
Abstract
Keywords
Introduction
As it connects devices and people, the IoT changes the way to communicate and is ubiquitous across all sectors. With the use of wireless sensor networks, the IoT enhances the connection between individuals and their electronic gadgets. 1 To better serve their users, healthcare systems mostly employ IoT to communicate sequentially. Using an E-healthcare monitoring system, it is possible to observe and evaluate a patient's online behavior. 2 Some applications of IoT monitoring systems include smart homes, smart hospitals, and gadgets that assist individuals with impairments in tracking their own vital signs and activities. 3 With the help of the IoT, electronic healthcare monitoring systems can improve customer service, create more scalable networks, and reduce energy consumption, among other benefits. Many hospitals use an IoT smart e-health gateway as part of their health monitoring system. 4 Enabling electronic healthcare gateways increases network performance and efficiency while reducing monitoring system energy consumption. System for digital electroencephalogram (EEG) monitoring captures and processes EEG signals, allowing healthcare providers to analyze patients’ neurological activity with greater accuracy and efficiency within IoT-supported environments. EEG Signals are vital for patient monitoring because they capture the patient's brain activity in high resolution and enable precise analysis of their health status. 5
With the use of big data analytics, we can sort through vast amounts of data from many different sources. Big data analytics, which unearth hidden datasets and patterns, can be used to find out how accurately the monitoring system covers data. 6 Big data analytics makes use of the classified data from large datasets. By enabling faster database searches, big data analytics contribute to a faster system as a whole. 7 Many monitoring systems in the healthcare business rely on machine learning (ML) techniques for big data analytics. Its performance is enhanced because ML makes the monitoring system more efficient and scalable. 8 Making auxiliary power units more efficient is crucial for any system, and ML methods improve monitoring system performance by doing just that. 9 EHR provide all the necessary information about a patient, including their photo, medical history, and medication details. If all the data included in EHRs could be retrieved and converted into a dataset usable by the healthcare monitoring system, it would be possible thanks to big data analytics. 10 Information already saved in databases, such as personal details, clinical records, and sensor readings, forms the basis of healthcare data analyzing. Due to the increasing number of data created by healthcare facilities across several domains, e-healthcare data analysis technologies are necessary. 11
Better user-to-network communication is the primary goal of deploying wireless sensor networks in healthcare institutions. The main use of ML algorithms and methods in healthcare analysis is in e-healthcare data processing, where they greatly enhance system efficiency.12,13 Medical facilities commonly employ ML algorithms for the purpose of data classification according to predetermined criteria. To construct a suitable dataset for research, comprehend the specific circumstances underpinning the produced data, and examine real-life patient situations, the support vector machine method is employed. 14 Nodes with sensors can find data faster and find its location in the database. As a result, the efficiency of data analysis is enhanced, which is good for all healthcare systems. To sort data according to certain criteria, healthcare institutions employ the K-nearest neighbors method. After data is created, it is compared to data that has already been stored to create a suitable dataset for analysis. 15
Fundamentally, Rendezvous Data Processing Model (RDPM) updates its outputs based on real-time comparisons of sensor data with suggestions. The recommendation logic of the system is updated if new data is found that contradicts the present recommendations. When compared to hidden Markov models (HMMs) and recurrent neural networks (RNNs), state learning greatly increases the flexibility of temporal sequence processing. HMMs calculate the likelihood that visible data will change a hidden state using probabilistic reasoning. When the data is inconsistent or noisy, it might cause forecasts to be wrong. While RNNs are sequence-loving, training them can be a data-intensive ordeal, and they might have trouble handling dependencies that persist over time. However, by keeping tabs on both historical and real-time data, RDPM's state learning system is able to enhance its state saving capabilities and provide more accurate recommendations. By adjusting to data in real-time, RDPM overcomes problems with HMMs and RNNs in e-health. The system needs to be able to make sound judgments because data quality is unpredictable in these situations.
Integrating Big Data Analytics and IoT can enhance E-health monitoring accuracy. Traditional approaches use physical and environmental observations to make patient recommendations. To improve decision-making and patient outcomes, a more precise and effective monitoring system that can analyze vast amounts of data from observed circumstances is needed. The core of the RDPM architecture, Human Activity Recognition (HAR), is the topic of this work. Despite the framework's broad E-health monitoring application, this is true. HAR gives critical information about a patient's mobility, functional state, and compliance with the prescribed level of physical activity for diabetes and cardiovascular disease management. HAR's issues—noisy sensor data, intermittent connectivity, and context-aware interpretation—are similar to physiological monitoring, making it a perfect testbed for the RDPM's flexibility.
While electronic health monitoring systems have been enhanced by the IoT and Big Data Analytics, computerized patient suggestions still lack remarkable accuracy and reliability. Because data is typically processed in batches in conventional systems, isolated data augmentation is seen as the gold standard occurs when earlier suggestions are disregarded during the evaluation of sensor data. A decrease in the accuracy of findings is caused by analytical errors, an increase in the rate of data interruption, and contradictory or redundant suggestions. There is insufficient continuing validation for the existing models to dynamically correlate historical conceptions with analytical errors in real time. The RDPM is one of the possible answers proposed by this research to address this problem. Specifically, this approach excels at enhancing individual datasets. A closed-loop feedback system that incorporates both old and new ideas is created through the application of state learning. Electronic health systems can now give better, more up-to-date recommendations as a result.
To produce more precise suggestions, the system utilizes sensor data, as seen in Figure 1. Gathering data from sensors for analysis is the initial phase in the data collection process. Uncertainty detection is the next step in processing the data. Any incompatibilities between our earlier concepts are now identified and filed away as data problems. Once this uncertainty analysis is finished, the data is passed through the State Learning and Validation component to make it easier for users to understand. It is possible to tell the difference between valid and invalid data. Using verified status data, the suggestion is iteratively changed throughout the Recommendation Adjustment stage. At this point, the integration with the cloud for the IoT is also considered, along with any changes made in real time. Once the proposal has been amended, it is considered the Final Recommendation, ensuring that the system's conclusions are reliable. The system's processing processes are depicted in the flow diagram, which starts with the initial data input and ends with the processed output. Continuous feedback loops can be used to enhance the recommendation quality.

Flow diagram of the proposed model.
RDPM Architecture for Electronic Health Record Systems is:
Implementing the RDPM to enhance the E-health monitoring system's data processing capabilities. By utilizing the capabilities of the IoT, the model offers timely recommendations for patient care, which improves the reliability of decisions in RDPM. With the goal of better communication and analysis of patient information, raise the bar for electronic healthcare monitoring data exchange and analysis. To develop E-healthcare monitoring systems that use ML and AI for more precise healthcare solutions
A summary of the research is provided below. In section “Related works analysis,” the current literature and study techniques are thoroughly examined. The research strategy, methodology, and processing procedures are detailed in section “Proposed method.” Experimental results and performance analysis are covered in section “Experimental result and performance analysis.” Ssection “Discussion” focuses on the discussion, and the final section explores the conclusion and future work.
Related works analysis
For sensor-based healthcare monitoring systems, Harb et al. 16 suggested a novel data analytics procedure. The utilization of IoT is a crucial component of the proposed method for enhancing the overall monitoring system. A patient's precise behaviors can be captured in a dataset by implanting biosensors in their body. The suggested system makes use of sensors to diagnose illnesses, spot emergencies, and ascertain the true state of patients.
Askar 17 used IoMT, cloud and fog computing, smart data analytics, and other technologies to create an intelligent healthcare system that met the project's goal. The system intends to build a diagnostic paradigm for early heart disease treatment. Cloud, fog, edge, and IoMT technologies enable deep support vector machine deployment. Accepting data from many IoMT devices allows for precise diagnoses. F1-score, accuracy, specificity, and sensitivity assess system performance.
Nagarajaiah et al. 18 found that Ambient Assistive Living can meet aging needs and minimize healthcare costs. This project aims to construct an intelligent and efficient health monitoring system using ML. The technology monitors physiological data for early intervention. With support vector machines, you may study sensory input and share condition findings with specialists. Simulation results show that the system performs better than planned. Its low packet loss and latency allow rapid data collecting and alteration.
Munnangi et al. 19 presented a study examining the healthcare industry's use of deep learning techniques, highlighting both the successes and failures of current approaches. A deep learning-based method, Moran Autocorrelations and Regression-based Elman Recurrent Neural Networks, is presented to address the vanishing gradient problem and shorten detection time. According to the experimental findings, the suggested strategy is feasible, increasing accuracy by 96% and reducing execution time by 18.5%. The proposed method is a perfect example of an IoT-enabled smart healthcare system because it effectively recognizes health status activities.
Subahi and Athama 20 displayed that the healthcare industry must use intelligent information systems due to the increasing availability of digital health-related data. These systems can manage and manipulate this data, improving health care and supporting decision-making. Expert decision-support systems are necessary because the intensive care unit experiences surges in admissions during seasonal illnesses and pandemics. The article presents a method for classifying the health risks of new hospital admissions using domain-specific knowledge graphs and fuzzy-logic inference.
Ismail et al. 21 proposed Regular Target Detection and Recognition Model (RTDRM) health factor analysis process based on a convolutional neural network. A larger dataset is used in the convolutional neural network model to help identify disease types. The Pearson correlation coefficient is also used in the proposed method to classify disease types. Regular pattern behavior is one data mining technique that may aid in effective data pattern discovery for categorization. Compared with other existing ML models, the proposed model outperformed by increasing prediction accuracy and reducing energy consumption.
Zyukov et al. 22 reported the development of a mathematical model to predict fasting blood glucose levels in individuals with diabetes mellitus; the study used data from 359 patients. Based on a linear regression approach, the model computed its results using IBM SPSS Statistics Version 23. Bread units had the most tremendous impact on glucose levels, and women with type 2 diabetes had the highest accuracy. The best ways to address comorbidities should be the subject of future research.
Daliya et al. 23 presented Industries such as transportation, retail, and healthcare rely on precise analysis and decision-making facilitated by the massive volumes of data generated by smart systems and IoT networks. Healthcare providers may use ML algorithms to anticipate how a condition would proceed. To predict the onset of diabetes in 442 participants, this research used an optimum Multivariable Linear regression method using demographic data including age, gender, BMI, and blood serum measurements. Patients may be able to get medical advice that slows the course of diabetes over a year thanks to the model's improved accuracy compared to non-optimized models.
Waleed et al. 24 being demonstrated this study introduces an IoT patient monitoring paradigm that stores, processes, and displays data in the cloud. Sensing, networking, and application are the three components that make up the model, subsequently reduces data volume by filtering and variable sampling, enabling greater patient monitoring. Advanced data analysis and individualized healthcare treatments are also made possible by the models that include AI and ML services. Data protection, real-world testing, and integrating ML and AI should be the focus of more research.
Zhou et al. 25 proposed a new HAR method based on an Improved Bayesian convolutional network (IBCN) for healthcare centers that uses the IoT. The interaction between patients and medical facilities relies heavily on radiofrequency technology. In order to extract the latent variables needed for recognition, convolution layers are used in the feature extraction process. To protect users’ anonymity and security, we use an extended deep learning strategy. The suggested approach improves the system's dependability while simultaneously decreasing noise.
The use of IoT-based data processing and monitoring in various fields, including healthcare, is enhancing electronic health systems. Khan et al. 26 developed a context-aware precision agriculture system by integrating sensor networks, cloud-based analytics, and the IoT. This was done to suggest adaptive fertilizer. Real-time IoT cloud integration and context-aware learning enhance decision accuracy, according to their research. The success of IoT frameworks highlights the promise of recommendation systems for data-driven and dynamic decision support across domains.
Cheltha et al. 27 improved human motion recognition with RNNs, multiple-hypothesis tracking, and hybrid RDA-WOA optimization handling noisy occlusions. Metaheuristics like RDA/WOA hybrid optimize neural network parameters and reduce sensor interruption performance loss. This endeavor is connected to RDPM's goal of reducing data interrupts in e-health monitoring, which might compromise system accuracy owing to temporary signal loss or partial sensor readings.
Asmat et al. 28 developed an information-centric IoT Proximal Policy Optimization caching solution using deep reinforcement learning. The clever and adaptive caching decisions reduce latency and boost data availability in busy IoT cloud networks. Deep reinforcement learning optimizes subsequent judgments in complex real-time scenarios, enhancing data processing efficiency and scalability, according to RDPM.
Novel IoT and cloud designs, optimization techniques that use cloud and IoT data, and intelligent caching make data-driven systems more dependable, efficient, and flexible. The suggested RDPM uses state learning, IoT-cloud rapport, and dynamic data processing to improve healthcare ideas and eliminate patient monitoring disruptions. Table 1 of the literature review demonstrates few strategies that combine scalability, dynamic error minimization, and adaptive state learning. Dynamic, context-dependent, high-volume e-health monitoring exists. These issues are not solved by current solutions because they are centrally located, use static models, or handle data streams individually. RDPM's meta-cognitive state learning creates a “rendezvous” between sensor data and analytical recommendations, a learning loop. This allows IoT-supported healthcare systems to revolutionize scalable, accurate, and continuously improving patient care.
Comparison of related methods and their key limitations.

Proposed method
This study comprises an experimental and simulation-based model, performed in collaboration with Princess Nourah Bint Abdulrahman University, AlMaarefa University, and the University of Business and Technology, Saudi Arabia, between January 2025 and May 2025.
The goal of this data processing model is to make e-health system recommendations more accurate by taking into account previous suggestions and patient help with physical observation data. Wearable health trackers like Fitbit, Apple Watch, and others are part of the E-health monitoring systems paradigm. These systems use smart, communication-based technology to collect and store patient data. 29 These systems use IoT to improve processing and data exchange. 30 Figure 2 shows the suggested model.

Proposed model.
The suggested IoT cloud architecture simulates real-world deployment scenarios beyond computational simulation. The system's three-tier architecture optimizes data flow and processing efficiency. Wearable MDs, such as blood glucose monitors and virtual smartwatches, collect physiological data at the edge tier. These devices can broadcast raw sensor data to a topic on an IoT Core message broker, such as Amazon Web Services’ IoT Core or Microsoft's Azure IoT Hub, using the lightweight MQTT protocol. Low-power, trustworthy communication is possible even over unreliable networks. In addition to ingestion and security, the cloud gateway tier authenticates each device, ensures the safe reception of telemetry streams, and validates and formats initial data. This layer manages data bursts and separates data ingestion and processing. It triggers a serverless function, such as AWS Lambda or Azure Functions, to package the data and send it to a high-throughput message queue, such as Apache Kafka or AWS Kinesis. Information is processed in real time as it is obtained. As a containerized microservice in a Kubernetes cluster, the RDPM may be automatically scaled, and the core cloud processing layer consumes this stream. This service processes information in near real time to understand the situation and provide advice. In conclusion, historical analysis uses PostgreSQL, and dashboards use InfluxDB. End users receive important alerts via secure WebSocket connections. In addition to accuracy, this pipeline must be tested for end-to-end latency, message throughput, and concurrent device management. This ensures the pipeline is feasible.
The health monitoring devices gather data at specific intervals, store it, and analyze it from the e-healthcare environment. Sensor devices that measure temperature, blood sugar level, blood pressure, etc., are equipped with communication-based systems. Improving the precision of these systems via observational data analysis is the primary goal (refer to Figure 2). The proposed RDPM uses big data analytics to design and analyze these systems. By reducing isolated data augmentation, the proposed approach aligns with prior suggestions but introduces analytical inaccuracy. Wearable sensor devices monitor the input data, which is then compared to the data processing model's earlier suggestion.
The E-health monitoring system consists of a centralized data-processing model that analyzes observed data in line with previous recommendations.
Analysis of past recommendations
The wearable sensors used to gather data from the E-health monitoring systems are responsible for physically observing patients. Temperature, heart rate, blood pressure, and other similar parameters may provide various types of input data. In a data-gathering scenario, equation (1) (data collection) represents the process of gathering and normalizing the sensor data over a time interval, as per the prior suggestion 
Where the variable 
Equation (2) denotes the previous recommendation of 
Using the equation shown above, one may estimate the degree of uncertainty within the period for a sequence up to the point at which MDs are actively monitoring data from big data analytics in electronic health monitoring systems. The state learning technique validates the preceding intervention, which includes separating the data and features. The following example of uncertainty is investigated using the state learning lens below. The acquired sensing input data must be matched to the previous feature, with high accuracy and precision, in a timely sequence, to improve the decision accuracy of the e-health system's suggestions. This scenario pertains to the field of electronic healthcare. Figure 3 shows how to identify system uncertainty to guarantee the model's suggestions are reliable. The system determines forecast trust by comparing current data to historical suggestions. The approach also shows how the model splits data into unsure and specific states. Additionally, it shows how fresh data changes uncertainty over time. Comparing recent sensor data with historical recommendations is enough to implement uncertainty detection. It helps the system spot inconsistencies that indicate uncertainty. The system uses this data to improve its predictions, resulting in more accurate suggestions.

Uncertainty identification process.
The
The result of the state model learning is to identify data splitting, the intervention, and the recommendations sequence rely on 
Therefore,
The IoT incorporation evaluation is based on the sequence of recommendations. In this
Where in RDPM, the consecutive instances of 
The variable
The data augmentation and state model of the physical observation data of the above representation operate on the linear
PriorRecommendationcontrol

In Algorithm 1, using state learning to validate recommendations, manage replications, evaluate uncertainties, and compute previous recommendations, the pseudocode approach improves the decision accuracy of e-health systems. Data interrupts are minimized, overlap is maximized, and interrupting faults are minimized. In ever-changing e-health settings, the algorithm maximizes efficiency while reducing redundancy.
An examination of the various IoT incorporations and the decision accuracy of e-health system recommendations of metrics recommendation ratio and data interrupt ratio is being carried out. However, it is necessary to govern both to control existing analytical errors and reduce isolated data augmentations. The work offered provides the most effective data observation and analysis for managing large volumes of data. Let 
Where the variable
The meta-cognitive State Learning layer of the RDPM architecture is the most forward-thinking because it goes beyond sequence modeling. State Learning iteratively improves the model's reasoning process in real time in response to performance feedback, unlike RNNs and HMMs. The model operates using a patient's physiological status and its current trust in its parameters. This is because recommendation errors and data disruptions have affected the model's performance. In this strategy, the system learns to fix itself by making minor modifications when confidence is high and major recalibrations, such as reweighting data streams or broadening uncertainty bounds, when confidence is low. Meta-learning for sequential decision-making is learnt offline using a reinforcement learning model that rewards stability, precision, and correct uncertainty flagging. Meta-learning is rationally superior to adaptive models. After that, it works online to adjust the model's logic based on the circumstances. Turning off the State Learning module in ablation research prevented the system from contextually modulating its reaction to analytical errors and changing data patterns. Precision and suggestion ratio decreased significantly, and data interruptions increased sharply.
Figures 4 and 5 present the state learning illustration for

State learning for

State learning for
The states for
Based on the recommendation and update states, the validation is performed based on
In this condition, the variable
The state learning process regulates big data, which holds the replication condition. If
IoT-enhanced recommendation and decision precision
The inputs for the new suggestion are copies of the old data,

IoT-enhanced recommendation and decision precision.
The update and data 
The process of new recommendations generates two solutions namely
Following the above procedure, the decision precision of E-healthcare is computed through a sequence of evaluations as per the above equations for both 
IoT-Enhanced Recommendation and Decision Precision

A decision-making algorithm that generates a suggestion sequence and computes decision accuracy using IoT reports, uncertainty measures, and a matching procedure is shown in Algorithm 2. The algorithm checks for an IoT report, refreshes old data with new data, computes a new recommendation with uncertainty metrics, processes the matching process using the report, validates the new recommendation using state updates, generates a recommendation sequence, updates recommendations, computes decision precision, and outputs it if there is no interruption. The system analyzes both historical and current data to provide reliable recommendations. Pseudocode 1 represents the simplified proposed RDPM algorithm.
Pseudocode 1: RDPM Algorithm

Real-time data and dynamic state learning distinguish RDPM from HMMs and RNNs. The adaptive process in RDPM uses historical suggestions and new data to create context-aware changes in real time, unlike RNNs and HMMs. Because it can manage historical and real-time data in a feedback loop, RDPM is well-suited for e-healthcare applications, where data streams are continuous and adaptability is crucial.
Experimental result and performance analysis
The Human Activity Recognition Using Smartphones dataset tests the proposed RDPM (https://www.kaggle.com/datasets/uciml/human-activity-recognition-with-smartphones). Activities of Daily living recordings from 30 people carrying smartphones with inertial sensors on their waists were utilized to generate the HAR database. The following reasons make the dataset a valid and accurate benchmark: (1) accurate, real-time activity profiling has applications in geriatric care, rehabilitation, and chronic disease management; (2) HAR faces data interruptions and uncertain states like physiological monitoring; and (3) processing physiological data streams is computationally similar to processing high-frequency, multi-dimensional sequential inertial sensor data. If the RDPM can handle this demanding task, it will be applicable to other E-health scenarios. To prove the RDPM's worth in more generalized E-health settings, it is necessary to show that it can handle this difficult task.
In Figure 7, the matching and deviation factors and uncertain instances for different previous recommendation factors are analyzed.

Matching and deviation factor and uncertain instances analysis.
In Figure 7, the matching and deviation for

Recommendation %, consecutive, and isolated instances for different deviation factors.
An analysis of the recommendation % consecutive and isolated instances is presented in Figure 8. The recommendation % increases for
This part presents MATLAB-based performance evaluation results for the suggested model. The data from https://www.kaggle.com/datasets/uciml/human-activity-recognition-with-smartphones analyzes older people's input. This source provides information on 30 human subjects, of whom 13 (age >60) were selected to deliver activity recommendations. The data source contains 22 fields and 18 features under 116 training iterations. This analysis examines performance using the recommendation ratio, data interruption, precision, time delay, and error factors. The proposed method, RPDM, is compared with the following techniques: SBDA, 16 RTDRM, 21 and IBCN. 25
Recommendation efficiency ratio
This metric measures the system's efficiency in producing valuable results, and uses a proportion of data processing intervals
The comparative analysis for the recommendation ratio under different inputs and features is presented in Figure 9. In the proposed model, the

Recommendation ratio analysis.
Data interrupt
This statistic measures system value creation and makes a non-null patient recommendation using a fraction of

Interrupt analysis.
Precision
As shown in Figure 11, a comparative examination of precision is offered under various data inputs and attributes. The recommendation is retained in different
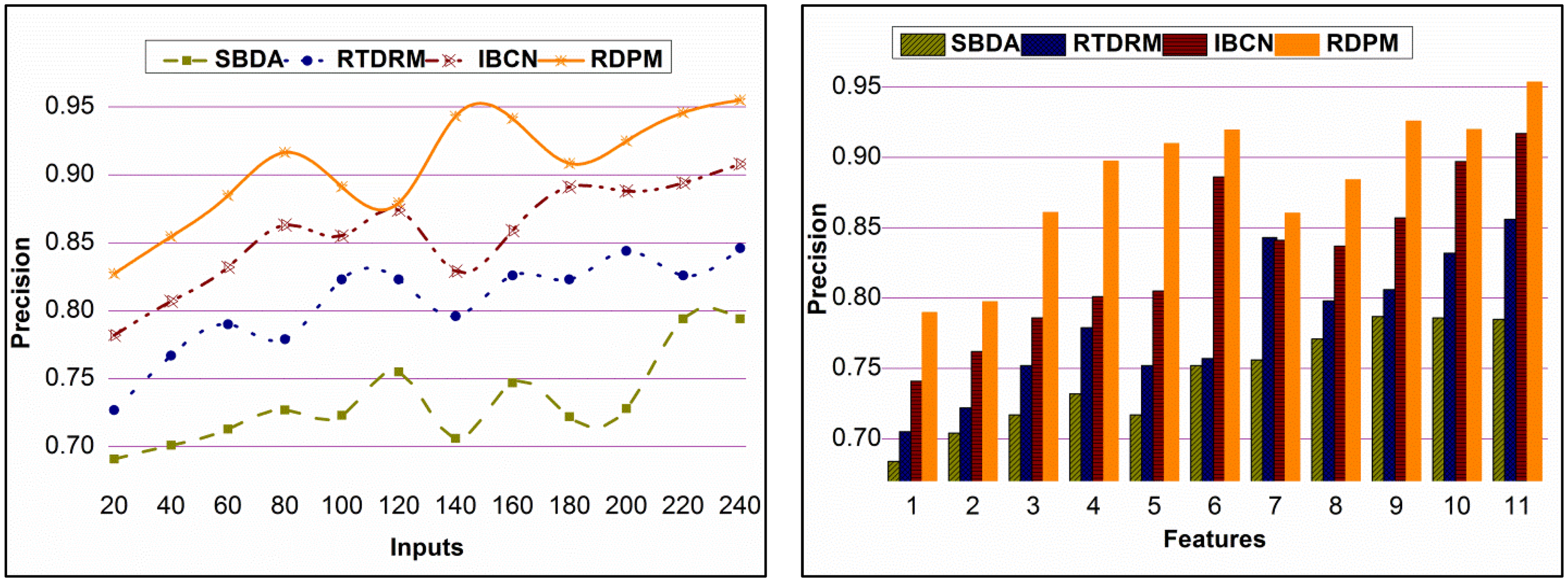
Precision analysis.
Time delay
The proposed model achieves lower time delays across different data inputs and features. The proposed model mitigates

Time delay analysis.
Error
The analysis for error under different data inputs and features is presented in Figure 13. The proposed model detects

Error analysis.
Performance analysis summary for inputs.

Performance analysis summary for features.

To validate the RDPM's clinical importance and allow a direct comparison with the literature, we used industry-standard binary classification metrics. This study includes “Positive” cases such as “alert for high blood pressure” and “suggest glucose intake,” indicating that a clinically significant incident requires intervention. They are both “good” situations. “Negative” describes a regular problem. Pairs of clinical doctors examined sensor and patient data to find the truth. The suggested RDPM model outperforms other clinical markers shown in Table 4. Patient monitoring relies on its high sensitivity of 0.92, which means it can identify actual clinical events while avoiding false negatives. For its extreme sensitivity. The model's overall discrimination is confirmed by its AUC-ROC of 0.96. Clinically, the RDPM outperforms state-of-the-art techniques in quality and reliability. Recommendation Ratio and Data Interrupt show system-level efficiency.
Clinical performance metric analysis.

Even though the study's core metrics—recommendation ratio, precision, and data integrity—are important for assessing the system's accuracy, the Quality of Experience (QoE) that electronic health monitoring systems provide to end users, such as patients and healthcare professionals, is more critical to their success. Beyond network-level Quality of Service (QoS), QoE measures user happiness and perceived quality. Due to the proposed RDPM framework's significant reductions in data interruptions (
QoE-aware system design methodologies from telecommunications and multimedia networks can be applied to e-health. The study “Estimating and synthesizing QOE based on QoS measurement for improving multimedia services on cellular networks using ANN method” uses Artificial Neural Networks to model the complex, non-linear relationship between technical QoS parameters, such as delay, jitter, and packet loss, and QoE. RDPM state learning can be viewed as an adaptive controller, similar to the IoT-cloud E-health system. The technology improves the health monitoring pipeline's “service quality” by reducing analytical errors and data flow pauses. In the healthcare industry, user trust and pleasure are crucial to a wonderful experience.
The term “QoE-aware self-tuning of service priority factor for resource allocation optimization in LTE networks” is helpful for future RDPM architecture improvements. Real-time quality-of-experience factors are used to prioritize traffic in this study dynamically. The RDPM's state-learning module can be enhanced to account for the QoE. The system can adjust resource allocation based on changes in network congestion or patient risk (
The model was also verified using the Diabetes dataset from the UCI Machine Learning Repository (https://www.kaggle.com/datasets/ealtintas/uci-machine-learning-repository-diabetes-data-set) to make sure that the RDPM is useful for clinical prediction tasks in general. There are 442 people with diabetes in this dataset which comprises age, gender, body mass index, average blood pressure, and six different serum levels. The objective variable is a numerical evaluation of the progression of the sickness one year subsequent to the establishment of the baseline state. Predicting a medical outcome using patient data with various variables is a frequent difficulty in medical AI regression, and this dataset exemplifies that complexity. These challenges aim to predict clinical outcomes from multivariate patient data. Even though the RDPM is a general framework, this validation primarily assesses how well it can be used to forecast clinical activities that incorporate physiological data. The UCI diabetes dataset was used to evaluate the model's ability to reliably forecast disease progression or a clinical event. To perform a full analysis, its performance was compared with that of the first comparison methods and a group of modern deep learning models (LSTM, Transformer, and TCN).
Table 5 shows that the RDPM outperforms earlier baselines (LSTM, Transformer, and TCN) and newer approaches (SBDA and IBCN) on crucial clinical prediction metrics such MAE and R2. Despite TCN's strength, the RDPM's integrated state learning and data ambiguity management yield superior accuracy. The D_I's preliminary results show that the RDPM must be able to perform consistently across data splits and endure simulated data disruptions to be used in the real world. These aspects show the RDPM's streaming versatility and durability.
Performance on clinical dataset.

Discussion
The RDPM improves electronic health monitoring system ideas’ accuracy, efficiency, and usefulness. IoT-based healthcare systems often lose data, obtain inaccurate data, and make data analysis mistakes. RDPM's ability to analyze past and present data and adjust recommendations is one of its strongest features and improves system decision-making with state learning instead of batch processing and static proposals. Because patient circumstances and sensor readings change fast, electronic healthcare systems must make prompt decisions. The IoT architecture allows real-time data processing and feedback loops that improve model predictions by connecting to the cloud. RDPM solves this problem with state learning, which compares novel and conventional concepts. In isolation, data augmentation creates redundant or consistent concepts. Adaptability allows the system make better decisions, helping doctors treat patients faster and more correctly. The proposed model beats state-of-the-art models in recommendation ratio, data interruption ratio, accuracy, and latency. The sensitivity data collected by IoT healthcare systems is often incorrect or absent. The model improved accuracy and suggestion ratio, which is crucial for real-time health monitoring and action. RDPM outperformed other approaches in the time delay research and its state-learning technology improved data flow, making cloud and IoT connections easier. Both companies will gain from shorter durations since medical personnel and patients will have better experiences. Since EHRs are becoming more intricate, real-time analysis of massive datasets is crucial for reliable outcomes. RDPM slows down in large healthcare networks with lots of data since it must process proposals repeatedly. Edge computing will reduce latency and speed up state learning, allowing the model to manage more users. The RDPM's clinical efficacy needs more study. The model is accurate in simulated environments and standard datasets, however unsupervised clinical scenarios must be tested. Due to the larger risk of mistake and change in real-world patient circumstances and sensor recordings, using feedback from healthcare professionals as the model is being implemented in the real world which can enhance it and overcome unexpected problems. The RDPM uses the IoT in constantly changing, aware environments to improve healthcare monitoring. Clinical and home-based health monitoring systems would benefit from being able to accept fresh data without errors or interruptions. Research and development are essential to ensure its reliability, growth, and therapeutic use.
Conclusion and future work
The RDPM asserts that EHR's make data management, recommendations, and accuracy better. The RDPM has fixed difficulties with analytical errors and segregated data growth by applying state-learning methods in the IoT cloud. Because of this, suggestions for how to treat patients will come faster and be more accurate. The model improves decision-making and system suggestions by constantly checking the data it gets and making sure that it doesn’t stop. RDPM may make the system able to make dynamic, on-the-fly judgments by adding real-time streams of hospital data. This would make the architecture extendable and reusable. It is possible that incorporating adaptive learning modules into the model might improve its performance over time. The model could be trained to respond dynamically to shifting patient parameters and sensor readings by implementing these features. With object-oriented frameworks, RDPM may be easily extended to massive, distributed IoT-cloud systems. Both the data-handling capabilities and the software's upgradeability will be improved as a result. By implementing these improvements, RDPM might be made more versatile and effective in many healthcare settings, opening up new possibilities for research and increased utilization of cutting-edge healthcare systems.
Footnotes
Acknowledgements
This research was supported by the Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R259), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. Ashit Kumar Dutta would like to thank AlMaarefa University for supporting this research under project number MHIRSP2025017. The authors extend their appreciation to the support provided by the University of Business and Technology, Jeddah 21448, Saudi Arabia.
Ethics approval and consent to participate
Ethical approval was not required for this study because it used only publicly available, anonymized data. The datasets employed were the Human Activity Recognition with Smartphones (https://www.kaggle.com/datasets/uciml/human-activity-recognition-with-smartphones) and the Kaggle – UCI Machine Learning Repository: Diabetes Dataset (![]() ). Both datasets are open-access resources and do not include any personally identifiable or patient-sensitive information.
). Both datasets are open-access resources and do not include any personally identifiable or patient-sensitive information.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the AlMaarefa University, Princess Nourah Bint Abdulrahman University (grant numbers MHIRSP2025017, PNURSP2026R259).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are openly accessible at the following links: https://www.kaggle.com/datasets/uciml/human-activity-recognition-with-smartphones and ![]()