
Abstract
Introduction
Deep neck space abscess (DNSA) is a severe infection that may cause life-threatening conditions.1,2 The most common origin is odontogenic etiopathogenesis.
3
Despite the general acceptance that DNSA originates from infection, the rate of positive bacterial culture is 30%–50%.
2
It has been reported that
Magnesium is the second most abundant intracellular cation (K+
Magnesium deficiency may occur due to decreased intake and/or absorption, renal excretion and polypharmacotherapy interactions with age. Chronic magnesium deficiency can cause increased oxidative stress 9 and low-degree inflammatory response. 10 Thus, a susceptibility to infection and inflammation may occur, especially in the elderly. Magnesium can play a role in the immune response as a cofactor for immunoglobulin synthesis and other processes tightly associated with the function of T and B cells. 11 Magnesium is also required to biosynthesize, transport, and activate vitamin D, which is an important factor in the fight against infectious diseases. 12
It is observed that the elderly are prone to both magnesium deficiency and DNSA.1,5,6,9 In magnesium deficiency, it is possible that many of the protective biochemical reactions mentioned above slow down and the immune system weakens. This situation is likely to be associated with infection related diseases such as DNSA. Besides, chronic magnesium deficiency is associated with augmented baseline inflammatory reaction related to oxidative stress.10,11 Considering the infection-predisposing1,2,11 and inflammation-enhancing9–11 effects of magnesium deficiency, as well as the infection origin and inflammatory nature of DNSA, it is reasonable and scientific to hypothesize that there may be an important relationship between magnesium deficiency and DNSA. Taking all together, the importance of magnesium for immune reactions and infectious diseases and the association of magnesium deficiency with various infections are worth considering.9–13
However, to date, it has not been investigated whether magnesium deficiency is present in patients with DNSA. Therefore, the present study aimed to test the hypothesis that magnesium deficiency may be associated with DNSA, and to compare serum magnesium concentrations between patients with DNSA and healthy controls.
Materials and methods
This was a retrospective case-control study. Sample collection was conducted between January 2023 and December 2023. The local ethical approval was received retrospectively (date: January 12, 2024), no: 2024/01-16). This study was conducted following the ethical standards of the Declaration of Helsinki. A written informed consent was routinely obtained from all patients and healthy controls before any procedure was initiated.
In this study, 23 patients with DNSA and 23 matched healthy controls for age, gender, and smoking status were included. The frequency of affected deep neck spaces and the most frequently isolated bacteria in the patients with DNSA were recorded. Healthy controls were recruited from among the patients’ relatives or companions from the same geographical area. Healthy controls were also evaluated in terms of general symptoms and signs of infections or diseases such as pain, fever, sweating, high blood pressure, increased pulse as well as the blood cells including leukocytes, neutrophyles, lymphocytes, monocytes, and thrombocytes.
On the other hand, cases aged <18 and >65 years were excluded from this study. Also, pregnancy or lactation, fasting, mental illness or lack of cooperation, malignant diseases, immunodeficiency, penetrating neck injuries, gastrointestinal disabsorption, consuming immunosuppressive drugs or magnesium supplementation were exclusion reasons. In addition, normal individuals who had mentioned symptoms or signs suggestive of infection, inflammation, or diseases were excluded from the control group.
While samples were taken, participants were ensured to be in a resting and lying position after a 12-hour overnight fast and in the morning. Abscess drainage and multiple antibiotics were applied to all patients with DNSA.
Measurement of serum magnesium levels
The atomic absorption spectrometry (Thermo Scientific C103500100, Beijing, China) was used to determine serum magnesium concentrations. This is accepted as the reference method for the measurement of magnesium, since it provides the most accurate magnesium levels. However, it is not practical and has negative features such as expensiveness and technical difficulties. 14 This method is based on the principle of absorbing electromagnetic rays of the element atoms gasified by increasing the temperature and calculating the absorbed beam according to the Lambert-Beer law. 15 Accordingly, venous blood (4 mL) taken from participants was placed in a biochemistry tube. This blood sample was centrifuged at 3000 rpm for 10 minutes in a Nuve NF-800 brand centrifuge. Then, the serum was separated and kept at −20°C. On the day of processing, the stored samples were brought to room temperature (15 °C–18 °C) by carefully mixing and swirling. Then, 1 mL of serum and 1 mL of 20% TCA were taken into falcon tubes. These tubes were closed, vortexed, and kept in an oven at 90°C for 15 minutes. Then the samples were cooled and centrifuged. The obtained supernatant was taken into new tubes and analyzed. 15
Statistical analyses
In the statistical analyses, the patient and control groups were compared in terms of clinical features including age, gender, smoking status, and laboratory features including magnesium levels, blood cells, and CRP levels. In addition, statistical correlations between magnesium and other laboratory parameters were analyzed.
The variables obtained from the groups were assessed and compared using statistical analyses performed with IBM SPSS version 20.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov-Smirnov test was used to determine whether continuous variables had a normal distribution. Accordingly, CRP and monocyte scores in the DNSA group; and magnesium scores in the control group were found to be non-normally distributed. Parametric and non-parametric tests were applied for normally and non-normally distributed variables, respectively. The Mann-Whitney U test was used in the comparison of CRP, monocyte, and magnesium scores between the two groups. For the comparison of normally distributed continuous variables, the student
Results
The affected deep neck spaces were anterior triangle ( Affected deep neck spaces. A: Anterior triangle (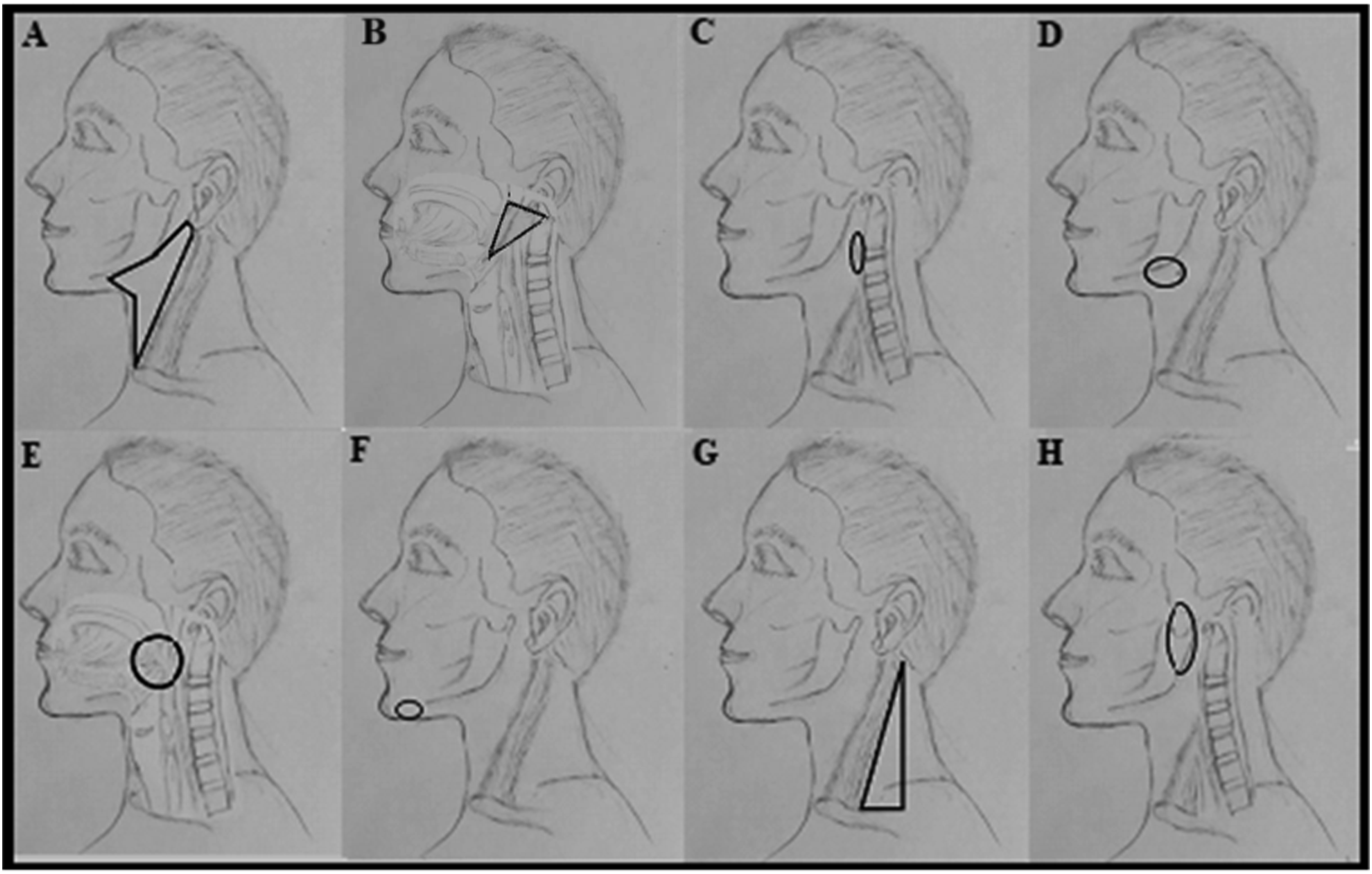
The bacteria isolated from DNSA.

The characteristics of patients and healthy controls.

aThe student
bThe Fisher’s exact test.
cThe Mann-Whitney U test.
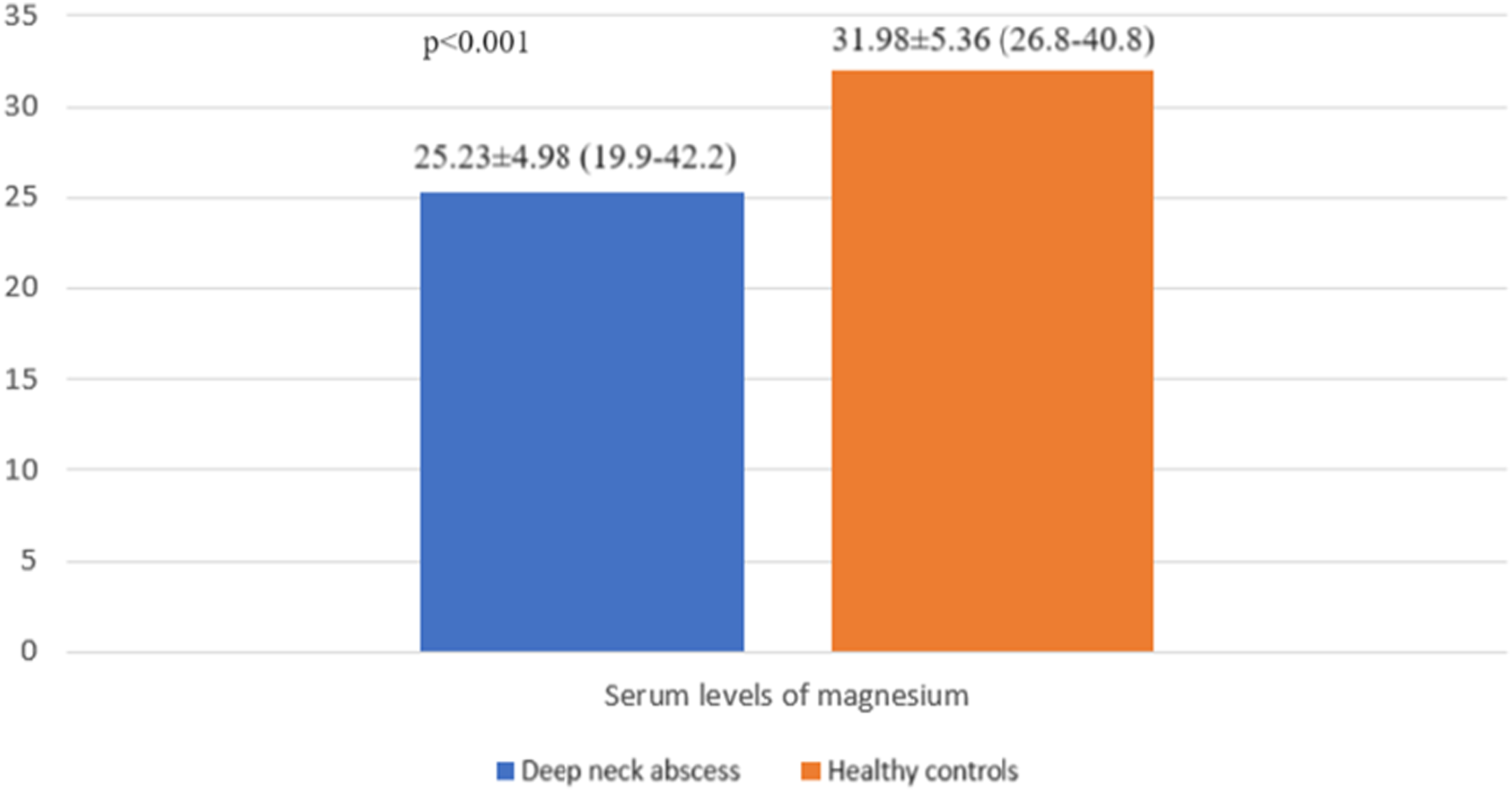
Figure 2 demonstrates the distribution of serum magnesium levels in the groups, and Figure 3 presents the comparison between the two groups in terms of serum levels of magnesium. Accordingly, serum magnesium concentrations showed a statistically significant difference between the two groups. More specifically, patients with DNSA had significantly decreased serum magnesium levels (µg/dL) compared to healthy controls [25.23 ± 4.98 (19.9–42.2) versus 31.98 ± 5.36 (26.8-40.8)], ( Distribution of serum magnesium levels in the groups. Serum magnesium levels (µg/dL) in the groups. Values were presented as mean ± SD (min.-max.).
Correlations of magnesium with other laboratory values.

aThe Pearson’s correlation test.
bThe Spearman’s correlation test.
Discussion
Herein, serum magnesium levels in patients with DNSA were addressed in a retrospective case-control study. As a result, patients with DNSA had lower serum magnesium concentrations than matched healthy controls. In addition, magnesium was significantly and inversely correlated with CRP in patients with DNSA. Therefore, from an etiopathogenetic perspective, decreased serum magnesium levels may be associated with DNSA. However, this was the first study to evaluate the research topic in the literature, and its results need to be confirmed.
Given the pivotal multifunctions of magnesium in the body,8–13 it is possible that the insufficiency of magnesium can be involved in immune system weakness and susceptibility to infections. In light of this sensible and scientific hypothetical inference, the present study addressed serum magnesium status in patients with DNSA which represents a serious infection and is also related to immunodeficiency.16,17 The results obtained in this study indicated that DNSA was associated with lower serum magnesium concentrations, manifesting in inverse correlation with CRP. Although no study to date has investigated the relationship between DNSA and magnesium, previous studies have displayed a significant inversely correlation of magnesium with CRP in various inflammatory disorders,18–21 in consistent with our correlation findings in patients with DNSA. On the other hand, Coşkun Benlidayı et al 22 have reported no significant correlation between serum magnesium level and CRP in patients with knee osteoarthritis. Similarly, we found no significant correlation between magnesium and CRP in healthy controls. These compatible findings suggest that magnesium and CRP are not correlated with each other in non-inflammatory conditions.
However, it is challenging to establish the causative factors of decreased serum magnesium levels in patients with DNSA that were detected in this study. Also, considering the case-control design of the study, it is not clear if this finding is a cause or consequence of DNSA. Therefore, several thoughts can be put forward regarding the emergence of this finding. For example, given various interactions between electrolytes, 23 reduced magnesium intake and other electrolytes due to appetite loss and pain or their increased use resulting from the disease may have caused decreased serum magnesium concentrations in patients with DNSA.
To date, serum magnesium concentrations in various disorders have been examined. 24 However, no studies have investigated the status of this fundamental element in patients with DNSA. Therefore, a detailed and in depth discussion section including comparative results from different studies could not be generated. Nevertheless, in parallel to our findings, Wang et al 25 have shown a strong association between magnesium deficiency and sepsis which is a similar condition to DNSA.
On the other hand, the limitations of this study should be considered. This was a planned retrospective case-control study limited to a certain period. Thus, the number of patients was 23 when the specified time expired. Thus, the study’s features including a small sample size, data from a single center, and a case-control design, are its main limitations. However, this is the first study on the relationship between DNSA and magnesium, and its limitations can be eliminated in further studies.
Conclusion
The results of this study showed that patients with DNSA have decreased serum magnesium levels. This finding suggests that magnesium insufficiency may be associated with DNSA etiopathogenesis. This was the first study on the research topic, and its results need to be confirmed. Also this study may inspire and guide the discovery of new motivations in future research.