
Abstract
Keywords
Introduction
Prostate cancer is the most common cancer and the second leading cause of cancer-related deaths among men in the United States (American Cancer Society, 2024). Risk factors for developing prostate cancer include older age, race/ethnicity, lifestyle factors (e.g., diet and physical activity), family history of prostate cancer, and prostate cancer genetics (Bergengren et al., 2023; Lowder et al., 2022). There is a limited understanding regarding the underlying molecular mechanisms of this disease and issues regarding excessive screening, overdiagnosis, and overtreatment of non-aggressive prostate cancer within the general population (Moyer & Force, 2012).
While screening for prostate cancer through prostate-specific antigen (PSA) testing can lower mortality rates (Martin et al., 2024; Van Poppel et al., 2022; Vickers et al., 2023) by increasing early detection, the benefits of screening continue to be debated, and clinical trials have produced mixed findings. Recently, in the randomized prostate, lung, colorectal, and ovarian cancer screening trial, no significant decrease was observed in prostate cancer-specific mortality in the screening group compared with usual care group (Georgiou & Scarbrough, 2024). Widespread PSA screenings may lead to the identification of cancers that would not pose clinical risks during a man’s lifetime, resulting in unnecessary treatment of indolent or slow-growing tumors (Pinsky et al., 2019). In addition, falsely elevated PSA tests can cause patients to seek out additional, more invasive prostate cancer diagnostic testing, such as transperineal biopsies, which pose the risk of infection in patients who may not have had prostate cancer in the first place (Pepe & Pennisi, 2022). National organizations have thus called for informed decision-making, a deliberative process to develop an individual understanding of the potential harms and benefits of asymptomatic screening with PSA (Moyer & Force, 2012). However, existing decision aids have not incorporated personalized genetic risk information (Davis et al., 2014; Gwede et al., 2015). Current guidelines recommend that individual men participate in informed decision-making and shared decision-making (in collaboration with a clinician) about screening, considering factors, such as age, race/ethnicity, family history, and individual values and preferences (Jackson et al., 2022).
Polygenic risk score has focused on a key research question of predicting which individuals have the risk of developing a disease (Baptista, 2005), in this case, higher likelihood of developing prostate cancer. Genome-wide association studies and fine-mapping efforts performed by the prostate cancer consortium (PRACTICAL) have identified 269 single nucleotide polymorphisms (SNPs) associated with prostate cancer susceptibility (Conti et al., 2021). The SNP genetic profiles refer to variations in a person’s DNA sequence at a single nucleotide base, which can influence susceptibility to diseases, such as cancer. These results may have clinical utility in genetic risk assessment for unaffected men from diverse racial-ethnic groups and varying risk levels. By analyzing these genetic variations, health care providers can better assess the potential aggressiveness of prostate cancer and categorize patients into appropriate risk groups for tailored management and treatment strategies.
The overarching research question of which men have a high likelihood of developing prostate cancer using individual genetic profiles among unaffected men to estimate risk categories in that population has not been completely investigated yet. These SNP genetic risk profiles have not been incorporated into screening decision aids; hence, it is not known what impact the integration of personalized genetic risk information has on prostate cancer screening informed or shared decision-making. It is also important to note that further understanding of SNP information from racially diverse unaffected men is needed before we can translate this information into a risk communication message to inform screening behaviors.
The primary focus of this study was to assess individual prostate cancer genetic risks and susceptibility beliefs among unaffected men and evaluate the willingness to provide a biospecimen (saliva sample) for prostate cancer genetic testing and determine genetic risk category. Compared with women, men participate less in genetic research, mostly due to lower awareness of genetic risk and genetic risk testing (Peshkin et al., 2021). In particular, Black men are significantly underrepresented in genetic research due to historical mistrust of medical research, lack of awareness about genetics and genetic testing, concerns regarding data usage, and limited access to research opportunities (Connor et al., 2022). Thus, this article centers on recruitment, enrollment, and biospecimen collection outcomes, and beliefs in genetic testing from a pilot study with unaffected men from diverse race and ethnic backgrounds. The findings from this pilot study are essential to understanding the feasibility and effectiveness of recruitment strategies, participation rates and provide insights into the challenges, opportunities and lessons learned that inform design of future larger studies. This study was approved by Advarra Institutional Review Board (IRB no.: Pro00063775).
Method
Recruitment
This pilot study investigated the feasibility of community-based recruitment, enrollment, and collection of epidemiologic data, beliefs on genetic testing, and saliva samples (biospecimen) for prostate cancer genetic risk testing among a diverse sample of unaffected individuals who are of are potential eligible for screening per national guidelines and prevailing clinical practice. A purposive community-based recruitment approach was used to enroll a target sample of 100 male individuals from diverse racial/ethnic backgrounds, ages 40 and older, with no personal history of prostate cancer, regardless of a family history of prostate cancer or previous screening experience for prostate cancer. The study targeted older males (40 years and older) due to the median age for patients diagnosed with prostate cancer being 67 years old (Raychaudhuri et al., 2025), and national guidelines for prostate cancer screening informed and shared decision-making centered around this age range (American Cancer Society, 2023). Given the known increased prostate cancer risk for Black men, the study placed emphasis on reaching Black men (of diverse African ancestry). The study used a cross-sectional observational approach, combining survey methods and biomarker genetic risk testing. For individuals who completed both components of the study, researchers would be able to gauge an individual’s genetic risk with a one-time approach (Wang & Cheng, 2020).
Recruitment was conducted using various community-based approaches and virtual methods using opportunities provided by community partners (e.g., non-profits, culture centers, and faith-based organizations) and programs offered at a cancer center in southwest Florida focused on community outreach. These included outreach efforts supported by the Office of Community Outreach, Engagement, and Equity by leveraging the Tampa Bay Community Cancer Network Partnerships (Community Advisory Board), and by the cancer centers Program for Outreach, Wellness, Education, and Resources (MPOWER) (outreach programming), which reaches out to the cancer centers of 23-county catchment area in West Central Florida. The study was also promoted through the cancer centers’ social media channels and additional media outlets, such as community organizations’ e-blasts and newsletters. This article provides recruitment efforts from March 2022 to April 2024.
Various recruitment approaches used successfully in a similar community-based study (Davis et al., 2018) were employed including active recruitment (in-person) and passive recruitment via flyers (online postings, media and other passive dissemination methods).
Passive (contactless) recruitment included flyers posted on community boards at locations identified through Google searches; online including digital flyers on Facebook pages, websites and listservs, and local television; printed flyers posted in libraries, newsletters, newspapers, and laundromats. In addition, word of mouth by enrolled participants helped disseminate flyers and individual referrals. All flyers featured QR codes that directed individuals to the study description, eligibility checklist, consent form, and survey questionnaire for eligible individuals to complete enrollment. In some cases, prospective participants contacted the study team via phone calls to express interest in the study.
To widen reach, the study team developed an outreach letter introducing the study, providing study rationale, eligibility requirements, study components, and relevancy to the event goal. Further engagement of event organizers was facilitated via phone calls, follow-up emails, or in-person visits by study staff to establish trust. A variety of collaboration methods were implemented, including tabling with educational materials and giveaways for attendees, informational sessions via a presentation by the study principal investigators, and/or providing study flyers for event organizers to distribute in their prepared informational packets. This milieu of methods has been effectively employed to reach racially and ethnically diverse individuals in community settings (Davis et al., 2018). Certainly, unique opportunities to increase visibility of the study in communities included the distribution of flyers to locations like libraries, thrift stores, Black-owned businesses, salons, and other places with high density of diverse populations.
Study Instrument/Questionnaire Description
A survey questionnaire from a prior study of prostate cancer patients, which focused on genetic risk for first-degree male relatives (Roy et al., 2020), was adapted to assess beliefs and attitudes about genes and genetic testing for risk of prostate cancer among unaffected individuals. The full questionnaire can be found in (Supplemental Appendix A). The relevant survey questions that were used for this article are summarized below.
Sociodemographics, Clinical, and Health Behaviors
Participants reported their age, race/ethnicity, education, marital status, employment status, health insurance coverage, family history of prostate cancer, tobacco and alcohol use, and prior PSA screening.
Perceived Genetic Risk and Susceptibility Beliefs
Participants answered questions about their knowledge and understanding of genetics, awareness and knowledge about the PSA screening controversy and screening informed decision-making, as well as their perceived comfort or difficulty in providing a blood or saliva sample for prostate cancer genetic risk testing, their perceived personal lifetime risk of developing prostate cancer, and their comparative risk of developing prostate cancer compared with other men of their own age.
Similar to the survey of prostate cancer patients (Roy et al., 2020), this survey included three different hypothetical genetic risk scenarios varying in level of genetic-related risk of developing prostate cancer ranging from 10%, 30%, and 50% greater than general population risk for prostate cancer. The hypothetical scenarios used in this study were created by the research team leveraging literature (Andrykowski et al., 2010; Roy et al., 2020). An example scenario and question were: Imagine you are working with your doctor to make a decision on screening test for prostate cancer. Imagine your doctor tells you there was a simple blood test that could help determine whether you carry genes that may give more information about your chances of developing an aggressive form of prostate cancer. There is some evidence to suggest that treating aggressive prostate cancer early improves a man’s chances of cure and long-term survival. Based on a genetic test, imagine your doctor knows you have gene variations that make it likely you have a 30% greater chance of having aggressive prostate cancer compared to a man who doesn’t have the genetic variations. How important would it be for your doctor to tell you this before you begin or continue with annual screening for prostate cancer? (check one response). Not important at all; A little bit important; Somewhat important; Very important; Extremely important.
Saliva Sample Kit Collection (DNA Genotek, Ottawa, Canada)
After enrollment and completion of the survey questionnaire, each participant was provided with a saliva sample kit with collection instructions. For the purposes of this study, the saliva sample collection was exclusively for genetic risk testing; this information was explained to participants in the informed consent. Individuals enrolled by in-person method were handed a saliva sample kit to complete and return to study staff on site. Accordingly, saliva kits were mailed to participants enrolled via online or other non-in-person methods. A postage paid, pre-addressed return mailing packet was included for the completed saliva kit to be returned to the research team.
Statistical Analysis
Baseline characteristics of the study participants were compared across primarily two racial groups (Blacks vs. Whites). Numerical variables were analyzed using the Student
Results
The overall recruitment and enrollment experience is summarized in the study Consort Diagram (Figure 1). A total of 154 individuals responded or were reached using passive and active recruitment methods. Among these, 10 could not be reached to assess eligibility or had incomplete eligibility online, and 19 were excluded for not meeting inclusion criteria, resulting in 125 eligible participants. Among those eligible, 24 did not complete consent, and one did not complete the survey, leaving 100 eligible participants who enrolled and completed the survey questionnaire.
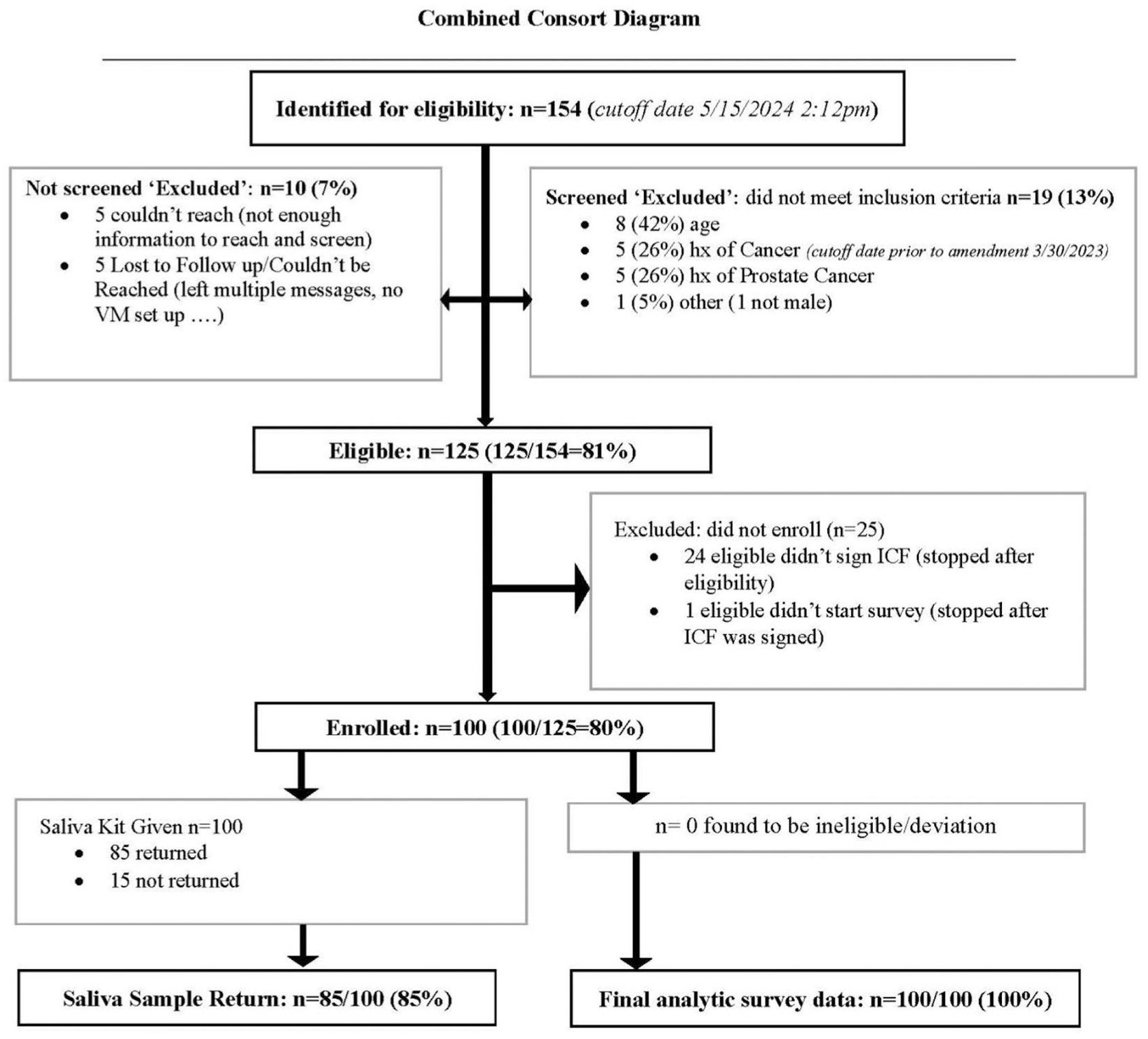
Consolidated Standards of Reporting Trials (CONSORT) Diagram—Showing the Number of Participants Screened, Eligible, Enrolled, and Included in Final Analyses
Sociodemographic and Clinical Characteristics
Table 1 summarizes the selected characteristics of enrolled participants. The majority of enrolled participants were Black or African American (62%), reported having health insurance coverage (92%), and had no family history of prostate cancer (80%). The average age was 57 years and 45% reported having had a PSA test at least once in their lifetime. There were no substantial differences among racial groups except for health insurance. Compared with Black men, Whites were less likely to have private health insurance (32% vs. 52%).
Selected Characteristics of Participants.

Prostate Cancer Susceptibility and Genetic Risk Beliefs
Table 2 summarizes prostate cancer susceptibility and genetic risk beliefs. Overall, 76% of individuals felt they had a risk of developing prostate cancer during their lifetime with 24% believing they had a 0% chance of developing prostate cancer, 39% believing they had a 10%- to 30% chance, and 29% believing they had a 40% to 60% chance. Eight percent believed their lifetime risk to be 70% to 100%. Perceived lifetime risk was slightly greater among Black men than White men (
Self-Reported Knowledge, Awareness, and Beliefs of Participants.

Saliva Sample Donation for Genetic Risk Testing
With regards to the feasibility and receptivity of saliva sample collection, Table 3 represents saliva sample return rates by race and recruitment method among those with complete survey data. All 100 enrolled men were offered in-person or mailed a saliva sample kit. Overall, 85 men returned their saliva kits yielding a return rate of 85%. For in-person recruitment (kits delivered in person), the saliva kit return rate was 95% (58/61); whereas for the mailed kits (for media and phone recruited participants), the return rate was 69% (27/39). In addition, there were no racial differences noted with approximately 89% (55/62) of Black males returning saliva kits compared with 90% (19/21) among White males. Overall, 31 consented participants were born outside the United States, and 71% (22/31) of them submitted a saliva sample kit (data not shown in the table).
Saliva Kits Returned by Race/Ethnicity and Recruitment Method.

Saliva kits were delivered and returned in-person (for in-person recruitment) and by mail (for online or other recruit).
Saliva sample kit return among other race = Asian (3/3 returned), American Indian/Alaska Native (2/2 returned), and other (6/12 returned).
Discussion
This community-based pilot study explored the feasibility of recruitment and participation of unaffected individuals from diverse racial backgrounds and assessed their willingness to submit a saliva sample for prostate cancer genetic risk testing. Given the disproportionate burden of prostate cancer among Black/African American men, our sample purposefully included more Black men. This study demonstrates that community-based recruitment, enrollment, and saliva sample collection from racially and ethnically diverse men is feasible even in the pan COVID-19 period (beginning March 2022 as community-based in-person interactions and outreach programs were resuming). Accordingly, we found that majority of eligible participants (100/154) enrolled in the study, suggesting high receptivity to the research. Most enrolled participants were reached in person (61%), particularly among Black males compared with other groups.
We also found comparable rates of receptivity and participation in biospecimen donation for genetic risk testing among Black and White participants with 89% and 90% saliva sample kit return rates, respectively. Overall, saliva sample kit return rate among participants was 85%, with slightly lower rates among men of “other” racial groups. In addition, saliva kit return rates were higher for in-person kit return than mailed kits. As such, future studies should consider engaging participants in person to boost both enrollment efficiency and saliva kit return. Finally, the findings regarding knowledge, awareness, and genetic risk beliefs suggest most men perceive themselves to be at increased risk of developing prostate cancer and are motivated to know their individual genetic risk test results.
An important consideration and lesson learned in conducting these types of studies is the personnel resources needed for “boots on the ground” efforts. Despite having vested community partners and organizations promoting the study, when study personnel were available to interact with prospective participants, the reach and enrollment yields improved drastically. Compared with online/contactless efforts, in-person recruitment interactions engender trust, provide an opportunity to answer questions and clarify study procedures, and offer an immediate opportunity to deliver, collect, and receive the completed saliva sample kits. Although multiple modalities are needed to reach more people, online and other contactless methods are associated with lessor yields. Nevertheless, the convenience afforded by virtual/online and contactless methods should be appreciated and promote practical and less resource intensive options. Furthermore, a wide variety of in-person events were used in this pilot study, including health-fair-oriented, traditional and cultural events, as well as other innovative venues, such as DMVs, barbershops, and online groups. This range of recruitment methods increased diversity in participants and, by utilizing word of mouth referrals and testimonials added value and increased trust (Davis et al., 2018; Harvey et al., 2024). It is important to remain flexible in expanding both eligibility criteria and recruitment approaches to reach broader and diverse audiences beyond those already engaged in health-seeking settings (e.g., health fairs) to engage other community settings, such as DMVs and laundromats.
Although this was a small pilot study, the results are promising. Going forward, to increase outreach to local communities, multifaceted approaches are needed to reach individuals, promote participation, and engage with community organizations. However, we are aware of the limitations of our study. Our inclusion criteria were men ages 40 and older, because the median age of prostate cancer diagnosis is 67 and the American Cancer Society recommends that men begin discussions about prostate cancer screenings beginning at age 50 (if they are at average risk), and earlier for those at increased risk. As such, we cannot generalize our findings to persons below 40 years old. Future studies should consider genetic risk in younger men. Also, potential confounding effects of sociodemographic characteristics, including age, income, health literacy, and educational level were not evaluated. As such, these factors could have possibly influenced participant engagement and study findings. In addition, our study was available only in English. Thus, there was limited reach for groups whose preferred language is not English; for example, Florida has a large Spanish or Creole-speaking/preferring population. Finally, due to oversampling of Black men and fewer numbers in the other racial/ethnic groups, our findings may have limited generalizability to the general population.
Conclusion
This pilot study demonstrated the feasibility and challenges of recruiting diverse male participants in community settings in the immediate pan/post-COVID-19 era. The lessons learned about using multimodal recruitment approaches directly inform future research efforts. Furthermore, in-person delivery of saliva sample kits reduces rates of non-return. As such, when possible, biospecimen kits should be presented and collected during in-person interactions when motivation to participate is highest. When in-person interaction is not possible, mailing is a reasonable alternative but should be complemented with multiple reminder calls to boost saliva sample kit return.
Our next steps include DNA extraction for the 85 samples received and the generation of personalized polygenetic risk scores. In the long run, if genetic risk information is determined to be useful in motivating screening decisions and behavior, it could be incorporated into existing prostate cancer screening decision aids (Seibert et al., 2023).
Supplemental Material
sj-pdf-1-jmh-10.1177_15579883251410526 – Supplemental material for Feasibility of Recruitment, Perceived Genetic Risk and Susceptibility Beliefs, and Saliva Sample Collection in a Community-Based Prostate Cancer Genetic Risk Pilot Study
Supplemental material, sj-pdf-1-jmh-10.1177_15579883251410526 for Feasibility of Recruitment, Perceived Genetic Risk and Susceptibility Beliefs, and Saliva Sample Collection in a Community-Based Prostate Cancer Genetic Risk Pilot Study by Carol Boxtha, Samaa El-Kolalli, Justin Denis, Ashley O’Neil, Susan T. Vadaparampil, Rania Abdulla, Hyun Park, Jong Y. Park and Clement K. Gwede in American Journal of Men's Health
Footnotes
ORCID iDs
Ethical Considerations
Informed Consent
Author Contributions
Funding
Declaration of Conflicting Interests
Supplemental material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.