
Abstract
Introduction
According to the World Health Organization (WHO; 2012),
Oral health is essential to general health and quality of life. It is a state of being free from mouth and facial pain, oral and throat cancer, oral infection and sores, periodontal (gum) disease, tooth decay, tooth loss, and other diseases and disorders that limit an individual’s capacity in biting, chewing, smiling, speaking, and psychosocial wellbeing.
As the above-mentioned definition suggests, a number of psychological factors seem to be implicated. At first, it is well known that the concept of quality of life (QoL) is “multidimensional and may be categorized within five dimensions: physical wellbeing, material wellbeing, social wellbeing, emotional wellbeing, and development and activity” (Felce & Perry, 1995, p. 51).
As oral health–related quality of life (OHRQoL) is “an integral part of general health and well-being,” it can be hypothesized that oral disorders may impair at least three of the QoL dimensions: the physical, emotional, and social well-being (Åstrøm, Haugejorden, Skaret, Trovik, & Klock, 2005; Sischo & Broder, 2011).
Studies have demonstrated the impact of oral health conditions on physical and psychosocial dimensions (John et al., 2004; Locker & Allen, 2007; Settineri, Rizzo, Liotta, & Mento, 2014), while there is a lack of scientific evidence about the link between OHRQoL and emotions. The majority of existing studies have focused exclusively on the relationship with dental anxiety (Kurer, Watts, Weinman, & Gower, 1995; McGrath & Bedi, 2004) and/or depression (Marques-Vidal & Milagre, 2006).
From a psychological point of view, all emotions play a fundamental regulatory role in human behavior (Gross, 1998), as they intervene in stressful situations, such as facing illness. Positive or negative feelings toward health problems may produce different outcomes (Bowman, 2001), suggesting a strict link between health and emotions. According to Kressin, Reisine, Spiro, and Jones (2001), the personality trait of “negative affectivity,” compared with the “positive affectivity” trait, is associated not only with a worse general physical health and worse health-related quality of life (HRQoL) but also with specific aspects of OHRQoL. On the contrary, an active coping and the trait of optimism seem to be related to dental health behavior, suggesting that the trait of optimism could be a determinant for both oral and general health (Ylöstalo, EK, & Knuuttila, 2003).
OHRQoL—as a part of a broad range of QoL domains—could have relationships with a wider emotional spectrum, from a functional affect expression to a psychopathological condition. In fact, emotions in clinical situations may become pathological, for example, when “there is a lack of balance between real and perceived danger” (Settineri, Mallamace, Muscatello, Zoccali, & Mento, 2013, p. 168).
Furthermore, as individuals during life span vary in their ability to regulate emotions and cope with stress (Wang & Saudino, 2011), it can be hypothesized that even the relationship between OHRQoL and emotions may differ across age, even if the existing literature seems to have neglected this point.
On the basis of these premises, the main aim of this study was to investigate the relationship between all emotions (Tension, Depression, Anger, Fatigue, Vigor, and Confusion) and the patient’s OHRQoL, with a particular attention for different life stages.
The hypotheses are the following:
Method
Instruments
For the evaluation, two questionnaires were used.
The POMS is a self-assessment mood scale consisting of 58 items (McNair, Lorr, & Droppleman, 1992). The participant has to indicate on a Likert-type scale from 0 (
The Oral Health Impact Profile (OHIP-14)—Italian version edited by Franchignoni et al. (2010)—consists of 14 items (Slade, 1997). As described by Meredith, Strong, Ford, and Branjerdporn (2016), each pair of item captures a specific dimension of the perception of the state of oral health: (a)
Procedure
The study was in conformity with ethical principles of research as it was conducted according to the Declaration of Helsinki. Each participant was informed in advance about methods and study aims and answered to the issued questionnaires only after signing informed consent. Data were collected in the period from January to May 2013. The administration was conducted by operators who had a brief training for the administration of psychological tests. The completion of the questionnaires required from 15 to 30 min, being two self-report measures. Data were analyzed using the Statistical Package for the Social Sciences (SPSS 17.0). To verify our hypothesis, we performed Pearson’s correlations, the ANOVA, and the Kruskal–Wallis test. The reliability of questionnaire used obtained a Cronbach’s alpha value of .93 for the OHIP-14 and .80 for the POMS.
Results
Sample
The whole sample consisted of 263 dental patients, all belonging to private dental surgeries of the center of Messina, Sicily (240,000 habitants). We included all participants with mild or moderate dental problems (gingivitis, cavities, plaque, sensitive teeth, halitosis, denture discomfort, etc.) according to the judgment of the dentist. For the analysis, we considered only the valid cases: 130 of them were females (56.8%) and 99 males (43.2%), for a total of 229 participants (see Table 1).
Descriptive Statistics of OHIP-14 and POMS.

To verify any difference between life stages, patients aged between 18 and 83 years (
Correlations Between POMS and OHIP-14.

Correlation is significant at the .05 level (2-tailed). **Correlation is significant at the .01 level (2-tailed).
Each dimension of OHIP-14 was referred to a pair of items (e.g.,
Hypothesis 1: Poor OHRQoL is linked not only to anxiety and depression but also to other mood states
To verify our first hypothesis, we performed Pearson’s correlation (see Table 3). All the POMS subscales were positively related to OHIP-14 items. Oral health dimensions were significantly related not only to the well-known constructs of
Differences in Oral Health Impact Profile Between Age Classes (OHIP-14).

Hypothesis 2: In different life stages, there are different OHRQoL degrees and different emotions
Second, we excluded any possible significant effect of gender by performing the Student t test for independent samples. On the contrary, the ANOVA revealed significant difference in the OHIP between age classes, as shown in Table 4.
Differences in Mood States Based on OH Classification.

In bold are statistically significant values (
Adult patients aged from 31 to 50 years had the higher scores and hence the worse oral health profile in almost all subscales, with the exception of
As regards POMS, there were no differences between males and females and between age classes. In the whole sample, 66 patients showed a level of
Hypothesis 3: Different OHRQoL degrees produce different expression of emotions, until psychopathology
According to the classification of the total score of OHIP-14, one hundred forty-four patients obtained a score lower than 14, which indicates the absence of oral health problems; 79 patients obtained a total score between 15 and 41, on the average; and only six patients obtained a score higher than 42, showing oral health problems. To verify our third hypothesis, we perform the nonparametric Kruskal–Wallis test (Table 4).
Patients who obtained a total score on the average (from 15 to 41) reported increased feelings of
Discussion and Conclusions
At first, as general result, all mood states subscales resulted positively related to oral health dimensions, with the exception for the
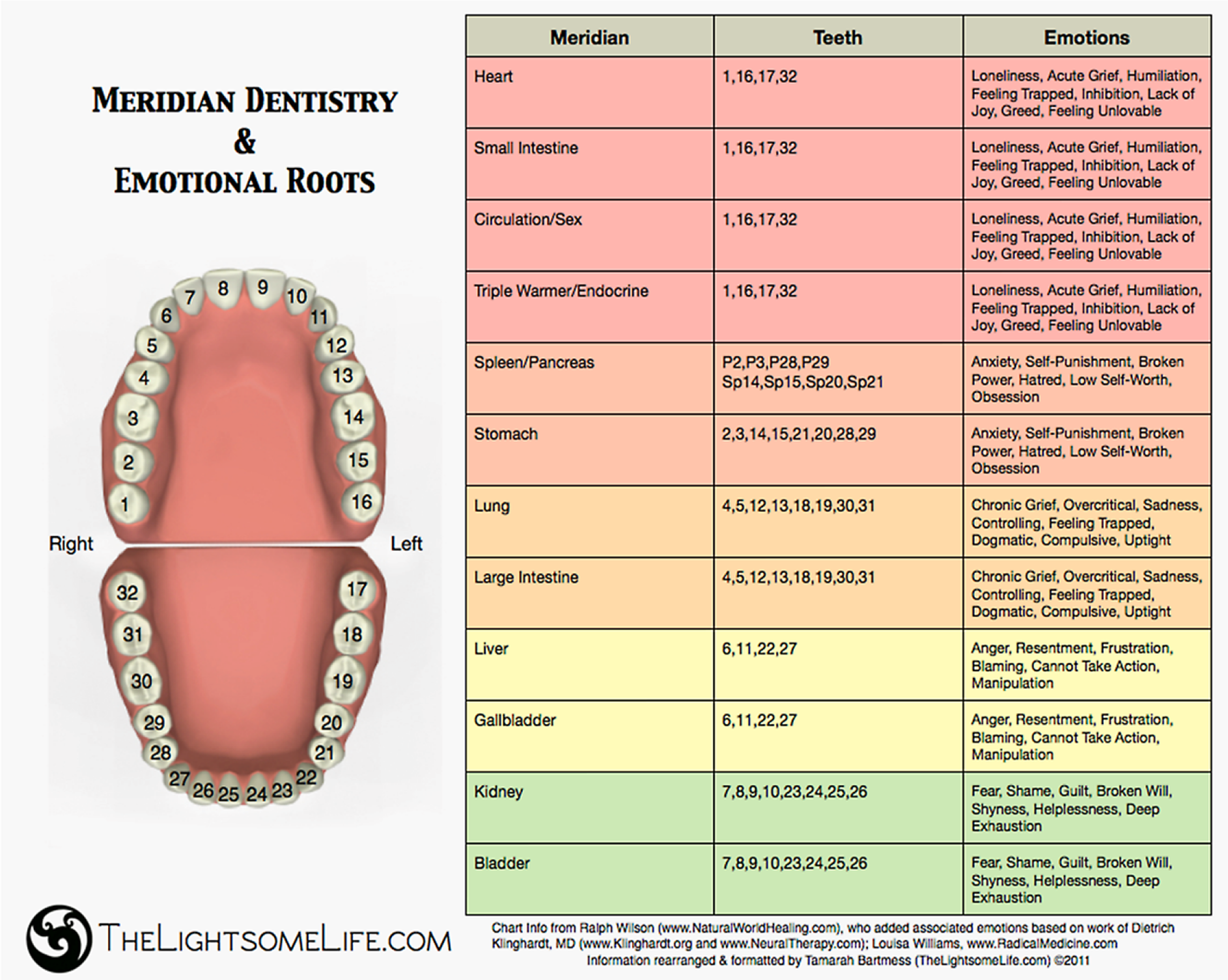
Meridian Tooth Chart.
Regarding the issue of age differences, we observed that the most significantly impaired oral health dimension for elderly patients is
It is also necessary to discuss issues surrounding the gender. Both in OHIP-14 and in the POMS, gender differences were not found. On the contrary, several studies have shown that males and females have a different perception of oral health status and oral health behavior in favor of females. Young woman “had better oral health behaviour and more factors associated with their oral health in comparison with young men” (Tada & Hanada, 2004, p. 104). At the same time, women perceived oral health as having a greater impact than men on their QoL in general, having both a greater negative or positive impact (McGrath & Bedi, 1999). Nevertheless, good general health habits correlate with higher oral health behaviors in males as well. For this reason, Fukai, Takaesu, and Maki (1998) hypothesized that “gender specificities in oral health depend on individual attitudes to oral health and dental utilization” (p. 187).
Although the findings have offered a first level of study of the psychopathology of emotions in dental patients, we must point out some limitations of the study. First, the sample showed the limits of generalizability, having been sourced in the same geographic region, because there are some evidence that oral health is influenced also by cultural background. For example, in Australia, those aged between 30 and 49 years showed the worst oral health profile scores; in the United Kingdom, instead, patients below 30 years showed the highest scores, reporting the worse oral health quality (Steele et al., 2004).
It would also be interesting to verify, both from the psychological and the dental point of view, whether the discomfort felt by the patient is congruent with the severity attributed by the dentist or whether there are differences attributable to the degree of invasiveness of the treatment.
In conclusion, the results of this study showed a significant relationship between the perception of the patient’s oral health and the mood states experienced. This knowledge may help to better understand the psychological mechanisms involved in the treatment compliance. The attention about the role of emotions in oral health life involves both psychologists and dentists, who have to safeguard the psychosocial, physical, and emotional well-being of dental patients. The teeth moreover have a symbolic value in the emotional life. The mouth, the main organ of our ability to express, can be read scientifically as an organ to cure, or symbolically as part of the body capable of recording and expressing our psychoemotional experience.