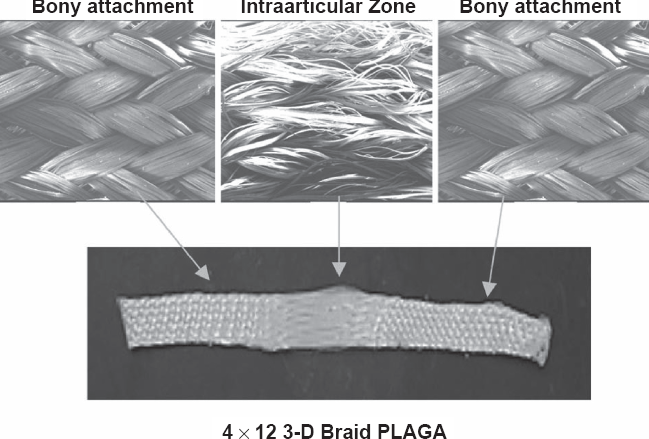
Photograph of the 3-D braided ACL replacement. This device has three sections for bone and ligament growth based on the polymer fiber braiding angles. Reproduced with permission from Cooper et al 2005. 2
In the past there have been woven or braided ligament replacement structures which performed well in the short term after implantation, but the long-term outcomes of these prostheses have been poor.22,23 These braids were limited by poor tissue integration, poor abrasion resistance, and fatigue.48,49 The 3-D braided scaffolds have three regions: a femoral tunnel attachment site (bony attachment end), a ligament region (intra-articular zone), and tibial tunnel attachment site (bony attachment end), as seen in Figure 4. The attachment sites have a higher fiber braiding angle than the intra-articular zone. These angle differences cause changes in pore size between the areas. Studies have shown that a minimum pore diameter of 150 μm is necessary for bone growth into scaffolds and 200–250 μm for soft tissue ingrowth.48,49 The different regions of the scaffold contain pore sizes within these ranges to encourage tissue (ligament and bone) ingrowth and capillary supply. The higher braiding angle at the insertion points also provides resistance to wear within bone tunnels, and improves the integration of bone tissue. The pore interconnectivity extending through the implant increases the overall surface area for cell attachment, allowing tissue ingrowth into the interior of the scaffold.
In
Another recent design is the braid-twist scaffold.51,52 It combines two techniques (fiber braiding and fiber twisting) that are commonly used in textiles and have been used separately in previous ligament prostheses (Fig. 5). Braiding is a technique that has been used to create products designed to bear axial loads and provide mechanical reinforcement. 53 Braided structures are shear resistant, conformable, and can transfer large loads while provide extension. 50

Photograph of the twist-braid scaffold for ACL replacement. This device combines fiber braiding with twisting to achieve ligament-like mechanical behavior.
The twisting of fibers is used in the textile industry to form yarns. 54 The twisting direction and degree of twisting affect yarn strength, abrasion resistance, and flexibility. A low degree of twist produces weaker yarns that pull apart more easily and can develop protrusions on their surfaces from abrasions. Increasing the amount of twist improves yarn strength and abrasion resistance. Although if the yarns are wound too tightly (and the fibers become increasingly perpendicular to the long axis of the yarn), the strength and abrasion resistance decrease. 54 Combining fiber twisting with fiber braiding yields a mechanically stable structure with a larger load capacity and greater degree of extensibility. The degree of braiding or twisting can be altered in order to match the device mechanics with the mechanics of the tissue being replaced. 52
The structure of this scaffold is also similar to the organization of a native ligament and is designed to mimic the biomechanical behavior of the ACL (display a toe region and linear region when placed under increasing load). It is composed PLLA fibers (which are bundles of microfibers, approximately 20 μm in diameter), a degradable poly α-hydroxyester that has been approved by the FDA for implantation in other biomedical devices.51,52 In previous studies, the braid-twist scaffold with the best degree of twisting and braiding had an ultimate tensile stress (UTS) of 81.6+ 1.6 MPa, elastic modulus of approximately 750 MPa, toe region length of 4%, and strain at failure of 30%. 52 The UTS for human ACL has been measured at 38 ± 9 MPa, which is lower than the UTS of the braid-twist scaffold.52,55 Mechanical tests on human ligaments have yielded various elastic moduli values, 65 MPa to 111 MPa, 10 180 ± 25 MPa, and 242 ± 28 MPa 56 Previous studies indicate that human ligaments have toe regions that range from 2.0% to 4.8%.56–60 Higher UTS and modulus values may be necessary to allow the device to degrade while still bearing the appropriate amount of load.
Stress relaxation tests on these scaffolds show that the braid-twist scaffolds have a rapid decrease in stress followed by a plateau region, similar to natural ligament tissue. 51 Unfortunately the final relative stresses (0.873 and 0.829) were higher than those seen in ACL and posterior cruciate ligament (PCL) (0.63 and 0.75).51,55,61 Mathematical modeling of the viscoelastic behavior demonstrates that the stress relaxation behavior can be changed by altering the braiding angles and twisting angles. 51
These scaffolds were also evaluated for their ability to sponsor fibroblast proliferation. 51 The scaffolds displayed the ability to sponsor the growth of patella tendon fibroblasts. The results of MTS assays showed an increase in the number of viable cells over 28 days. Scanning electron microscope images also showed the presence of ECM material secreted by the cells onto the braid-twist scaffolds. 51
Biological tissue based devices
Concerns with devices produced from biological tissues are usually based on the source of the material, when using tissues from a source other than the patient. These concerns include the potential of bacterial infection, disease transmission, or unfavorable immunogenic response.8,48 Some sterilization methods for these tissues can weaken their mechanical properties. On the other hand, they do not require a second harvest surgery, as in autografts. There is a virtually unlimited supply of graft tissue for these devices and they have the appropriate initial mechanical strength (depending on the tissue source). 48 They also promote cell proliferation and new tissue growth.
Xenografts (tissues from animals) have been presented as an option for ACL repair. These tissues have the same advantages and disadvantages as allografts, but they may also carry the additional risk of transferring a disease seen in animal populations to a human host. Rejection of the foreign tissue is another very serious risk of xenografts. Recent work by Stone et al has looked to reduce these risks; they have shown that specially pretreated xenografts are viable options for tissue repair, including the ACL.8,21,49,62–65 Stone and colleagues have utilized chemically modified grafts from cloned pigs as ACL replacements. In preparation for implantation, the porcine graft material is immunochemically modified and chemically crosslinked.8,49,62–66
The immunochemical modification involves the enzymatic removal of the α-gal epitopes in order to prevent graft rejection. This process eliminates the interaction between the natural anti-Gal antibody and α-gal epitopes. This interaction has been a major obstacle in the use of porcine tissues in humans.64,65 Recently, the cloning of pigs lacking α-gal epitopes has eliminated this obstacle.65,67 In addition, the ACL grafts used in these studies have been pulse lavaged to remove cellular components further reducing the risk of rejection. The grafts have also been crosslinked with 0.10% gluteraldehyde for 12 hours followed by glycine endcapping to block unreacted gluteraldehyde molecules and sterilization by electron beam irradiation at 17.8 kGy.65,68 These steps increase mechanical strength and sterilize the graft respectively.
In an
The implants promoted the regeneration of new ligament tissue 65 with signs of graft remodeling extending from the periphery of the graft to its center. In addition, after 12 months the porcine grafts displayed comparable ultimate load, yield load, stiffness and ultimate displacement to monkey grafts. The strength of the implanted treated grafts increased from 43% to 58% between 6 and 12 months. The grafts also demonstrated lower values for ultimate strength, yield strength, ultimate strain, and modulus compared to intact ligaments. 65
The animals were tested for signs of porcine graft rejection. 68 Blood samples were taken prior to surgery and after surgery, at days 10, 14, 21, 28, 42, 56 as well as at 3, 6, 9, and 12 months. Blood samples were analyzed for the presence of anti-Gal and anti-non-Gal antibodies, including antibodies to proteins present in the porcine grafts. Serum immunoglobulin (Ig) anti-Gal IgG and IgM activity was determined by ELISA. The analysis showed a greater increase in anti-Gal titers (>200%) in animals with the untreated porcine graft when compared to animals with the treated graft (95% lower than the untreated) within 2 weeks following implantation. The response to the untreated grafts indicates acute rejection which may lead to graft destruction and resorption. It is hypothesized that the smaller increase in anti-Gal titers in animals with the treated grafts may be due to an immune response not to α-gal epitopes on the graft itself, but those on the porcine bone marrow cells in cancellous bone of the bone-ligament-bone graft. The anti-Gal titers reached resolved preimplantation values by 8 to 12 weeks after implantation.
In an additional clinical study by Stone, these porcine grafts were implanted into human subjects for ACL replacement. 65 Western blotting analysis and ELISA showed the presence of anti-non-gal antibodies against multiple pig xenoproteins in the grafts. The antibody levels peaked from 2 to 6 months, but the antibodies were no longer produced 2 years after implantation. No antibodies were produced against human ligament proteins. After 2 years, 5 of the 6 patients displayed no problem with the function of the porcine graft.
Conclusion
As the number of incidents of ACL injury increases in increasingly younger populations, additional options for ligament repair that overcome the limitations of current treatments are necessary. The ACL is a complex, highly ordered tissue with mechanical properties that are important for normal knee kinematics. These new options must display the mechanics of the original ligament while sponsoring the growth of new tissue and resisting rejection from the body. In response to these criteria, researchers are turning to a variety of techniques and material sources. Solutions in this new generation of ACL grafts typically fall into one of three categories, natural materials based devices, synthetic materials based devices, and natural tissue based devices. Candidates from each of these categories have a number of benefits and have achieved degrees of success in ACL replacement and regeneration. The devices listed above represent some of the advancements that have been made in ACL tissue engineering in each of these categories. These devices have been designed to fulfill the needs of a tissue engineered replacements for musculoskeletal tissues; these include structural stability, appropriate mechanical strength, promotion of cell and tissue growth, and the ability to slowly degrade and allow the new tissue to bear the load. As research into ACL replacement and regeneration continues, it is expected that tissue engineering techniques will lead the way in the design, production, and testing of next generation scaffolds to will mimic the mechanics of natural ligament and lead to the quick and complete regeneration of a new, mechanically sound, natural tissue.