
Abstract
Introduction
Hyponatremia is the most commonly seen electrolyte disorder seen in nearly 6% of the hospitalized patients. 1 The clinical presentation of hyponatremia is variable and is related to a huge extent to the rate of decline of the serum sodium concentration and the magnitude of fall in serum sodium concentration. Serum sodium concentration rapidly falling to less than 120 mEq/l is usually considered a medical emergency. A gradual fall in serum sodium levels may be completely asymptomatic. The symptoms of hyponatremia are usually neurological-headache, lethargy, disorientation and ataxia which may progress to seizures, coma, brainstem herniation, respiratory arrest and death. 2
Hyponatremia has been found to be, unlike hypernatremia, a significant independent predictor of 6-month and 1-year direct medical costs.
3
Persistent hyponatremia has been identified as a poor prognostic indicator in patients with heart failure. Of the 433 patients with heart failure enrolled in the ESCAPE (Evaluation Study of Congestive Heart Failure and Pulmonary artery catheterization Effectiveness) trial, hyponatremia (serum sodium levels less than 134 mEq/L) was present in 23.8% of the patients (n = 103). Within this group, 68.9% (n = 71) had persistent hyponatremia. Hyponatremia was associated with an increased mortality at six months after covariate adjustment (hazard ratio [HR] for each 3 mEq/l decline in sodium concentration = 1.23; 95% confidence interval [CI] = 1.05 to 1.43;
Hence, much attention has been paid to the development of treatment modalities for this disorder. Vasopressin receptor antagonists are the newest addition to the therapeutic options for the treatment of hyponatremia, tolvaptan being one of them.
Mechanism of Action
Vasopressin or anti-diuretic hormone is a polypeptide synthesized in the supraoptic and paraventricular nuclei in the hypothalamus. It is contained in granules which travel down the axons of the supraopticohypophyseal tract to the posterior pituitary where it is stored and subsequently released upon stimulation. 5 Vasopressin is released primarily in response to hyperosmolarity and decreased real and effective circulatory volume. 6 The effects of vasopressin are mediated through three receptor subtypes: (1) Vasopressin type 1 receptors (V1Rs) (2) Vasopressin type 2 receptors (V2Rs) and 3) Vasopressin type 3 receptors (V3Rs). 7 The details of these receptors are summarized in Table 1. 7
Subtypes of vasopressin receptors.

The binding of vasopressin to the type 2 receptors leads to an increase in the water permeability of the collecting duct causing an increase in the concentration of urine and a fall in serum sodium concentration. 8
The treatment of hyponatremia is determined by the volume status of the patient, presence or absence of symptoms of hyponatremia, severity and duration of hyponatremia. 1 Hyponatremia is classified into three categories based on volume status: (1) Hypervolemic, as in heart failure 9 and liver cirrhosis; 10 (2) euvolemic, as seen in syndrome of inappropriate ADH secretion (SIADH); 2 and (3) hypovolemic, as observed in emesis and diarrhea. 1
Hypovolemic hyponatremia is treated with isotonic saline infusion. The vasopressin receptor antagonists or to be more specific, the V2 receptor antagonists have a role in management of only hypervolemic or euvolemic hyponatremia. 11 The effect of V2R antagonists is hypotonic diuresis. 12 Some agents also antagonize V1R to improve systemic vascular resistance and cardiac output to some extent. 13 The receptor binding specificity for some vasopressin receptor antagonists has been summarized in Table 2. 8
Receptor selectivity for vasopressin receptor antagonists.

The modalities being used for the treatment of hypervolemic hyponatremia before the development of V2R antagonists comprised of loop diuretics and an angiotensin converting enzyme inhibitor or an angiotensin receptor blocker to increase the delivery of water to the collecting tubule and improve cardiac output respectively. Euvolemic hyponatremia, on the other hand, has been classically treated with water restriction and the use of loop diuretics, demeclocycline or lithium to antagonize the effects of vasopressin. 9
Tolvaptan is a non-peptide vasopressin antagonist with a V2R: V1R selectivity of 29:1 for human arginine vasopressin receptors cloned in HeLa cells. 14
Pharmacokinetic Profile and Metabolism
In terms of pharmacokinetics, there is significant variability amongst individuals. The pharmacokinetics have been observed to be linear up to the recommended maximum daily dosage of 60 mg. At higher doses ranging from 60–480 mg orally daily to healthy volunteers, the pharmacokinetics remained linear although the peak plasma concentration was found to increase at a lesser rate compared to the recommended maximum dosage. 15 The increase in mean serum sodium levels is not dose dependent but the urine volume increases linearly with increment in doses. 16 The absolute oral bioavailability of tolvaptan is around 56% and is unaffected by ingestion of food products. 15
The time taken to achieve peak plasma concentration (Cmax) is nearly 2–3 hours. 17 In patients with chronic heart failure, steady state pharmacokinetic parameters were observed after administration of 30 mg of the drug daily for 7 days (n = 20). The Cmax achieved was 283 ng/mL after a median time of 2 hours (tmax) after administration. The mean area under the concentration-time curve (AUC) over 24 hours was 3087 ng-h/mL. The average plasma steady state concentration was 129 ng/mL and the mean minimum plasma concentration at the end of once daily dosage interval was 48 ng/mL. The pharmacokinetic profile was similar in a group of patients with heart failure randomized to receive 15 mg of tolvaptan twice daily. 15 In patients with HF, with doses of 30 mg and 90 mg, the Cmax attained was 460 ng/mL and 723 ng/mL respectively. 17
The volume of distribution of tolvaptan is nearly 3 L/kg. The drug is highly protein bound (98% to 99%). Tolvaptan is metabolized primarily via the cytochrome P 450 (CYP) 3A isoenzymes and is eliminated by non-renal routes. Less than 1 percent of the drug is excreted in the urine unchanged. 15 The half-life of tolvaptan is nearly 6–8 hours. 17 The clearance of tolvaptan is 4 mL/min/kg in healthy people which is reduced to half in patients with hyponatremia of any etiology. 15 In patients with NYHA class II or III heart failure, the mean elimination half-life was 9.4 hours following oral administration of 30 mg of tolvaptan once daily for 7 days. 15
Moderate to severe hepatic impairment and heart failure reduce the clearance and increase the volume of distribution of tolvaptan but the changes are clinically irrelevant. In patients with renal impairment, with variable creatinine clearance rates between 10 and 79 mL/min, no difference was found in exposure to tolvaptan when compared to individuals with normal renal function. Age does not seem to affect plasma tolvaptan concentration. 15
Since the drug is metabolized by CYP3A and is an inhibitor and substrate of P-glycoprotein, it has significant drug interactions. Administration of the drug with ketoconazole, an inhibitor of CYP3A, increased the exposure to tolvaptan nearly 5 fold. 17 Hence tolvaptan should not be administered with strong inhibitors of CYP3A like ketoconazole, clarithromycin, ritonavir, indinavir, nelfinavir and nefazodone as per US prescribing information. Concurrent administration of rifampicin, a CYP3A inducer reduced the exposure to tolvaptan by nearly 85%. When used with inducers of CYP3A, increased dosages are hence needed. When administered with a P-glycoprotein inhibitor such as cyclosporine, increased dosage is needed. 16 Co-administration with digoxin (a P-glycoprotein substrate) increased the exposure to digoxin 1.3 fold while there were no significant changes in pharmacokinetics when administered with warfarin, amiodarone, furosemide, hydrochlorothiazide or lovastatin. 15
Clinical Studies
Tolvaptan has been studied in animals as well as humans. In animals, there have been studies in both healthy as well as experimental heart failure models. In conscious rats, tolvaptan increased the urine volume, serum sodium concentration and osmolality while simultaneously decreasing urine osmolality in a dose dependent manner when used in a single or multiple dosing regimens. 14 It has been shown to improve serum sodium levels and produce dose dependent aquaresis in both acute and chronic severe hyponatremic rat models. 18 Lewis rats with immunologically mediated myocarditis and heart failure when treated with tolvaptan for four weeks, demonstrated significant electrolyte free water loss without evidence of activation of renin-angiotensin system. 19 In the above models, there was reduced renal expression of aquaporin-2 in spite of elevated levels of AVP suggesting antagonism of V2 receptors. In dogs with heart failure induced by chronic rapid ventricular pacing, tolvaptan increased free water excretion without activating the sympathetic or renin-angiotensin system. At 10 mg/kg dose, tolvaptan decreased the pulmonary capillary wedge pressure along with an increase in urine output. However, there was no alteration of peripheral vascular resistance, renal blood flow or glomerular filtration rate. 17 Hence, tolvaptan reduced the pulmonary vascular congestion without altering the systemic hemodynamics, renal function or levels of the neurohormones.
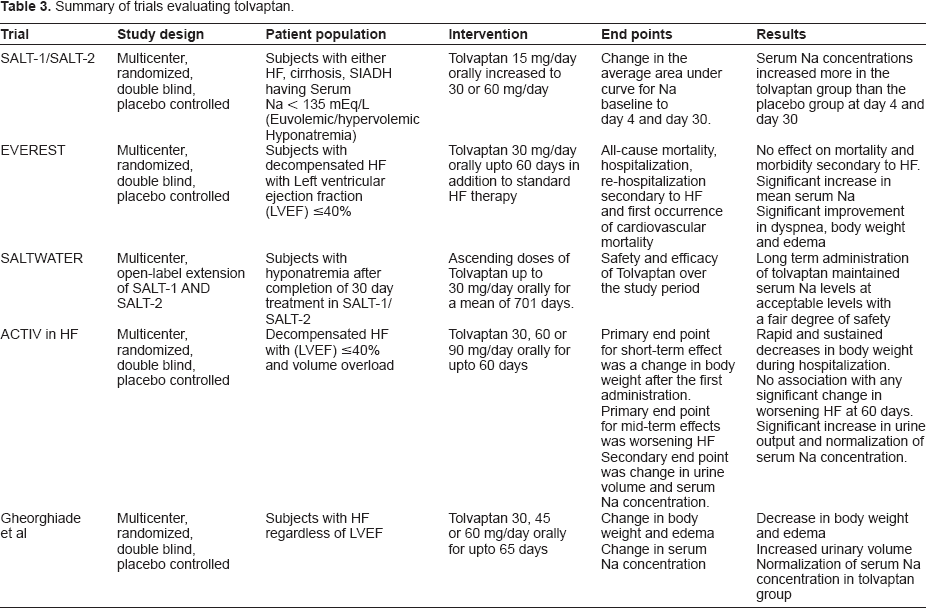
The role of tolvaptan in patients with euvolemic or hypervolemic hyponatremia was assessed in SALT-1 and SALT-2 trials. These were phase-III, multicenter, randomized, double blind, placebo-controlled, multidose trials.
20
The patient population comprised of individuals with heart failure, hepatic cirrhosis and SIADH. The total number of subjects in the two trials was 448 (n = 448). The individuals included in the trials had a serum sodium level less than 135 mEq/l. The subjects were randomized to either the tolvaptan group (n = 225) or the placebo group (n = 223). The dose of tolvaptan used was 15 mg by oral route daily which was increased subsequently to 30 mg or to 60 mg daily, if needed, based on serum sodium concentrations. The primary endpoints in the trials were a change in the average daily AUC for serum sodium for serum sodium from baseline to day 4 and the change from baseline to day 30. In both trials, the serum sodium concentrations increased more in the tolvaptan treatment group than the placebo group during the first 4 days (
The EVEREST (Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan), which was a randomized, double blind, event driven study investigated the effects of tolvaptan in patients with heart failure.
21
In this trial, 4133 subjects hospitalized with heart failure were randomized to receive either tolvaptan or placebo with standard HF therapy in both groups within 48 hours of admission for a minimum of 60 days. The dose of tolvaptan used was 30 mg by oral route daily. The number of subjects in the tolvaptan group was 2072 compared to 2061 in the placebo group. In the tolvaptan group, 1607 subjects completed the study through death or completion while 1620 completed the study in placebo group. The primary end points were all- cause mortality and cardiovascular events or hospitalization for heart failure. The number of events were 871 (42%) in the tolvaptan group and 829 (40.2%) in the placebo group after a median follow-up of 9.9 months (HR 1.04; 95% CI 0.95–1.14;
The SALTWATER trial, a multicenter, open-label extension of SALT-1 AND SALT-2 investigated the safety and efficacy of longer term treatment with tolvaptan compared to the SALT trials. 22 The subjects in the study were participants from the SALT-1 and SALT-2 trials. 111 subjects were enrolled in the SALTWATER trial which is nearly 25% of subjects enrolled in the SALT trials. Of these, 38 had participated in the SALT-1 trial (16 from tolvaptan group and 22 from the placebo group) and 73 in the SALT-2 trial. At the time of enrollment, 17 subjects were normonatremic, 59 had serum sodium concentrations from 130 to 135 mEq/l and 35 had serum sodium concentrations >130 mEq/l. So nearly 85% of patients enrolled in the SALTWATER trial had hyponatremia to begin with. The subjects were administered ascending doses of oral tolvaptan, up to 30 mg orally everyday for a mean duration of 701 days. All subjects enrolled in the trial received tolvaptan at the dose specified above.
A total of 64 patients did not complete the trial. Thirty subjects experienced an adverse event or died, thirteen withdrew consent, nine subjects did not re-enroll. Six subjects experienced a drug related adverse event and the rate of correction of hyponatremia exceeded the desired rate (>1 mmol/L per hour) in five subjects. In one subject, the trial was stopped because of hypernatremia defined as a serum sodium level greater than 145 mEq/l. The mean serum sodium concentration increased from 130.8 mEq/l to 135 mEq/l over the duration of the study. The response in terms of serum sodium concentration was comparable in patients with heart failure and SIADH but was relatively small in patients with cirrhosis. Also, as seen in SALT-1 and SALT-2, the serum sodium concentrations returned to baseline in around 70% of the patients after discontinuation of tolvaptan for 7 days. 22
The ACTIV in CHF (Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Heart failure) was a multicenter, randomized, double blind, placebo controlled trial which evaluated the short and mid-term effects of three different doses of tolvaptan in hospitalized patients with heart failure. 17 In this trial, 1159 patients were screened for symptoms of decompensated heart failure despite standard therapy. 319 patients were enrolled in 34 centers in the United States and 11 centers in Argentina after the screening process. The patients were randomized to receive tolvaptan 30 mg, 60 mg or 90 mg orally daily or placebo in addition to the standard therapy. The patients were followed for 10 days in the hospital and an additional 7 weeks as outpatients. The primary end point for the short term effect of tolvaptan was a change in body weight after the first administration of the drug while the primary end point for mid-term effects was worsening heart failure as evidenced by rehospitalization, unscheduled visit for heart failure symptoms or death within 60 days of randomization. The secondary end points were change in urine volume and serum sodium concentration as an inpatient and patient and physician assessed symptom scales as an outpatient. 17
Tolvaptan 30 mg, 60 mg or 90 mg was associated with greater decrease in body weight at 24 hours after first administration as compared to placebo. However, there was no difference in heart failure symptoms after 60 days of treatment with tolvaptan or placebo. The urine volumes were higher in patients treated with tolvaptan. 17 In the subgroup of patients with hyponatremia at the time of enrollment (n = 68), there was faster increase in sodium levels and often normalization of serum sodium levels in the tolvaptan group compared placebo group. In addition, the effect remained consistent till the last day of visit thus suggesting that the effect of tolvaptan was maintained in patients with chronic heart failure as far as correction of hyponatremia is concerned. 15
In a double blind randomized trial involving 254 patients with chronic heart failure conducted by Gheorghiade et al, the effects of three different doses of tolvaptan (30 mg, 45 mg or 60 mg) were compared with a placebo. A total number of 221 patients completed the study. 59 patients received tolvaptan 30 mg, 59 received 45 mg of tolvaptan, 48 received tolvaptan 60 mg and 55 patients received placebo for twenty five days. The primary end point was a change in body weight while the secondary end points were urine volume, urine osmolality and change in serum sodium levels. In tolvaptan treated groups, there was significant reduction in body weight compared to placebo on the first day of treatment which was maintained through the duration of the study (
The effectiveness of tolvaptan versus fluid restriction and placebo in twenty-eight hospitalized patients with hyponatremia was assessed by Gheorghiade et al. After a two day run in period, subjects were randomized 2:1 to tolvaptan group (n = 17) or fluid restriction plus placebo (n = 11). The dose of tolvaptan used was 10 mg daily. The duration of treatment was 27 days and the subjects were followed up for 65 days. The serum sodium concentration increased by 5.7 ± 3.2 mEq/L in subjects in tolvaptan group and by 1.0 ± 4.7 mEq/L in subjects in fluid restriction group. 23 Trials of tolvaptan in humans with autosomal dominant polycystic kidney disease are still ongoing. 24
Safety
In the SALT-1 and SALT-2 clinical trials, the most common side effects were thirst and dry mouth (doses used- 30 mg and 60 mg) in nearly 15% of the subjects in tolvaptan group. The incidence of adverse events was similar in both the study groups in both trials. There were 26 serious adverse events noted in the SALT trials. Eleven such events occurred in eight subjects in tolvaptan group- dehydration and hypotension, dehydration and dizziness, syncope, acute renal failure, ascites, hypernatremia with increased serum creatinine and Escherichia coli septicemia with respiratory failure. Eight subjects in the tolvaptan group withdrew from the trial because of adverse events-rash (2 subjects), dysgeusia, nocturia, increased urinary frequency, exanthema, muscle weakness and hypernatremia (1 subject each). 15 adverse events occurred in 10 subjects in placebo group (acute renal failure in 2 subjects, rash in 2 subjects, worsening heart failure noted twice in one subject, acute dyspnea with edema, worsening anemia with renal failure, fall in hemoglobin and hematocrit, vomiting, hepatic encephalopathy and dyspepsia in 1 subject each). Eight subjects withdrew from the placebo group (rash in two subjects, acute renal failure in two subjects, hyponatremia in two subjects, renal failure and vomiting in 1 subject each). The number of deaths in two groups was also comparable- 14 out of 223 subjects died in tolvaptan group and 13 out of 220 subjects died in placebo group. 20
The incidence of side effects in tolvaptan group was similar in SALT-1 and SALT-2: commonest being dry mouth and thirst. Other notable side effects were weakness, nausea, constipation, diarrhea, ascites and vomiting. 20
In the EVEREST trial, adverse events resulting in discontinuation of drug administration were noted in 6.5% of the subjects in tolvaptan group and 5.5% of subjects in placebo group. Again, increased thirst and dry mouth were seen more in tolvaptan group (7 subjects were noted to have increased thirst and 4 had dry mouth compared to none in placebo group). Also, hypernatremia was noted in 1.7% of the subjects in tolvaptan group as opposed to 0.5% in the placebo group. The findings were comparable in two groups with regards to changes in baseline blood pressure, heart rate, gastrointestinal symptoms (nausea, constipation, vomiting, diarrhea), renal failure and hypotension. 21
In the SALTWATER trial, 105 of the 111 subjects experienced an adverse event, the common ones being peripheral edema (n = 25), hyponatremia (n = 23), anemia (n = 20), diarrhea (n = 19), urinary tract infection (n = 18), nausea (n = 17), fatigue (n = 15), hypokalemia and headache (n = 14), ascites, hypotension, pneumonia (n = 13), heart failure, thirst and dizziness (n = 12). The adverse events potentially related to tolvaptan therapy were pollakiuria (n = 11), thirst (n = 10), fatigue (n = 6), dry mouth, polydipsia, polyuria, hypotension, hypernatremia, dizziness, headache, peripheral edema and acute renal failure (n = 4). 19 subjects withdrew from the study because of a treatment emergent adverse event. Six of the 19 patients died secondary to heart failure, esophageal varices, hepatic cirrhosis, cerebral hemorrhage and gastrointestinal hemorrhage. The adverse events in the other 13 subjects leading to discontinuation of the study were- ventricular tachycardia, vertigo, gastrointestinal hemorrhage, vomiting, gait disturbances, irritability, increase in serum creatinine, hypernatremia, anorexia, bladder cancer, dysphasia, myocardial infarction and pruritis. Of these, six were thought to be related to tolvaptan therapy- ventricular tachycardia, irritability, hypernatremia, anorexia, renal failure and pruritis. The rate of correction of sodium was higher than the acceptable rate in five subjects. Eighteen subjects experienced hypernatremia of which one withdrew from the study while the hypernatremia resolved in the remaining 17 subjects. 22
Summary of trials evaluating tolvaptan.
Efficacy
In the SALT trials, the average daily area under curve for serum sodium concentration was significantly higher in the tolvaptan group compared to placebo regardless of the fact whether the hyponatremia was mild or severe at baseline. The results were seen consistently within 8 hours of administration of tolvaptan and for the total duration of the 30 day study period.
20
The serum sodium concentration corrected faster in the tolvaptan group and the number of patients with normal serum sodium concentration were higher in the tolvaptan group than placebo at day 4 and day 30 of therapy. However, when the subjects were followed up the week after discontinuation of tolvaptan, there was no difference in the rate of fall in serum sodium concentration in two groups.
20
Also noted was the fact that the patients in tolvaptan group required lesser fluid restriction than the placebo group (9.3% in tolvaptan group vs. 17.5% in placebo group). The study also assessed the health status of subjects on day 30 using scores for the Physical Component Summary and the Mental Component Summary of the SF-12 Health Survey. The scores were similar on the Physical Component Summary but improved significantly for the Mental Component Summary in tolvaptan group (
In the EVEREST trial, mortality at the end of 1 year was 25% in tolvaptan group and 26% in placebo group (HR = 0.98;
In the SALTWATER trial, correction of serum sodium occurred at a rate comparable to SALT-1 and SALT-2 trials and the serum sodium levels were also similar by day 14 in all trials. The fact that the subjects in SALTWATER had previously been treated with tolvaptan in SALT-1 and SALT-2 did not alter the long term effects of tolvaptan. In addition, the mean serum sodium levels remained within the normal range throughout the study period. In subjects with marked hyponatremia, serum sodium tended to correct at a faster rate whereas in subjects with hepatic cirrhosis, the final sodium levels attained seemed somewhat lower than rest of the subjects. By week 4 of the study, 60% and 45% of the subjects in the mild and marked hyponatremia group respectively, had normal serum sodium levels. However, when tolvaptan was discontinued, serum sodium levels declined (3 mEq/L in 68% of the subjects) in all subjects by 7 days. Fluid restriction was needed in 13.2% of the subjects in mild hyponatremia group and 5.4% of the subjects in marked hyponatremia group. One subject received urea while no subject required demeclocycline. 22
The acute hemodynamic effects of tolvaptan in patients with systolic cardiac dysfunction and symptomatic heart failure were studied in an international, multicenter, randomized, placebo controlled trial by Udelson et al. 181 patients with advanced HF on standard treatment were randomized to tolvaptan (15,30 or 60 mg) vs. placebo. Tolvaptan significantly reduced pulmonary capillary wedge pressure, pulmonary arterial pressures and right atrial pressures at all doses. In addition, dose dependent aquauresis was noted within 3 hours of initiation of tolvaptan. 28
Patient Preference and Place in Therapy
Tolvaptan seems to be a logical choice based on the underlying pathophysiological mechanism of euvolemic or hypervolemic hyponatremia. The group of patients in whom tolvaptan has been studied fall in the above two categories with underlying disease processes being SIADH, heart failure and hepatic cirrhosis. Of the three subgroups of patients, the numbers seen in day to day practice are much higher in the HF and cirrhosis group. As seen in the SALT trials, the effects of tolvaptan on serum sodium levels in patients with hepatic cirrhosis is modest. The increments in serum sodium levels have been best demonstrated in patients with SIADH which seems logical.
In patients with HF, tolvaptan has been shown to be beneficial in correcting hyponatremia in both SALT as well as EVEREST trials. However, there has been no clear survival benefit as far as cardiovascular mortality and worsening heart failure leading to hospitalization are concerned.
21
Another consideration in the use of tolvaptan in patients with HF has been the increased levels of circulating vasopressin which might lead to excessive stimulation of V1Rs located on cardiac myocytes thus causing fibrosis and worsening of HF. However, this concern seems only theoretical based on the EVEREST trial which revealed that the mortality difference between tolvaptan group and placebo group was within the pre-specified non-inferiority margin (
The use of tolvaptan has not been associated with rapid over-correction of serum sodium levels in patients with hyponatremia. This is relevant considering the chronic nature of hyponatremia in patients with heart failure. Another practical consideration in patients with hypervolemic hyponatremia is fluid restriction and compliance with the same. The use of tolvaptan in such patients may potentially overcome this problem by increasing the free water elimination.
The data on the use of tolvaptan suggests its use in chronic hyponatremia. Thus far, there have been no studies investigating the use of tolvaptan in acute and severe hyponatremia. Tolvaptan and other V2R antagonists begin to increase the serum sodium concentration within a few hours of administration. The current treatment for acute severe hyponatremia is hypertonic saline which may cause volume overload in patients with existing fluid overload. Hence, it may be worthwhile exploring the use of V2R antagonists in this setting. As of now, the use of tolvaptan in this scenario is not recommended. 29
Currently, tolvaptan is supplied in 15 mg and 30 mg blister packs containing 10 tablets each with the average wholesale price being close to US$ 300.00 per day. 30
Conclusions
Hyponatremia is a very common electrolyte disorder observed both acutely as well as chronically. Tolvaptan is an exciting, fairly new treatment modality for euvolemic and hypervolemic hyponatremia. Clinical studies thus far suggest its use in chronic hyponatremia. Tolvaptan has clearly demonstrated short term benefits especially in correcting hyponatremia. The instances of rapid over-correction of serum sodium levels have been few. However, there has been no evidence of tolvaptan improving long term survival in the patient population studied above. This probably remains the greatest challenge to widespread use of the drug. The cost of the drug is a factor dictating the use of the drug as well.
The drug itself is tolerated fairly well, the most common side effects being thirst and dry mouth. However, the drug may be beneficial in diminishing the need for fluid restriction. An important consideration in the use of tolvaptan is its potential for drug interactions considering its metabolism through the CYP3A4 pathway. Currently, the initiation of tolvaptan is recommended in an inpatient setting with frequent monitoring of serum electrolytes.
Disclosure
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.