
Abstract
Introduction
A number of pathological osseous conditions require fixative and replacement therapies involving the use of medical implant appliances,1,2 and during the past several years, a number of materials, such as titanium and its alloys, have been used for the fabrication of these medical devices. Criteria such as an acceptable mechanical behaviour and biocompatible chemical composition to avoid adverse tissue reactions have been used to define an ideal implant material for orthopaedic surgery, but the overriding clinical requirement for these materials is to facilitate osteogenesis at the bone-implant interface, i.e. enhance osteoblast differentiation and function. 3 While the shape, length and diameter of a medical implant have been proposed to enhance clinical performances, the type of material and implant surface treatment and coating markedly influence its osteogenic properties. 4 Although many implant materials appear to be capable of enabling bone cell attachment, migration and growth (osteoconduction), their ability to stimulate the proliferation and differentiation of pluripotent mesenchymal cells into bone forming osteoblasts (osteoinduction) 5 is nevertheless still unclear. While titanium and a multitude of titanium alloys have been widely used and are generally regarded as the materials of choice due to their high biocompatibility and osteoconductivity,6,7 other promising implant coating materials, such as hydroxyapatite, bioactive glasses and biologically active agents, have also been used as coating materials in order to enhance bone-to-titanium (alloys) anchorage by facilitating their osteoinductivity.8–11 Understanding the mechanisms by which osteogenic cells respond to such materials is therefore of major importance in developing the most effective materials to promote functional osseointegration, which is required for the long-term success of implant surgery. 5
A number of commercially available implant surfaces have proven clinical efficacy (approximately 95% over 5 years).
12
Several attempts have been made to develop new implant surfaces and to study their
Tissue Responses to the Implant Material following Implant Placement
Within a few nanoseconds following implantation, the tissue responds to the implant material surface by allowing water molecules to make contact with the implant surface, thus forming a water layer surrounding the implant. 19 Surface properties of the implanted material have a major influence on the extent and specific interaction pattern of the material surface with this hydration layer, which in turn facilitates proteins and other molecules in the biological micro-environment to adsorb to the material surface.19,20 In the second stage, from seconds to hours after implantation, the material is subsequently covered by a thin layer of the extracellular matrix proteins; its conformation, orientation and composition are also likely to be affected by the implant material surface.21–23 The third stage involves the interaction of cells with the ‘surface’ of the implant via the adsorbed protein layer. The cell-protein bound surface interface, occurring from as short as minutes after and up to days following implant placement, initiates cellular adhesion, migration and differentiation, which occurs from a few hours to several days after implantation. 21 This stage is tightly regulated by numerous biological factors, including extracellular matrix proteins, cell surface-bound and cytoskeletal proteins, by chemical characteristics and topographies at the implant surface and by the released ions/products from the material. 24 The final stage of the body responses to the implant, which can last up to several decades, is the continuing development of the earlier stages, eventually resulting in the formation of functionally active mineralized bone tissue surrounding the implant. However, adverse responses, such as pathological inflammation, fibrous capsule formation and implant failure, can also occur during this stage.25–27 The future development of modern implant biomaterials is therefore aimed to minimize such effects as well as to promote rapid wound healing and implant-to-bone integration for the long-term success of an implanted device in the body, which is significantly dependent on the tissue biocompatibility at the site of implantation as well as the physicochemical properties of the material.
Both
Cellular Responses to Modern Implant Surface Modifications
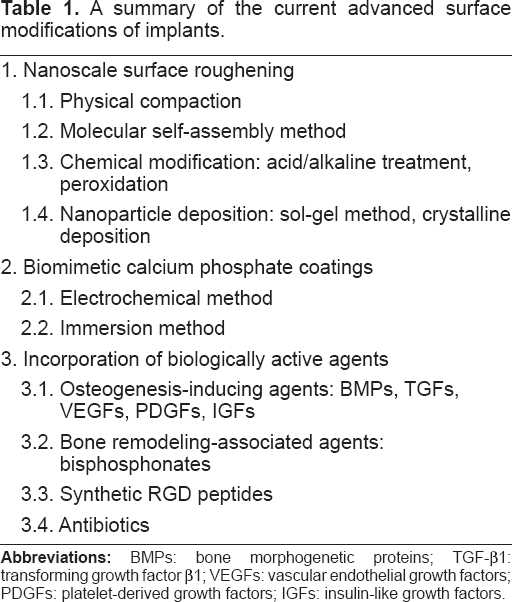
It is generally accepted that commercially pure titanium and its alloys are gold standard materials for medical implants, and their osteogenic properties can be enhanced by various modifications of the material surface in order to obtain osteogenic-inducing surface chemistry. A number of approaches have been considered in an attempt to achieve rapid and long term success of implant osseointegration. These modern trends include surface roughening at the nanoscale level, the use of biomimetic calcium phosphate coatings and the incorporation of biologically active agents into medical implants. A summary of the current advanced surface modifications of implants is shown in Table 1.
A summary of the current advanced surface modifications of implants.
Nanoscale surface roughening of medical titanium implants
It is well established that the roughness of implant surfaces plays a crucial role in the biological events following implant placement. It is possible that implant materials with a rough surface topography induce a three-dimensional growth of cells, supporting osteoblast adhesion and differentiation and promoting mesenchymal cells to differentiate along the osteoblast lineage by activation of several osteogenic-associated genes, e.g. core-binding factor 1 (Cbfa1), collagen, alkaline phosphatase, osteonectin, osteopontin and bone sialoprotein.33–38 It is thus believed that surface topography has a significant influence on the proliferation and differentiation of osteoprogenitor cells. Although presently available data are not consistent, the most commonly observed trends are that as surface roughness increases, the differentiation of osteogenic cells and their synthesis of extracellular matrix increase together with a concordant decrease in their proliferation. While micron-scale topographic modification of the commercially pure titanium surface has been accepted in the endosseous implant market due to its ability to facilitate osteogenesis at the bone-implant interface,39,40 increasing evidence has suggested that surface nanotechnology applications to the titanium implant may provide a promising approach to manufacture endosseous implant surface with a greater specific control of osteoblast differentiation and surrounding tissue fate, thus positively regulating implant osseointegration.
Nanotechnology involves materials that have a nanoscale topography or comprise nano-sized materials, which generally have a size range between 1 and 100 nm. Several methods have been proposed to create nanofeatures on titanium implant surfaces, for example, physical approach by compaction of nanoparticles (such as titanium dioxide (TiO2)), molecular self-assembly method, chemical modification by acid/alkaline treatment or peroxidation, nanoparticle deposition (such as sol-gel and discrete crystalline deposition).
41
While a number of methods have already been utilized to treat titanium orthopedic implants available commercially, most of nanotechnology-based surface modifications are currently undergoing the research and development process. A number of
It is not yet clear how nanoscale roughened topography influences its target cells. It is possible that nano-roughness topology regulates the interfacial forces that direct re-organization of cytoskeletal and cell surface receptor proteins. Moreover, nanoscale roughness could also modify the protein adsorption and conformation of integrin-binding adhesion molecules and thus modulating intracellular integrin pathway. This eventually results in controlling transcriptional events in the nucleus that guide target cells to undergo osteoblast differentiation, hence promoting implant osseointegration.
Although mechanisms by which nano-roughness enhances cell adhesion are not yet well understood, it has been suggested that initial attachment of cells to implant surfaces occurs through well-developed filopodia, directly exploring surface irregularities of the implant. 44 This is found to be primary adhesion structures in cell-to-extracellular matrix interaction. The roughness at nanometer thus provides positive guidance for osteogenic cells to attach, leading to enhanced cellular attachment via the selective attachment of osteoblasts to the implant surface. 44 This selective attachment process might result in the improvement of initial healing around medical implants with nanoscale roughened surfaces. On the other hand, cells attach to a smooth surface by focal adhesions around their surface membrane as primary attachment structures because repulsive signals from the environment lead to the retraction of filopodia back to the cell bodies. 44 This results in flattened cells with reduced cellular attachment to their surrounding substrates. Intriguingly, Prince and colleagues 49 reported that nanometer dimension fibers selectively enhanced osteoblast adhesion, whereas they decreased adhesion of smooth muscle cells, fibroblasts and chondrocytes. Such selective cell adhesion property therefore offers an advantage of a nano-roughened surface over its counterpart surface with respect to its potential to induce true direct bone contact but not unfavourable integration such as fibro-osseous intregation.
In addition to the positive effect of nanostructured surfaces on osteoconductivity, it has also been shown to facilitate the implant material osteoinductive property by enhancing osteoblast differentiation of stem/progenitor cells. Recent studies have shown strong cell responses of mesenchymal populations and osteoprogenitors to nanofeatures with increased levels of two important bone matrix proteins, osteocalcin and osteopontin.50,51 It is also suggested that progenitor cells are, in fact, more responsive to topography than more mature cell types and that they are actively seeking cues from their micro-environment.
52
Moreover, Oh and colleagues
53
have recently shown that the optimal dimension (approximately 70-100 nm diameter) of nanotube titanium oxide surface structures markedly drived differentiation of human mesenchymal stem cells into osteoblasts without the use of supplemented osteogenic-inducing factors
The roughness of the material also plays a significant role in the bacterial attachment process, presumably when the surface irregularities are comparable to the bacterial size and can protect them from unfavourable environment. In general, most commonly found bacteria range between 0.5 and 5 μm. Thus, it is possible that surface roughness on a scale much smaller than the bacteria would not be expected to influence the initial attachment. It is noteworthy that while osteoblastic cells are selectively adhered onto nanoscale surface, bacterial adhesion and growth on such surface is reduced. 54 Moreover, Mitik-Dineva and colleagues 55 reported that surface modification by etching, which resulted in a 70% reduction in the nanoscale roughness of the glass surface, significantly increase the number of bacteria adhering to the surface, suggesting that bacteria are sensitive to nanoscale surface roughness. Since the adhesion of bacteria to implant surfaces is also a key factor for the failure of implant osseointegration, this initial report suggests that such nanometer-roughness may provide favourable condition for successful osseointegration by preventing post-operative bacterial infection. Future comprehensive studies on the role of the nanotopography in bacteria are undoubtedly required to develop a clinically-successful medical implant system.
While a number of novel nanophase materials may be a promising alternative implant material, potential pitfalls or undesirable side effects associated with the use of nanomaterials in medical applications are also of important concern.
56
Nanostructured implants by physical compaction of nanoparticles could possibly be problematic due to loosening particles, resulting in an accumulation of nano-sized wear debris. Although the role of micron-sized wear particles in long term post-operative surgery is well-known, the effect of nano-sized debris generation in bone micro-environment is still poorly investigated. Thus, more detailed
Biomimetic calcium phosphate coatings on medical titanium implants
Delamination of calcium phosphate coating from the titanium implant surface causes a long term failure of osseointegration of the conventional plasma-sprayed hydroxyapatite-coated titanium implant. A new coating method, mimicking the natural process of bone mineralization, has been recently developed in order to avoid the drawbacks of such coatings. In this biomimetic approach, precipitation of calcium phosphate apatite crystals from simulated body fluids forms a coating on the titanium surface at room temperature.57,58 In order to enhance the deposition of coatings from aqueous solutions, a number of methods have been used. The electrochemical method involves the deposition of calcium phosphate by using a titanium cathode and a platinum anode to generate a current.59,60 This method is generally performed in acidic calcium phosphate solutions and gives rise to brushite coating formation which is subsequently converted into apatite by hydrothermal processing. Moreover, the electrochemical deposition conducted in simulated body fluid buffered at neutral pH can also produce a carbonated apatite coating directly on the titanium surfaces. 61 This method gives possible impeccable control of the calcium phosphate thickness on all types of complicated surfaces with a short coating time and high reproducibility and efficacy. 62 The second method involves immersion in simulated body fluid which allows calcium phosphate to precipitate onto titanium surfaces.57,58 This method involves the heterogeneous nucleation and growth of bone-like crystals on the surface of the implant. An implant is first treated with an alkaline in order to form titanium hydroxyl groups on the titanium surface, serving as nucleating points, followed by the crystal growth of the coating. In general, these subsequent events help promote the heterogeneous nucleation of the calcium phosphate.
Bone cell responses to biomimetically produced calcium phosphate materials have previously been shown. For example, these materials promote surface adhesion and proliferation of both osteoblastic and osteoclastic cells
The osteogenic effect of biomimetic calcium phosphate-coated implants has been assumed to be comparable to the conventional calcium phosphate coatings. Previous
Incorporation of biologically active agents into medical titanium implants
The surface of implants may be coated with osteogenesis-stimulating agents, such as growth factors, in order to accelerate angiogenesis and bone formation surrounding the endosseous implants. Members of the transforming growth factor β (TGF-β) superfamily (in particular bone morphogenetic proteins (BMPs) and TGF-β1), vascular endothelial growth factors (VEGFs), platelet-derived growth factors (PDGFs) and insulin-like growth factors (IGFs) are some of the most promising candidates for this purpose. For example, incorporation of BMP peptides into medical implants have widely been used to induce and sustain implant osseointegration.80–83 However, the biologically active product has to be released progressively, and not in a single burst, to the peri-implant micro-environment. Another method to obtain the BMP-incorporated surface is the utilization of a plasmid containing the BMP encoding gene. 84 Although this option may offer a better sustained release profile of the BMP, the outcome could nevertheless be limited due to the poor efficacy of transfecting plasmids into the target cells and the low expression/secretion level of the protein by the transfected target cells. In addition, continuing overexpression of the BMP by plasmid-transfected cells might not be advantageous after the completion of bone healing following implant placement. In addition to BMPs, much attention has currently been focused on the activation of angiogenesis, a key factor for rapid bone healing, by local and sustained delivery of plasmid DNA encoding for VEGF.85,86 Incorporation of VEGF gene into the implant surface could thus be a promising modern surface modification in this era medical implantology.
The implant surface could also be loaded with bone remodeling-associated bioactive agents. Incorporation of certain bone antiresorptive drugs, such as biphosphonates, might be beneficial in clinical application for patients lacking sufficient bone support, e.g. severely resorbed alveolar ridges. It has recently been shown that a chemically-associated biphosphonate zoledronate onto calcium phosphate compounds inhibits osteoclastic activity and thus reducing bone resorption.87,88 This might shift the balance of bone remodeling toward the formation of new bone
The integrins are a superfamily of cell adhesion receptors necessary for cell-to-cell and cell-to-matrix attachments, which play an important role in cell signalling and consequently control the biological activity of the cells. Therefore, the coating of titanium implant surface that contains binding sites for integrin receptors may potentially enhance peri-implant osteogenesis. Synthetic RGD peptides (Arg-Gly-Asp) coated onto the surface of implant materials increase bone-to-implant contact and newly formed peri-implant bone,
97
presumably by enhancing early cellular attachment to the implant surface. Moreover, the RGD coating has been shown to promote the bone-bonding ability of the coated implants.
98
The osteogenic role of RGD coating has also been demonstrated in
Interestingly, it has been demonstrated that coatings of implant surface by a combination of different bioactive molecules synergistically influence osteogenic events. For example, when RGD peptides coupled to a bisphosphonate were chemically adsorbed on titanium discs, adhesion and spreading of osteoblastic cells together with the formation of biomineralization were markedly enhanced.
102
Moreover, nanoscale roughened surfaces with RGD peptide coating provided an optimum surface for cell adhesion, spreading, and cytoskeletal organization, and also enhanced the expression of integrins.
45
However, the effect of combination coatings on new bone formation at the implant site
While several lines of evidence suggest the osteogenic-enhancing role of the RGD coating, a recent study has shown that RGD-coated hydroxyapatite discs significantly inhibited total bone formation as well as the amount of new bone formed at the peri-implant site. 103 It is noteworthy that RGD coatings, which are widely believed to promote cell-biomaterial interactions, could have a negative effect on hydroxyapatite implant performance, suggesting that for biomaterials that are highly interactive with the tissue microenvironment, e.g. hydroxyapatite, the ultimate effects of RGD peptides will depend upon how signaling from these peptides integrates with endogenous processes such as protein adsorption.
Antibiotic incorporation into implant coatings has also recently been introduced. Calcium-based coatings of an implant material can bind to antibiotics, such as cephalothin, carbenicillin, amoxicillin, cefamandol, tobramycin, gentamicin and vancomycin, which are able to release from the coating material. These releasing antibiotics also remain their bacterial inhibition property. 104 For example, tobramycin-supplemented coatings on titanium alloys release functionally active tobramycin that could suppresses growth of Staphylococcus aureus bacteria. 105 Moreover, recent reports suggest that antibiotics incorporated in polyester urethane coatings on implants significantly inhibit bacterial colonization and prevent bacterial resistance.106,107 The data suggest that certain antibiotics could be utilized to prevent post-operative bacterial infection and thus potentially enhancing implant osseointegration following implant placement. Moreover, future studies focusing on the drug release, method of drug incorporation and chemical structures of the antibiotic that facilitate their incorporation capacity, would be of utmost importance to develop a novel antibiotic-incorporated coating material for medical implants.
Conclusion
Studies of recent advanced surface modifications of implants have provided insight into potential benefits for endosseous implant therapy by positively controlling osteogenic responses of progenitor cells and thus stimulating both